Nikki Posnack, PhD, named as Foglia-Hills Professor of Pediatric Cardiac Research
Dr. Posnack joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair.
Children’s National Hospital has appointed Nikki Posnack, PhD, as the Foglia-Hills Professor of Pediatric Cardiac Research.
Dr. Posnack serves as a principal investigator for the Sheikh Zayed Institute of Pediatric Surgical Innovation at Children’s National. Her laboratory is part of both the Children’s National Heart and Lung Center and the Sheikh Zayed Institute.
The big picture
Dr. Posnack joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful to generous donors who have altogether funded 51 professorships.
Professorships support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and the donor’s commitment to advancing and sustaining knowledge.
Why it matters
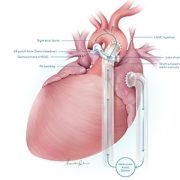
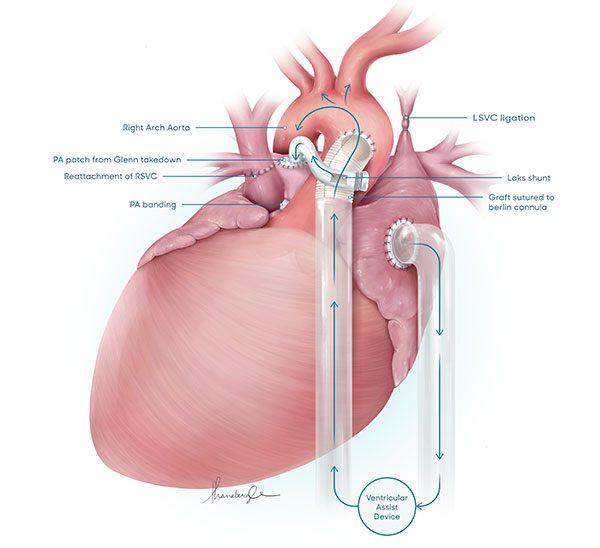
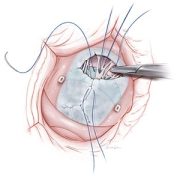
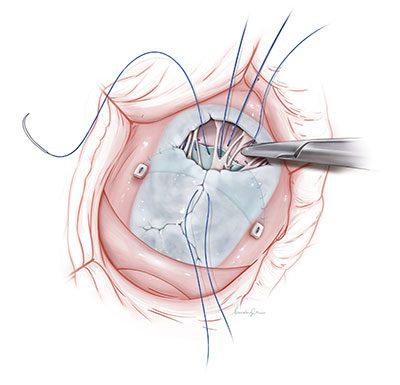
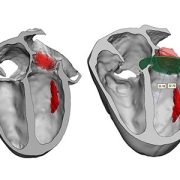
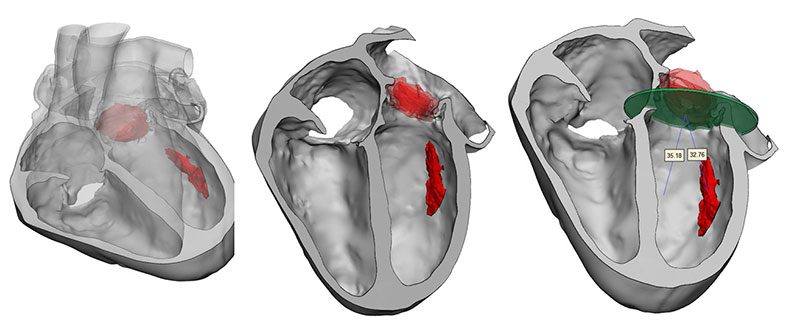
Dr. Posnack’s research is transforming our understanding of pediatric cardiac health. She leads a multidisciplinary team conducting pioneering studies on cardiac electrophysiology, environmental exposures during heart surgery and personalized treatments for children. Notably, the team’s findings on plastic chemical exposure during cardiopulmonary bypass operations are influencing clinical care for young patients with congenital heart disease.
“I am deeply honored to be named Foglia-Hills Professor of Pediatric Cardiac Research,” Dr. Posnack says. “It is a powerful opportunity to amplify the mission of my lab: to help make cardiac care safer, less invasive and more effective for kids. The role will help accelerate discovery and bring meaningful innovations from the lab to bedside.”
Moving the field forward
Paul and Barbara Hills and Vincent and Patricia Foglia established this endowed professorship over a decade ago. Through their vision and generosity, they are ensuring that Dr. Posnack and future holders of this professorship will launch bold, new initiatives to rapidly advance the field of pediatric cardiac research, elevate our leadership and improve the lifetimes of children with special hearts.
“This professorship shows the incredible foresight of the Foglia and Hills families, who believe in driving progress through research,” says Wayne J. Franklin, MD, MBA, senior vice president of the Children’s National Heart and Lung Center. “Dr. Posnack is a true leader in the field, and this support will help her continue to push the boundaries of what’s possible in caring for patients with heart disease.”














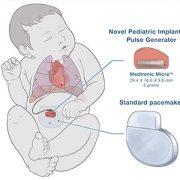








 Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.
Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.