Transitional urology bridges care for those with pediatric-onset conditions

A hot topic at national urology meetings is how to transition patients with pediatric-onset urologic conditions as they grow into adults. Michael Hsieh, MD, PhD, is leading the way in the U.S. by serving as a bridge for patients at the first dedicated transitional urology program in the mid-Atlantic region. The Clinic for Adolescent and Adult PedIatric OnseT UroLogy (CAPITUL) is a joint venture between Children’s National and George Washington University Hospital that started two years ago.
What’s most unique about the clinic is that Dr. Hsieh has a foot in both the pediatric world of urology and one in the adult world, with clinical privileges at both institutions. He sees the full span of pediatric urology patients, including expectant moms with fetuses that have suspected urologic anomalies to adults who may have congenital conditions that require follow-up. However, he sees more teenagers and young adults than his urology colleagues both at hospitals.
The clinic’s patients have included a 19-year-old man with multiple urethrocutaneous fistulas after failed hypospadias repairs, a 25-year-old woman with cloacal exstrophy and continent urinary diversion with a urinary tract infection and stones, and a 25-year-old man with spina bifida with incontinence urethral erosion from an indwelling catheter.
A number of significant urological conditions until recently led to premature death because of medical complications, Dr. Hsieh says. Today, 90 percent of spina bifida patients live past the age of 30. “There’s a synchronized wave of patients who are all now young adults with spina bifida, and they are facing issues of reproduction and sexuality,” Dr. Hsieh says. “These are issues that pediatric urologists generally speaking are not comfortable in managing. It makes sense: It’s been many, many years since they did that type of urology.”
The program is specifically following this transitional group on conditions that are long term and that may affect fertility, such as cancer and varicoceles.
One in five teenage boys have varicoceles, or varicose veins on the scrotum. “The relationship between having varicocele as a teenager and infertility as an adult is not clear, so we felt it important to include this diagnosis in the transitional program so we can follow these patients long term and monitor their testicular growth,” Dr. Hsieh says.
Proof that the program’s working
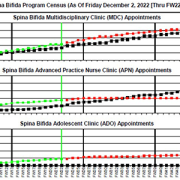
Dr. Hsieh tracks the messages from colleagues referring patients from one institution to the other. “Unfortunately, some patients and families—for a range of issues—fall through the cracks, so it is really important to have that direct link. If we didn’t have the program set up as it is, there would be fewer successful transitions between institutions,” he says.
Another way Dr. Hsieh knows the program is working is because of the uptick in adolescent and young adult patients in his practices at Children’s and at GW.
Dr. Hsieh says the optimal time to begin transition is at age 12, when the team makes the patient and family aware of the transition policy. From ages 14-16, it’s time to initiate the health care transition plan and begin discussing the adult model of care. By age 18, Dr. Hsieh recommends the transition to adult care, and by ages 23-26, patients are integrated into adult care.