Cardiac care leaders recognized for mentorship and innovation at AAP
Two Children’s National Hospital cardiac care leaders received prestigious recognition awards from the American Academy of Pediatrics (AAP) during that organization’s virtual National Conference and Exhibition in October 2021.
- Gil Wernovsky, M.D., cardiac critical care specialist at Children’s National Hospital, received the 2021 Maria Serratto Master Educator Award from AAP Section on Pediatric Cardiology and Cardiac Surgery, celebrating his 30-plus-years as a clinician, educator, mentor and leader in the field.
- Gerard Martin, M.D., FAAP, FACC, FAHA, C. Richard Beyda Professor of Cardiology, Children’s National Hospital, received the AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award, in recognition of his work to establish the use of pulse oximetry to screen newborn infants for critical congenital heart disease in the first 24 hours of life.
Dr. Wernovsky: 2021 Maria Serratto Master Educator Award, AAP Section on Pediatric Cardiology and Cardiac Surgery

Gil Wernovsky, M.D., received the 2021 Maria Serratto Master Educator Award from AAP Section on Pediatric Cardiology and Cardiac Surgery.
The Master Educator Award is presented each year to a pediatric cardiologist or cardiothoracic surgeon who exemplifies excellence as an educator, mentor and/or leader in the field.
A practicing cardiac critical care specialist with more than 30 years’ experience in pediatric cardiology, Dr. Wernovsky trained and mentored more than 300 fellows in pediatric cardiology, cardiac surgery, neonatology, critical care medicine and cardiac anesthesia, in addition to countless residents and fellows. He also organizes national and international symposia to share expertise around the world. During the COVID-19 public health emergency, for example, he co-founded the Congenital Heart Academy (CHA). The CHA provides content from an international faculty of cardiac care to more than 26,000 practitioners in 112 countries and includes a thriving YouTube channel.
Dr. Wernovsky is also a founding member of several international societies focused on bringing together clinicians, researchers and students across sub-specialties of pediatric cardiology and cardiac surgery for knowledge exchange and best practice sharing. These include: the Pediatric Cardiac Intensive Care Society, World Society for Pediatric and Congenital Heart Surgery, the International Society of Pediatric Mechanical Circulatory Support and the Cardiac Neurodevelopmental Outcome Collaborative.
Dr. Wernovsky received the award on October 10 at the virtual Scientific Sessions of the 2021 American Academy of Pediatrics National Conference and Exhibition.
Dr. Martin: AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award
Gerard Martin, M.D., FAAP, FACC, FAHA, C. Richard Beyda Professor of Cardiology, Children’s National Hospital, received the AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award.
The Section on Advances in Therapeutics and Technology (SOATT) educates physicians, stimulates research and development and consults on therapeutics and technology-related matters for the AAP. The Achievement Award recognizes someone who has shown leadership in applying innovative approaches to solve pressing problems.
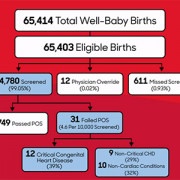
Dr. Martin is the C. Richard Beyda Professor of Cardiology and has cared for children at Children’s National for more than 30 years. As an advocate for congenital heart disease efforts nationally and internationally, he played an integral role in the development of an innovative use of existing hospital technology—the pulse oximeter—to detect critical congenital heart disease in newborn babies.
Today, Dr. Martin and colleagues across the United States and around the world have worked to make this screening method a standard of care for newborns everywhere. It is a part of the Health Resources and Services Administration (HRSA) Recommended Uniform Screening Panel and has become law in every state. They continue to conduct research to refine the recommendations and hone-in on the most effective ways to harness these tools.
Dr. Martin was selected for this award in 2020. He accepted it and offered remarks during the 2021 virtual AAP National Conference and Exhibition on Monday, October 11, 2021.