Straightening out testicular torsion care
A new collaborative accelerated care pathway for testicular torsion assessment and treatment may save critical time between diagnosis and intervention.
The clock starts ticking for a child with testicular torsion as soon as the pain starts. To increase the likelihood of successfully salvaging the twisted testicle and spermatic cord, surgical intervention – which involves restoring blood flow to the testis – should ideally occur within six hours from the onset of pain.
That’s six hours for a parent to identify that there is a problem, bring a child to the emergency department (ED) and go through all the steps required to get the child to the operating room. This process starts with an emergency physician, who probably doesn’t see many cases of this relatively rare condition, being able to identify the potential issue and contact the pediatric urologist on call. Next, diagnostic imaging orders need to be placed and actual imaging needs to occur for the diagnosis to be made. Finally, the patient needs to be moved to the pre-operative area, assessed by the anesthesia team and then taken to surgery.
In April 2016, the Division of Urology at Children’s National launched a new, accelerated care pathway for testicular torsion assessment and treatment that was developed collaboratively with the Emergency Department, Diagnostic Imaging and Radiology, the Department of Anesthesiology, and the peri-operative and operating room team.
“What stood out to us when we looked at the total time from identifying the problem to getting to surgery, was the length of time from when the diagnosis was made in the emergency department to the operating room,” says Tanya Davis, M.D., a pediatric urologist who led this new initiative along with Harry Rushton, Jr., M.D., chief of the Division of Urology. “It was an area where we could easily identify and streamline the process to accelerate the time for a patient to get from arrival in the ED to the surgical suite.”
Now, when a patient presents in the emergency department with the symptoms of testicular torsion, there is a straightforward path mapped out for the physician. “Who you need to talk to, how to reach them, relevant phone numbers, details on when to communicate to the attending physician, the ideal order of activities, the ability for residents to quickly transport the patient rather than waiting for hospital transport to surgery, and, most important, making it clear to everyone involved that this condition is a true emergency when every second matters,” Dr. Davis adds.
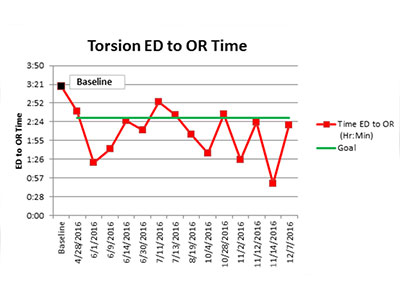
Analysis of the streamlined care pathway, which emphasizes communication that the condition is a true emergency, has improved time from ED to OR within target ranges.
Since the initiative’s launch, 21 cases, from referrals and direct diagnosis, have come into the ED. The new protocol is working efficiently, reducing the mean time from the ED to the OR by more than an hour, now averaging below the team’s target goal of less than 2.5 hours from ED arrival to the OR.
Though salvage rates have not improved yet, the team will continue to collect data and monitor the impact of the accelerated pathway. Additionally, Dr. Davis says that a significant need remains for referring emergency and primary care physicians, as well as parents, to understand the condition and its need for urgent treatment. Children’s National urologists are developing handouts for both physicians and families to help raise awareness.
The hope is that more general knowledge of testicular torsion will allow parents, primary care doctors and emergency department staff to expedite diagnosis when a child complains of scrotal pain or has visible discoloration, further reducing the time from onset of pain to successful intervention. With such a short window of time for treatment, the accelerated care pathway is showing promising results.