Pediatric heart patients exposed to plastic chemicals during cardiopulmonary bypass
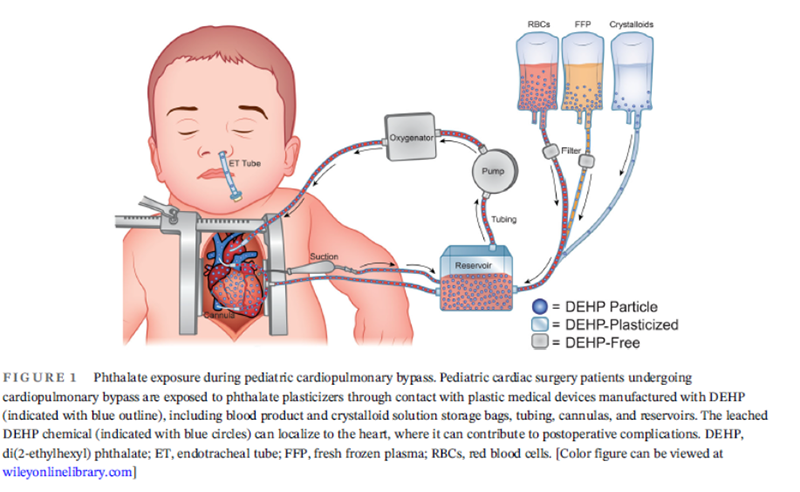
Image credit: Transfusion, April 2024
Children undergoing cardiac surgery using cardiopulmonary bypass are exposed to high levels of plastic chemical additives called phthalates, including DEHP, according to the largest single center study to date to measure this exposure. The findings were authored by a multi-disciplinary group from Children’s National Hospital and appear in the journal Transfusion.
What is it?
Di(2-ethylhexyl) phthalate (DEHP) is one of the most commonly used plasticizers in polyvinyl chloride (PVC) plastics, making up 40% to 80% of the finished weight of medical-grade tubing and blood storage bags. The study’s primary goal was to quantify three aspects of pediatric cardiac surgery: the phthalate exposure with and without cardiopulmonary bypass (the heart and lung machine), the time it takes for phthalates to clear after surgery and any correlations between higher phthalate exposures and postoperative complications.
The authors suggested that, like infants in the NICU exposed to various medical equipment, children on cardiopulmonary bypass are likely exposed to significant DEHP levels from blood products, bypass circuit components, and endotracheal tubes, potentially impacting postoperative outcomes.
Why does it matter?
Despite daily phthalate exposure in the general population, studies link high phthalate levels to developmental delays in language and motor skills. Phthalates accumulate in the hearts of infants undergoing umbilical catheterizations or blood transfusions. This is worrisome as even low-dose environmental exposure correlates with higher risks of overall and cardiovascular-related mortality.
Knowing these risks exist, it is important to understand these exposures, what causes them and implement measures to mitigate them, safeguarding medically fragile children. Regulatory actions in NICUs have reduced DEHP-containing plastics, yet no such efforts have been made for children on cardiopulmonary bypass.
The study also found some associations between postoperative complications and higher levels of phthalates, especially in younger children. They write, “it is plausible that a combination for risk factors (young age, longer CPB duration, increased phthalate exposure) collectively contribute to these complications.” More research is needed to understand the association and the impact of phthalates on how children recover from surgery.
Children’s National leads the way
The study involved 110 pediatric patients undergoing 122 cardiac surgeries at Children’s National, marking the largest single-center investigation into phthalate exposures in cardiac surgery. Led by a multidisciplinary team, including divisions of Transfusion Medicine and Cardiac Surgery, along with researchers from the Sheikh Zayed Institute for Pediatric Surgical Innovation, the study’s findings are some of the first to quantify that pediatric cardiac surgery patients are exposed to greater levels of these phthalate chemicals from plastic medical products, with increasing exposure the longer they require cardiopulmonary bypass. This is especially true when the bypass uses a prime based on red blood cells.
What’s next
The teams are exploring strategies to minimize chemical exposures, such as:
- Using freshly donated blood products (made possible at Children’s National by the unique on-site Blood Donor Center).
- Storing blood in DEHP-free storage bags prior to use when possible.
- Increasing use of cell-saver equipment, which washes red blood cell products and removes extracellular contaminants.
- At Children’s National, cardiac surgeons prioritize the use of recently collected, washed red blood cells in cardiopulmonary bypass cases, especially for younger and/or smaller patients.
“These exposures will affect patients undergoing pediatric cardiac surgery at any institution,” says first author Devon Guerrelli, M.S. “But we hope understanding what’s causing the exposures will help operating rooms around the United States take immediate small steps, like using washed red blood cells, to begin mitigating these exposures as soon as possible.”
Senior author Nikki Posnack, Ph.D., adds that the implications of phthalates on health are tremendous. “Studies have shown that heightened phthalate exposure increases your risk of all-cause and cardiovascular mortality,” she said. “Now is the time to support research efforts to understand how plastic chemicals damage the heart and to investigate strategies to reduce their overall impact.”
Read the study:
Prevalence and clinical implications of heightened plastic chemical exposure in pediatric patients undergoing cardiopulmonary bypass