Bladder cancer’s unique bacterial “fingerprint”
Michael H. Hsieh, M.D., Ph.D.
Decades ago, researchers thought that the native bacteria scattered throughout the human body—such as in the gut, the oral cavity and the skin—served little useful purpose. This microbiota, whose numbers at least match those of the cells in the body they live on and in, were considered mostly harmless hitchhikers.
More recently, research has revealed that these natural flora play key roles in maintaining and promoting health. In addition, studies have shown that understanding what a “typical” microbiome looks like and how it might change over time can provide an early warning system for some health conditions, including cancer.
Now, a small, multi-institutional study conducted in experimental models suggests that as bladder cancer progresses, it appears to be associated with a unique bacterial fingerprint within the bladder—a place thought to be bacteria-free except in the case of infection until just a few years ago. The finding opens the possibility of a new way to spot the disease earlier.
Bladder cancer is the fourth-most common malignancy among U.S. men but, despite its prevalence, mortality rates have remained stubbornly high. Patients often are diagnosed late, after bladder cancer has advanced. And, it remains difficult to discern which patients with non-invasive bladder cancer will go on to develop muscle-invasive disease.
Already, researchers know that patients with grade 4 oral squamous cell carcinoma, women with increasingly severe grades of cervical cancer and patients with cirrhosis who develop liver cancer have altered oral, vaginal and gut microbiomes, respectively.
New technological advances have led to identification of a diverse community of bacteria within the bladder, the urinary microbiome. Leveraging these tools, a research team that includes Children’s National Health System investigators studied whether an experimental model’s urinary bacterial community changed as bladder cancer progressed, evolving from a microbiome into a urinary “oncobiome.”
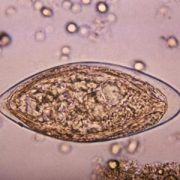
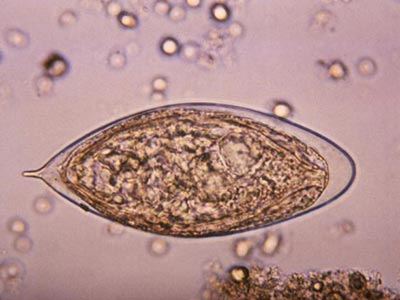
To test the hypothesis, the research team led by Michael H. Hsieh, M.D., Ph.D., a Children’s urologist, exposed an experimental model of bladder cancer to a bladder-specific cancer-causing agent, n-butyl-n-(4-hydroxybutyl) nitrosamine (BBN). Bladder cancers induced by BBN closely resemble human cancers in tissue structure at the microscopic level and by gene expression analyses. Ten of the preclinical models received a .05 percent concentration of BBN in their drinking water over five months and were housed together. Ten other experimental models received regular tap water and shared a separate, adjacent cage.
Researchers collected urine samples ranging from 10 to 100 microliters at the beginning of the longitudinal study, one week after it began, then once monthly. They isolated microbial DNA from the urine and quantified it to determine how much DNA was microbial. All of the bladders from experimental models exposed to BBN and two bladders from the control group were analyzed by a pathologist trained in bladder biology.
According to the study published online July 5, 2018, by the biology preprint server Biorxiv, they found a range of pathologies:
- Five of the experimental models that received BBN did not develop cancer but had histology consistent with inflammation. Three had precancer on histology: urothelial dysplasia, hyperplasia or carcinoma in situ. Two developed cancer: invasive urothelial carcinomas, one of which had features of a squamous cell carcinoma.
- The experimental model that developed invasive carcinoma had markedly different urinary bacteria at baseline, with Rubellimicrobium, a gram negative organism found in soil that has not been associated with disease previously, Escherichia and Kaistobacter, also found in soil, as the most prominent bacteria. By contrast, in the other experimental models the most common urinary bacteria were Escherichia, Prevotella, Veillonella, Streptococcus, Staphylococcus and Neisseria.
- By month four, the majority of experimental models exposed to BBN had significantly higher proportion of Gardnerella and Bifidobacterium compared with their control group counterparts.
“Closely analyzing the urinary bacterial community among experimental models exposed to BBN, we saw distinct differences in microbial profiles by month four that were not present in earlier months,” Dr. Hsieh says. “While Gardnerella is associated with the development of cancer, Bifidobacterium has been shown to exert antitumor immunity, and its increasing abundance points to the need for additional research to understand its precise role in oncogenesis.”
Dr. Hsieh adds that although the study is small, its findings are of significance to children who are prone to developing urinary tract infections (UTIs), including children with spina bifida, due to the association between UTIs and bladder cancer. “This work is important because it not only suggests that the urinary microbiome could be used to diagnose bladder cancer, but that it could also perhaps predict cancer outcomes. If the urinary microbiome contributes to bladder carcinogenesis, it may be possible to favorably change the microbiome through antibiotics and/or probiotics in order to treat bladder cancer.”
In addition to Dr. Hsieh, co-authors include Catherine S. Forster, M.D., M.S., and Crystal Stroud, of Children’s National; James J. Cody, Nirad Banskota, Yi-Ju Hsieh and Olivia Lamanna, of the Biomedical Research Institute; Dannah Farah and Ljubica Caldovic, of The George Washington University; and Olfat Hammam, of Theodor Bilharz Research Institute.
Research reported in this news release was supported by the National Institutes of Health under award number R01 DK113504 and the Margaret A. Stirewalt Endowment.