

Surgical Innovation


“This project is exciting as it targets more precise surgery with improved safety in terms of decreased radiation,” says Matthew Oetgen, MD, division chief of Orthopaedic Surgery and Sports Medicine at Children’s National.
What if surgeons could fix a child’s hip with pinpoint accuracy – using fewer X-rays and cutting-edge robotics? That’s the promise of a new National Institutes of Health funded project combining 3D imaging and robotic technology to improve the treatment of slipped capital femoral epiphysis (SCFE), a condition that affects the hip joint in growing children.
Right now, orthopedic surgeons place screws by hand using 2D X-ray images to guide them. To see the screw from different angles, they have to move the X-ray machine around. “The screw must be placed near the center of the femoral head, but not penetrate it,” says Kevin Cleary, PhD, associate director of engineering at the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). This process takes time and can increase the amount of radiation the patient receives.
Even though better tools like 3D imaging and surgical robots exist, they aren’t used together in current surgical practice. “Individual procedures have nuances that require their own validated workflows,” says Tyler Salvador, a research engineer at Children’s National Hospital. In other words, each type of surgery is different, and doctors need proven steps before using new technology in the operating room.
This project brings together low-dose 3D X-rays from nView with a small surgical robot called Micromate™ to help place screws more precisely during SCFE surgeries. “Our research group has been developing robotics, imaging, and related technologies to improve surgical procedures,” says Dr. Cleary. While these tools exist separately, putting them together in one system focused on bone surgery is new. Tyler Salvador adds, “This will provide a complete solution for precision SCFE implant placement and verification.”
“This project is exciting as it targets more precise surgery with improved safety in terms of decreased radiation,” says Matthew Oetgen, MD, division chief of Orthopaedic Surgery and Sports Medicine at Children’s National. “This is a paradigm-shifting effort that will improve outcomes while improving safety which is the holy grail of translational clinical research. It embodies the goal of the SZI — combining technical expertise with surgical leadership to improve outcomes in pediatric surgery.”
Children’s National is unique because the Sheikh Zayed Institute combines research and clinical care in one place. “Having the labs right inside the hospital helps us work closely with doctors,” says Salvador.
Together, this work is paving the way for safer, faster and more precise surgeries for children with hip problems. By combining advanced imaging and robotics, the team at Children’s National is helping shape the future of pediatric orthopedic care. In addition to this robotic hip pinning project, the Children’s National team is also behind two additional groundbreaking projects including robotic gallbladder removal and a kidney surgery initiative.
This project has been funded in whole with federal funds from the National Institutes of Health under Contract No. R01EB035559.
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success.
A novel immunotherapy approach that involves training autologous T cells derived from peripheral blood mononuclear cells (PBMCs) has shown early signs of safety and efficacy in a small pre-clinical model. The approach, pioneered by researchers within the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital, may have future implications for the treatment of intractable pediatric solid tumors such as neuroblastoma.
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success. There is an urgent need for innovative strategies to effectively target these tumors.
This study presents another approach to cell therapy that collects peripheral blood mononuclear cells from the patient and teaches them to target and eliminate solid tumor cells through exposure to similar tumor cells in a controlled laboratory setting. The cells are then primed to find and attack the solid tumor cells when reintroduced, an approach known as adoptive immunotherapy.
The authors note that more well-established modalities such as CAR-T and TCR-T therapies have also made significant advances and demonstrate clinical promise at battling cancers such as neuroblastoma. However, the approach presented in the paper offers early promise of an additional potential strategy, especially in a context “where simplicity, speed and safety are priorities.”
By using small molecule treatments, the authors induce an immunogenic response in neuroblastoma tumor cells, making them more recognizable and attackable by immune cells. Ex vivo training of PBMCs with treated neuroblastoma cells exhibited strong tumor-killing activity.
The authors highlight a few key differences of this approach versus existing adoptive cellular therapies. The method “is technically straightforward, requiring only small tumor samples and peripheral blood mononuclear cells (PBMCs), and avoids the need for the complex genetic engineering intrinsic to CAR-T and TCR-T manufacturing,” the authors write. This method leverages ex vivo tumor cell modification, which may mitigate systemic toxicities. “Additionally, because our approach is not limited to a few surface antigens, it may expand the repertoire of actionable tumor-associated targets.”
Children’s National is a leader in the development of cell therapies for a wide range of pediatric conditions, including pediatric cancer, HIV/AIDS, sickle cell disease and others.
This research is the latest development in a decade-plus of focused research in adoptive immunotherapy within the Center for Cancer and Immunology Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
The authors write that there are several critical areas for future research to advance this approach, including a need to understand the specific T cell component and receptors involved in recognizing tumor antigens. They will also need to explore the longevity of the trained T cell response including studies of the memory and persistence of trained PBMCs to ensure lasting anti-tumor effects. Finally, the team will explore the risk of T cell exhaustion, which could reduce the effectiveness of the therapy over time.
Though work remains, the authors note, “Our findings lay the groundwork for developing this approach into a viable therapy for neuroblastoma and possibly other solid tumors as well.”
Read the full study: Trained autologous cytotoxic T cells derived from PBMCs or splenocytes for immunotherapy of neuroblastoma in Frontiers in Immunology.


The multi-disciplinary team who implanted the first AVEIR leadless pacemakers at Children’s National.
Two new devices being used in adults with heart rhythm disorders — atrial and dual chamber leadless pacemakers and extravascular defibrillators — were successfully implanted in pediatric patients for the first time at Children’s National. These devices represent the latest technology in pacing and defibrillating the heart to maintain its rhythm. Though they are smaller in size, have fewer complications and longer battery life than most of the devices currently available for young patients, they have not been available for use in these younger patients until recently.
“For the first time, we’re bringing these devices that are smaller, smarter, less painful and more flexible to children and teenagers who can really benefit from them,” says Elizabeth Sherwin, MD, a pediatric cardiologist and electrophysiologist at Children’s National who led the teams completing these minimally invasive procedures.
Offering implantation of these devices gives more children and adults with congenital heart disease access to the latest technologies in implantable heart rhythm devices, which may offer unique benefits for these groups.
Abbott AVEIR dual chamber leadless pacemaker is the newest FDA approved leadless pacemaker. It uses electricity to maintain heart rhythm and can be used to pace both the top and bottom chambers of the heart, which is particularly important for pediatric and adult congenital patients. These devices also:
Dr. Sherwin says that the minimally invasive procedure and the lack of leads on these devices are particularly key for younger people because these factors remove or reduce the risk of complications commonly experienced with pacemakers in children. There is a reduced risk of bleeding, infection, lead movement or fracture, and long-term problems with the veins. Even better, because they are placed directly in the heart, there are no scars on the chest or visible signs of a pacemaker present.
Medtronic Aurora EV-ICD is an extravascular implantable cardioverter-defibrillator (ICD), which is implanted under the skin (subcutaneous) with a generator on the left chest wall and a lead that goes under the breastbone (sternum). The design includes:
For both of these newer devices, the patient’s size, weight and medical history will help determine if they are a good candidate.
The Electrophysiology team is the first and only pediatric and congenital cardiology team trained to implant AVEIR leadless pacemakers and the Aurora EV-ICD for eligible individuals in the mid-Atlantic region. Dr. Sherwin, Charles Berul, MD, and Tom (Nak) Choi, MD, are trained to provide these procedures for people in Washington, DC, Virginia and Maryland. For both devices, Children’s National is among only a handful of children’s hospitals in the U.S. with the training and expertise to offer access to these technologies.
“This is a game-changer for kids with rhythm disorders and adults with congenital heart disease,” Dr. Sherwin says. “We are really excited to be among the first to offer these options for patients who need them.”

“Healthcare is moving very fast. And what often happens in adults, also happens in children. Unfortunately, most of the research is directed initially at adults, and then whittles down to children. At Children’s National, we’re trying to turn that around. We’re trying to do research for children that will expand its way up to adults, turning it on its head.”
Anthony Sandler, MD, senior vice president and surgeon-in-chief, Joseph E. Robert Jr. Center for Surgical Care, and director of the Sheikh Zayed Institute for Pediatric Surgical Innovation highlighted the exciting research and innovation happening at Children’s National – including demonstrating a technology, led by Raj Shekhar, PhD, that uses real-time imaging with augmented reality to project live ultrasound visualization of a patient within the surgeon’s field of view. This enhances surgical precision and ultimately supports positive patient outcomes.
This conversation was a part of Axios’ inaugural Future of Health Summit – an event bringing together the top voices in healthcare, policy and technology to explore the biggest challenges and innovations shaping the future of medicine.

Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
The Nursing Sponsored Keynote Lecture by Vincent Guilamo-Ramos, PhD, MPH, LCSW, ANP-BC, PMHNP-BC, FAAN, explored “Redesigning the U.S. broken health system.” He offered an urgent and inspiring call to reimagine pediatric care by addressing social determinants of health.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD
“Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD
“Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey
“Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
MENTORSHIP AWARDS
Basic Science Research
Conrad Russell Y. Cruz, MD, PhD
Clinical Research
Bench to Bedside Research
Ioannis Koutroulis, MD, PhD, MBA
ELDA ARCE TEACHING SCHOLAR AWARD
SUZANNE FEETHAM NURSING RESEARCH SUPPORT AWARD
Eileen P. Engh, PhD RN
“Rare Disease Organization Lifecycle” Role in Helping Parents with Everyday Life Information Seeking and Connection (RDO-HELIX)
EXPLORATIONS IN GLOBAL HEALTH PILOT AWARDS
Launchpad Awards
Mi Ran Shin, MD, MPH
“Establishing Interdisciplinary Rehabilitation for Birth and Burn Injuries in Ethiopia”
Susan Harvey, MSN, CPNP-AC
“Implementation of Sickle Cell Pilot Program in Ndhiwa Sub County, Kenya”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
Brandy Salmon, PhD, associate vice president of Innovation and Partnerships at Virginia Tech, opened the day with “The Alchemy of Innovation,” focusing on how institutions can build a culture that fuels transformative partnerships.
A multidisciplinary panel discussion moderated by Nathan Kuppermann, MD, MPH, and Catherine Bollard, MBChB, MD, featured Nehal Mehta, MD, Julia Finkel, MD, Kevin Cleary, PhD, Ioannis Koutroulis, MD, PhD, MBA, Francesca Joseph, MD and Patrick Hanley, PhD, who shared how innovation can be advanced and promoted, especially as a core institutional priority.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.













The guidelines are the first globally acknowledged framework for developing and deploying health care AI applications and gauging whether the information they generate can be trusted or not.
More than 100 international experts in the application of artificial intelligence (AI) in health care published the first set of consensus guidelines that outline criteria for what it means for an AI tool to be considered trustworthy when implemented in health care settings.
The guidelines, published in the journal the BMJ, are the first globally acknowledged framework for developing and deploying health care AI applications and gauging whether the information they generate can be trusted or not.
Called the FUTURE-AI framework, the consensus guidelines are organized based on six guiding principles:
The cadre of experts reviewed and agreed upon a set of 30 best practices that fall within the six larger categories. These practices address technical, clinical, socio-ethical and legal aspects of trustworthy AI. The recommendations cover the entire lifecycle of health care AI: design, development and validation, regulation, deployment and monitoring.
The authors encourage researchers and developers to take these recommendations into account in the proof-of-concept phase for AI-driven applications to facilitate future translation to clinical practice.
“Patients, clinicians, health organizations and authorities need to know that information and analysis generated by AI can be trusted, or these tools will never make the leap from theoretical to real world application in a clinical setting,” says Marius George Linguraru, DPhil, MA, MSc, Connor Family Professor for Research and Innovation in the Sheikh Zayed Institute for Surgical Innovation at Children’s National Hospital and co-author of the guidelines. “Bringing so many international and multi-disciplinary perspectives together to outline the characteristics of a trustworthy medical AI application is part of what makes this work unique. It is my hope that finding such broad consensus will shed light on the greater good AI can bring to clinics and help us avoid problems before they ever impact patients.”
The FUTURE-AI consortium was founded by Karim Lekadir, PhD, ICREA Research Professor at the University of Barcelona in 2021 and now comprises 117 interdisciplinary experts from 50 countries representing all continents, including AI scientists, clinical researchers, biomedical ethicists and social scientists. Over a 2-year period, the consortium established these guiding principles and best practices for trustworthy and deployable AI through an iterative process comprising an in-depth literature review, a modified Delphi survey and online consensus meetings. Dr. Linguraru contributed with a unique perspective on AI for pediatric care and rare diseases.
The authors note that, “progressive development and adoption of medical AI tools will lead to new requirements, challenges and opportunities. For some of the recommendations, no clear standard on how these should be addressed yet exists.”
To tackle this uncertainty, they propose FUTURE-AI as a dynamic, living framework. This includes a dedicated website to allow the global community to participate in the FUTURE-AI network. Visitors can provide feedback based on their own experiences and perspectives. The input gathered will allow the consortium to refine the FUTURE-AI guidelines and learn from other voices.
Read the full manuscript outlining all 30 best practices: FUTURE-AI: international consensus guideline for trustworthy and deployable artificial intelligence in healthcare


Researchers at Children’s National Hospital are developing supervised autonomous robotic surgery to make expert kidney tumor removal accessible in rural areas, combining robotics, AI and surgeon oversight for safer, more precise outcomes.
Imagine a robot capable of planning and executing the intricate removal of a cancerous kidney tumor — a concept that might sound like science fiction. Yet this groundbreaking work is underway at the Sheikh Zayed Institute (SZI) for Pediatric Surgical Innovation at Children’s National Hospital.
Called Supervised Autonomous Robotic Renal Tumor Surgery (SARRTS), the project aims to prove that a supervised autonomous kidney resection is feasible. Its goal is to enable general surgeons in rural hospitals to oversee robots performing complex resections, democratizing access to specialized surgical care. Backed by a $1 million contract from the Advanced Research Projects Agency for Health (ARPA-H), the initiative represents new opportunities in medical innovation.
“The hope is that, someday, patients will no longer have to travel to major oncology centers to get the best possible surgical outcome when faced with renal tumors,” said Kevin Cleary, PhD, associate director of engineering at SZI. “We hope to combine the precision of robotics with a surgeon’s clinical expertise to create consistently high outcomes.”
Surgery is a cornerstone of cancer treatment, but access to skilled surgeons remains unevenly distributed nationwide. Autonomous robotic surgery could address this disparity by increasing access to expert-level care, enhancing the precision and consistency of procedures and unlocking new surgical possibilities beyond human surgeons’ capabilities.
Under the initial concept, the SARRTS system will use a combination of CT imaging and 3D mapping from a robot’s RGB-depth camera. While the robot independently plans and executes the incision and tumor resection, the supervising surgeon retains full control, with the ability to approve, modify or halt the procedure at any time — an interplay between human expertise and robotic precision to help ensure safety.
Testing will be conducted on realistic kidney models, called phantoms, which are designed to train and test surgical outcomes. The project aims to validate the feasibility of supervised autonomous tumor resection while advancing technologies that could pave the way for broader applications.
“Robotics and medicine have finally reached a point where we can consider projects requiring this level of complexity,” said Anthony Sandler, MD, senior vice president and surgeon-in-chief at Children’s National and executive director of SZI. By combining autonomous robotics, artificial intelligence and surgical expertise, we can profoundly impact the lives of patients facing life-altering cancer diagnoses.”
In addition to the kidney surgery initiative, the Children’s National team is pursuing other groundbreaking projects. These include a second ARPA-H contract focused on robotic gallbladder removal and a National Institutes of Health grant to explore robotic hip-pinning, a procedure used to repair fractured hips with pins, screws and plates.
Axel Krieger, PhD, an associate professor of mechanical engineering at Johns Hopkins University, is collaborating closely on the kidney resection and gallbladder projects. The interdisciplinary team believes this state-of-the-art care could be tested and developed within the next decade.
“This particular surgery is complex, and a robot may offer advantages to address difficulties created by patient anatomy and visibility within the surgical field,” said Dr. Sandler. “We can imagine a day – in the not too distant future – when a human and a robotic arm could team up to successfully advance this care.”
This project has been funded in whole with federal funds from ARPA-H under cooperative agreement AY1AX000023.


Dr. Asa Yancey’s pioneering operation went unrecognized for over half a century due to discriminatory publishing practices in academic medicine.
A group of international pediatric colorectal surgery leaders called for the renaming of a surgical procedure for Hirschsprung disease after finding evidence that an African American surgeon, Asa Yancey, M.D., had pioneered the procedure 12 years before its’ current namesake, Franco Soave, M.D. Dr. Yancey was not recognized previously due to discriminatory practices in academic medical publishing.
A literature review published in the Journal of Surgical Research conducted by the American Pediatric Surgical Association Hirschsprung disease interest group, including Marc Levitt, M.D., chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital, identified that Dr. Yancey’s work describing pull-through of normal colon through a cuff of aganglionic colon as a treatment for Hirschsprung disease was published in 1952. The paper by Soave was published in 1962 and from that work, the “Soave” procedure bore his name.
The authors point out that Dr. Yancey’s pioneering operation went unrecognized for over half a century because of the discriminatory segregation in the publishing practices of academic medicine dating back to the 1950s.
Dr. Levitt and his colleagues in the interest group suggested active changes to give posthumous credit to Dr. Yancey, including renaming the procedure to the Yancey-Soave pull-through technique.
Together with Dr. Yancey’s family, including his children, three of whom are physicians, the interest group and other surgeons have started using the procedure’s new name in presentations, operative notes, articles and book chapters.
At the end of their literature review recommending the update, the authors wrote, “Posthumous acknowledgment of Yancey was long overdue but signifies improvements in the inclusion of underrepresented groups in academic medicine while simultaneously reminding physicians that there is still much work to be done.”
Read the article The Story of Dr. Asa G. Yancey and Surgical Innovation in the Face of Discrimination in the Journal of Surgical Research.
![]() In 2024, Children’s National Hospital continued to make remarkable strides across diverse areas of pediatric medicine, from groundbreaking technological innovations to critical health advocacy. The following compilation showcases ten significant stories that demonstrate the breadth and depth of the hospital’s impact, as featured in major national news outlets including NBC Nightly News, CNN, The Washington Post, The New York Times, NPR, The Today Show, Healio, and POLITICO. Delve into our 2024 news highlights for more.
In 2024, Children’s National Hospital continued to make remarkable strides across diverse areas of pediatric medicine, from groundbreaking technological innovations to critical health advocacy. The following compilation showcases ten significant stories that demonstrate the breadth and depth of the hospital’s impact, as featured in major national news outlets including NBC Nightly News, CNN, The Washington Post, The New York Times, NPR, The Today Show, Healio, and POLITICO. Delve into our 2024 news highlights for more.
Charles Berul, M.D., and a patient family talk about the pill-sized pacemaker that saved the life of Abby, an infant born with deadly heart defects. (NBC Nightly News)
Sivabalaji Kaliamurthy, M.D., addiction psychiatrist and director of the Addictions Program, spoke to CNN about the impact of drug addiction on teen health and the lack of resources available to treat opioid use disorder. (CNN)
Susma Vaidya, M.D., M.P.H., associate medical director of the IDEAL Clinic, shared her concerns about childhood obesity treatment recommendations issued today by a leading panel of independent U.S. health experts. (The Washington Post)
Shideh Majidi, M.D., M.S.C.S., and Emily Frymark, clinical dietitian, spoke about how the food pharmacy, created in partnership with the Capital Area Food Bank, benefits patients with diabetes and other chronic conditions. (The Washington Post)
Kendric Cromer, a 12-year-old boy being treated at Children’s National Hospital, became the first person in the world with sickle cell disease to begin a commercially approved gene therapy that may cure the condition. “This is a big effort,” says David Jacobsohn, M.D., ScM, M.B.A. (The New York Times)
Mikael Petrosyan, M.D., associate chief of General and Thoracic Surgery, discusses the stress medical staff face when treating young victims of gun violence. (NPR)
Landon, an 11-year-old patient, rang the bell at Children’s National Hospital with family, friends, doctors and nurses cheering after finishing his final round of chemotherapy. (The Today Show)
Monika Goyal, M.D., M.S.C.E., pediatric emergency medicine specialist and co-director of the Center for Translational Research, emphasized the need for awareness in addressing period poverty in teenagers and young adults. (Healio)
Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer, participates in a panel discussion covering AI data collection, associated risks, reliance and other topics related to artificial intelligence. (POLITICO)
Children’s National patient Kendric Cromer, 12, became one of the first children ever to be treated with a newly approved gene therapy that will free him from the sickle cell disease that has stolen his childhood. (The New York Times)

 2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.
2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.
A study led by researchers at Children’s National Hospital showed that babies born during the COVID-19 pandemic have differences in the size of certain structures in the brain, compared to infants born before the pandemic. The findings suggest that exposure to the coronavirus and being pregnant during the pandemic could play a role in shaping infant brain development.
(3 min. read)
Children’s National Hospital was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
(2 min. read)
In January 2023, a team of multidisciplinary doctors performed the first case in the world of using bilateral high intensity focused ultrasound (HIFU) pallidotomy on Jesus, a 22-year-old patient with dyskinetic cerebral palsy. The procedure is part of a clinical trial led by Chima Oluigbo, M.D., pediatric neurosurgeon at Children’s National Hospital.
(3 min. read)
A novel ultrasound device developed by Bloom Standard received the Food and Drug Administration’s valued breakthrough device designation with the help of Children’s National Hospital. The device that enables autonomous, hands-free ultrasound scans to be performed anywhere, by any user.
(2 min. read)
Understanding the effects of Lyme disease on the developing fetal brain is essential to ensure timely prenatal and postnatal treatments to protect the fetus and newborn. In response to this need, Children’s National Hospital is leading a pilot study to establish the groundwork needed for a larger study to determine the effect of in utero exposure to Lyme disease on pregnancy and early childhood neurodevelopmental outcomes.
(3 min. read)
Five years ago, Cayden was born 6 weeks early weighing less than four pounds and at risk of dying from her critical congenital heart disease. Today, she’s a happy five-year-old. Early diagnosis of her hypoplastic right ventricle, double inlet left ventricle and critical coarctation of the aorta allowed for the team at Children’s National Hospital to create a careful plan for safe delivery and to offer an innovative hybrid HLHS surgical approach at the hospital within 24 hours after she was born.
(1 min. read)
Children’s National Hospital appointed Wayne J. Franklin, M.D., F.A.C.C., as the new senior vice president (SVP) of the Children’s National Heart Center. In this role, Dr. Franklin oversees the full spectrum of heart care services including cardiac imaging and diagnostics, interventional cardiology, electrophysiology, cardiac anesthesia, cardiac surgery and cardiac intensive care.
(2 min. read)
By pioneering artificial intelligence (AI) innovation programs at Children’s National Hospital, Marius George Linguraru, D.Phil., M.A., M.Sc., and the AI experts he leads are ensuring patients and families benefit from a coming wave of technological advances. The team is teaching AI to interpret complex data that could otherwise overwhelm clinicians.
(4 min. read)
Painting a sobering picture, a research team led by Children’s National Hospital culled years of data demonstrating that maternal mental illness is an under-recognized contributor to the death of new mothers. They called for urgent action to address this public health crisis.
(3 min. read)
Children’s National Hospital appointed Nathan Kuppermann, M.D., M.P.H., as its new executive vice president, chief academic officer and chair of Pediatrics. In this role, Dr. Kuppermann oversees research, education and innovation for the Children’s National Research Institute as well as academic and administrative leadership in the Department of Pediatrics at George Washington University School of Medicine & Health Services.
(2 min. read)
Researchers from Children’s National Hospital presented findings from the first clinical trial of the medication vosoritide for children with hypochondroplasia – a rare genetic growth disorder. During the phase 2 trial, researchers found vosoritide increased the growth rate in children with hypochondroplasia, allowing them to grow on average an extra 1.8 cm per year.
(2 min. read)
Since its establishment in July 2023, the Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital has gained recognition through high-impact scientific publications, featuring noteworthy studies exploring the early phases of human development.
(3 min. read)
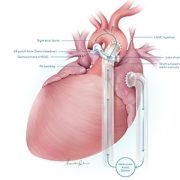
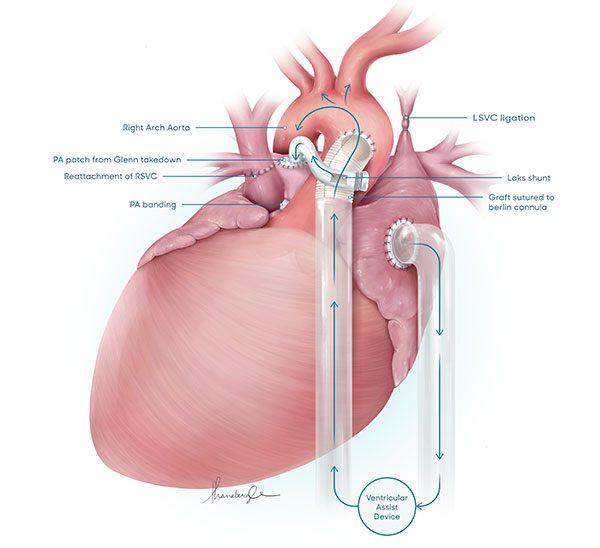
The team supported R’s heart using a VAD and an innovative implantation technique to increase the likelihood he would tolerate the device well.
A case study published in the Journal of Thoracic and Cardiovascular Surgery Techniques demonstrates a proof of concept that temporary use of a VAD to support a single ventricle heart may give that heart time to grow stronger and allow for corrective and lifesaving procedures under cardiopulmonary bypass instead of heart transplant.
The cardiac surgery team at Children’s National Hospital was able to offer a young boy’s family a lifesaving surgical option, after they were told elsewhere that their only choice was palliative care.
Baby R was born with a series of complex congenital heart conditions: Heterotaxy syndrome, unbalanced atrioventricular septal defect (AVSD), severe atrioventricular valve regurgitation, reduced ventricular function and obstructed total anomalous pulmonary venous drainage (TAPVD).
That combination of defects left his family facing an unthinkable statistic — there was an up to 90% possibility that R would die before reaching his first birthday.
A set of early interventions, including an initial attempt at a single ventricular correction called a bi-directional cavo-pulmonary shunt (BCPS) failed. His already weak heart was left even weaker than before. He continued to decline.
“We don’t ever want to say, ‘There is nothing we can do for your child,’” says Yves d’Udekem, M.D., Ph.D., chief of cardiac surgery at Children’s National. “Instead, we make the impossible, possible.”
The team decided to support R’s heart using a ventricular assist device (VAD) and an innovative technique during implantation of the VAD to increase the likelihood that he would tolerate the device well. By relieving some of the heart’s workload, they hoped that complicating functional issues might improve enough to allow surgeons to operate again and fix some of the structural conditions to optimize blood flow.
There is literature showing VAD used in this way in adults with heart failure, but until now it had never been successfully applied as a bridge to surgical intervention in a child with a single functioning ventricle. These assist devices are typically used only as a bridge to heart transplant in children.
This is the first documented case where ventricular assist device implantation resulted in gradual improvement in ventricular function, atrioventricular valve regurgitation, and pulmonary vascular resistance.
The improvements culminated in a major milestone: After 8 weeks of VAD support, at 6 months old, R was weaned off the device and had a successful BCPS, the first of several surgical procedures to make blood flow in his heart effective enough to sustain his organs.
When he was 14 months old, he returned for a successful second procedure along the established single ventricle pathway.
R is nearly 3 years old and thriving at home, not in the CICU, as he waits to undergo the Fontan procedure — the final structural surgery for his single ventricle heart.
The knowledge and skill of Children’s National Heart Center turned this formerly hopeless situation into a brighter prognosis by repurposing existing technology to save a life.
In their case study conclusion, the team writes, “The observed improvement in ventricular function and AV valve regurgitation following VAD implantation in this patient is proof of the concept that patients with a failing single-ventricle circulation can be bridged to recovery by temporary VAD support. This concept may open new avenues of treatment.”
Read the study: Revalidation to single ventricle pathway with single ventricular assist device: Proof of concept

 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
This year, U.S. News ended ordinal rankings on its Honor Roll. Instead of assigning a numerical rank from 1 to 10, all hospitals on the Honor Roll will be recognized as having attained the highest standards of care in the nation.
In addition, Children’s National tied for #1 pediatric hospital in the Mid-Atlantic region, which includes New York, New Jersey, Delaware, Pennsylvania, the District of Columbia, West Virginia and Virginia. It’s also best in the Mid-Atlantic in Neonatology.
For the fourteenth straight year, Children’s National ranked in 10 specialty services. New this year, U.S. News included behavioral health as a service line in the rankings. Since it’s the first year, there are no ordinal rankings for behavioral health, but the Children’s National program was named one of the top 50 programs in the country.
“In my first year here, I witnessed what makes Children’s National so special — our commitment to collaboration, empowering one another, and charting a bold path forward for pediatric care,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “I’m proud U.S. News again recognized Children’s National as one of the top in the nation and the highest-ranked pediatric hospital in D.C., Maryland and Virginia. Together, we’ll continue to push the boundaries of care, research and innovation to make a difference for those who matter most — the kids.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“For nearly two decades, U.S. News has published Best Children’s Hospitals to empower the parents and caregivers of children with complex medical needs,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Children’s hospitals appearing on the U.S. News Honor Roll have a track record of delivering unparalleled specialized care.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
The other four specialties ranked among the top 50 are Behavioral Health, Cardiology and Heart Surgery, Pulmonology and Lung Surgery, and Urology.


“It is a market failure that we are dealing with – a lack of incentives leading to a stagnation in innovation with respect to small markets, such as pediatrics. Children’s National Hospital and our partners in other children’s hospitals in the country play a critical role in making noise and sending a message that children should not be an afterthought.”
Hear more from Kolaleh Eskandanian, Ph.D., M.B.A., during her recent appearance at POLITICO. As vice president and chief innovation officer at Children’s National and Alliance for Pediatric Device Innovation principal investigator, Dr. Eskandanian shared her approach to engaging with the Food and Drug Administration (FDA) to advance artificial intelligence (AI) and machine learning technologies for pediatric healthcare. To date, she noted, the FDA has authorized 950 healthcare-related technologies enabled with AI and machine learning.

Patients want to hear they are “in good hands” when choosing a surgeon. A Children’s National Hospital team is investigating whether those hands could be replaced with an autonomous robotic arm during pediatric cholecystectomy procedures.
“The role of autonomous surgery is at a pivot point,” said Anthony Sandler, M.D., senior vice president and surgeon-in-chief at Children’s National and director of the Sheikh Zayed Institute of Pediatric Surgical Innovation (SZI). “Just as it is with autonomously driving cars, we are testing whether a gallbladder removal can be controlled and managed by a robotic arm, rather than a laparoscopic surgeon. In preclinical models, we are evaluating whether we can take the next step forward. We believe we can, and this research will be proof of concept for autonomous surgery.”
The rate of cholecystectomy has been on the rise among pediatric patients for the last two decades. It becomes necessary when the gallbladder becomes full of painful gallstones, often caused by obesity and inherited blood disorders like sickle cell disease. Across the country, 99% of gallbladder removals happen without complications.
Yet Children’s National hopes to develop technologies to boost that number even higher. Working with partners, the hospital has embarked on two contracts with the Advanced Research Projects Agency for Health (ARPA-H): a three-year and a two-year contract, worth $3.5 million each (75N91023C00048 & 75N91023C00053, respectively). The Children’s National team is collaborating on solutions with Optosurgical Chief Executive Officer Yoseph Kim, M.S.E., and Axel Krieger, Ph.D., associate professor of mechanical engineering at Johns Hopkins University.
They are tapping into two areas of expertise: robotic surgery and the development of a novel fluorescent dye that – when paired with advanced imaging – can aid surgeons in seeing bleeds during gallbladder removals.
The project also combines the talents of Dr. Sandler and Children’s National optical engineer Richard Cha, Ph.D., principal investigator at SZI, to explore how to integrate these technologies in the operating room.
“Autonomous gallbladder removal involves the identification of the target tissue – the bile duct, the cystic artery and the gallbladder. Our team’s new 3D imaging techniques will help visualize and work through the surgical steps, by locating each target,” Dr. Cha said. “When this technology and related programming come together, it could mark a significant step forward in pediatric surgery.”
Given the gallbladder’s small size and accessible location just beneath the liver, cholecystectomy is most often done laparoscopically, using small cameras and incisions. There are three main steps: ligating – or closing off – the cystic artery, ligating the cystic duct while protecting the common bile duct, and removing the gallbladder. Drs. Sandler and Cha believe outcomes will improve if the expertise and delicacy of a robot are incorporated into the procedure.
“If you’re that one patient out of 100 who has significant bleeding post-operatively or, even worse, you are among the 0.5% of patients who have an injury to the bile duct, the impact on your wellbeing is significant after that surgery,” Dr. Sandler said. “Having that extra security of technology and guidance will be an incredible value-add for any patient undergoing this procedure.”
These projects have been funded in whole with federal funds from ARPA-H, National Institutes of Health, Department of Health and Human Services, under Contract No. 75N91023C00053 and Contract No. 75N91023C00048.
Drs. Oetgen and Kane join a distinguished group of Children’s National physicians and scientists who hold an endowed chair.
Children’s National Hospital named Matthew Evan Oetgen, M.D., as the Joseph E. Robert, Jr. Professor of Orthopaedic Surgery and Sports Medicine. Dr. Oetgen serves as chief of Orthopaedic Surgery and Sports Medicine.
Children’s National Hospital named Timothy Dennis Kane, M.D., as the Joseph E. Robert, Jr. Professor of General and Thoracic Surgery. Dr. Kane serves as chief of General and Thoracic Surgery.
Drs. Oetgen and Kane join a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful for its generous donors, who have funded 48 professorships to-date.
Professorships support groundbreaking work on behalf of children and their families. They foster new discoveries in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and donor’s forethought to advance and sustain knowledge.
Dr. Oetgen is a longstanding leader in orthopaedic surgery and sports medicine. Under his leadership, Children’s National opened the Fight For Children Sports Medicine Center in 2021. It provides a wide range of orthopaedic services to help young athletes function at their peak performance. Additionally, his team launched the nation’s first pediatric Spinal Fusion Surgical Home. This program led to significant decreases in average length of stay and patient pain scores for children with idiopathic scoliosis.
“We provide state-of-the-art care to young athletes across the region,” says Dr. Oetgen. “This professorship will help us continue the development of innovative clinical and research programs that streamline care for children with complex orthopaedic needs.”
Dr. Oetgen has authored more than 60 book chapters and publications. He has presented at many major national and international conferences in his field. Dr. Oetgen is also a key member of the multidisciplinary clinical trial team that was the first to apply magnetic resonance guided high-intensity focused ultrasound to non-invasively relieve osteoid osteoma tumors in children.
Dr. Kane works to develop the Joseph E. Robert, Jr. Center for Surgical Care’s minimally invasive surgery program through clinical practice, instruction and research, while improving minimally invasive surgical techniques and speed into standard clinical care for pediatrics. He serves as principal investigator in the Minimally Invasive Therapy Program in the Bioengineering Initiative of the Sheikh Zayed Institute for Pediatric Surgical Innovation. He has specific interest and expertise in minimally invasive thoracic, gastrointestinal and neonatal surgery. Under his direction, the Division of General & Thoracic Surgery developed peroral endoscopic myotomy (POEM), a newer technique to treat esophageal achalasia in children.
“Children’s National performs more POEM procedures than any other children’s hospital in the country,” says Dr. Kane. “I’m grateful for this professorship and look forward to making even more surgical advances in pediatric care.”
The Joseph E. Robert Jr. Trust, through their vision and generosity, are ensuring that Drs. Oetgen, Kane and future holders of these professorships will launch bold, new initiatives. These innovations will help rapidly elevate our leadership in the field of pediatric orthopaedic and general surgery and improve lifetimes for children.
The Joseph E. Robert, Jr. Charitable Trust is a long-time champion of Children’s National. It honors the memory of the late Joseph “Joe” E. Robert, Jr. A native of Washington D.C., Joe was an entrepreneur and visionary who believed in the importance of investing in children through education and healthcare. His first gift to Children’s National created and endowed our Joseph E. Robert, Jr. Center for Surgical Care. He was also instrumental in shaping the vision and building support for the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National, created in 2009 with a $150 million gift from the Government of Abu Dhabi.
These professorships embody Joe’s legacy of inspiring others to think bigger and differently to advance pediatric healthcare for children of the Washington, D.C. community and beyond.
“Joe’s legacy is represented through the incredible work being done at Children’s National,” says David Fensterheim, board chair of Fight For Children. “Drs. Oetgen and Kane are trailblazers in pediatric healthcare. We are proud to honor them and their cutting-edge work with this prestigious professorship.”


Dr. Cleary joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair.
Children’s National Hospital named Kevin Cleary, Ph.D., as the Sheikh Zayed Professor of Bioengineering through philanthropic support from the people of the United Arab Emirates (UAE).
Dr. Cleary serves as Technical Director of the Bioengineering Initiative within the hospital’s Sheikh Zayed Institute for Pediatric Surgical Innovation. He also is professor of Pediatrics and Radiology at The George Washington University School of Medicine and Health Sciences.
Dr. Cleary joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful to generous donors who altogether have funded 48 professorships.
Professorships support groundbreaking work on behalf of children and their families. They foster new discoveries and innovations in pediatric medicine. These appointments reflect the recipient’s achievements and the donor’s commitment to advancing knowledge.
Under Dr. Cleary’s leadership, the Bioengineering Initiative fosters innovation via collaboration across the hospital. It fuels the development of minimally-invasive robotics that improve outcomes for children. For example, Dr. Cleary’s team is collaborating with the Division of Physical Medicine & Rehabilitation to develop PedBotHome. This video game-based robotic ankle device helps children with neurological impairments such as cerebral palsy do rehabilitation exercises at home.
“I am deeply honored by this endowed professorship,” says Dr. Cleary. “It will enable me to continue to fulfill our mission of providing more precise and less invasive solutions to improve children’s health. The Sheikh Zayed Institute will continue to be a hub for technology development and innovation.”
The people of the UAE created the professorship endowment through philanthropy. The UAE’s vision and generosity will ensure that Dr. Cleary and future holders of this professorship will have the opportunity to make strategic and timely investments. This will advance the field of bioengineering and improve children’s lives.
Children’s National takes pride in four decades of medical collaboration with the UAE. This relationship inspired a philanthropic partnership yielding more than $215 million to advance children’s health worldwide. The UAE’s generosity reflects the longstanding commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, president of the UAE and ruler of Abu Dhabi.
In 2009, the UAE generously funded the creation of the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National. The government of Abu Dhabi made the gift in honor of His Highness Sheikh Zayed bin Sultan Al Nayhan. Sheikh Zayed founded the UAE and served as the country’s president from 1971 until his death in 2004.
The Institute seeks to make pediatric surgery more precise, less invasive and pain free. It drives progress for children by translating breakthrough discoveries into new treatments and medical inventions. These include support for a technology that seeks to objectively measure pain through a handheld device and the first use of high-intensity focused ultrasound (HIFU) to treat childhood nerve tissue tumors.
The Sheikh Zayed Professorship in Bioengineering is a continuation of the UAE’s investment within the Sheikh Zayed Institute.
The amount of long-term liver cirrhosis in children with single ventricle congenital heart disease who underwent the Fontan procedure may depend on which surgical approach is chosen by the pediatric cardiac surgeon.
The amount of long-term liver cirrhosis in children with single ventricle congenital heart disease who underwent the Fontan procedure may depend on which surgical approach is chosen by the pediatric cardiac surgeon, according to researchers at Children’s National Hospital who presented their findings this week at the American Association of Thoracic Surgery annual meeting. The full manuscript appears in the Journal of Thoracic and Cardiovascular Surgery.
Senior study author Yves d’Udekem, M.D., Ph.D., chief of Cardiac Surgery at Children’s National, says that the vast majority of Fontan procedures in the United States use an extracardiac conduit approach to redirect blood flow to the lungs. However, a retrospective review of 332 patients who underwent the Fontan at Children’s National showed that children who received the extracardiac Fontan may experience liver cirrhosis at a rate of 30% after 15 years compared to the lateral tunnel approach which showed 15-year liver cirrhosis at a significantly lower rate of 4.4%. The lateral tunnel was a well-established method pioneered in Europe by pediatric cardiac surgeon Marc de Leval in the 1980s. This technique lost traction in the field and people started in the 1990s to perform a variation of the technique called the extracardiac Fontan because it was thought that it would be giving more favorable flows and protect the patients against rhythm issues. Thirty years later, these predictions did not reveal themselves to be true.
“Since the 1990s, the vast majority of Fontan procedures in the United States are performed creating an extracardiac conduit rather than the lateral tunnel,” says Dr. d’Udekem. “But what we see when we follow long-term outcomes of these children is a consequence not reported before.”
Dr. d’Udekem and the research team, including presenter and first author Eiri Kisamori, M.D., a cardiac surgery fellow at Children’s National, are the first to report these findings based on reviews of 15-year outcome data. These retrospective reviews of long-term outcomes are a critical tool to inform and improve clinical approaches with the goal of optimizing the long-term quality of life for children born with these critical congenital conditions.
While more research is needed, the authors hypothesize that the size of the conduit for blood flow may be the culprit for higher levels of liver damage. For children who have already received an extracardiac Fontan, Dr. d’Udekem says that widening their existing conduit in a reoperation may successfully improve blood flow to the liver. For future procedures, he notes that in his own practice, he now uses the lateral tunnel approach whenever possible.
Read the study: Alarming rate of liver cirrhosis after the small conduit Extracardiac Fontan. A comparative analysis with the Lateral Tunnel.

Children’s National experts pioneered a novel approach of inducing strokes to stop seizures and improve neurodevelopmental outcomes in newborns under three months old with hemimegalencephaly (HME). The procedure, called an endovascular embolic hemispherectomy, can be safely used to provide definitive treatment of HME-related epilepsy in neonates and young infants. Monica Pearl, M.D., neurointerventional radiologist, and Panagiotis Kratimenos, M.D., Ph.D., neonatologist, discuss why having a multidisciplinary team skilled at this procedure is the reason we’re the only center in the world capable of providing this treatment.
