



Children’s National Hospital in Washington, D.C., was ranked No. 7 nationally in the U.S. News & World Report 2020-21 Best Children’s Hospitals annual rankings. This marks the fourth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide.
In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fourth year in a row.
For the tenth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“Our number one goal is to provide the best care possible to children. Being recognized by U.S. News as one of the best hospitals reflects the strength that comes from putting children and their families first, and we are truly honored,” says Kurt Newman, M.D., president and CEO of Children’s National Hospital.
“This year, the news is especially meaningful, because our teams — like those at hospitals across the country — faced enormous challenges and worked heroically through a global pandemic to deliver excellent care.”
“Even in the midst of a pandemic, children have healthcare needs ranging from routine vaccinations to life-saving surgery and chemotherapy,” said Ben Harder, managing editor and chief of Health Analysis at U.S. News. “The Best Children’s Hospitals rankings are designed to help parents find quality medical care for a sick child and inform families’ conversations with pediatricians.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
The other three specialties ranked among the top 50 were cardiology and heart surgery, gastroenterology and gastro-intestinal surgery, and urology.


Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
You can view the entire Children’s National Research Institute academic annual report online.


Despite early reports suggesting COVID-19 does not seriously impact children, a new study shows that children who contract COVID-19 can become very ill.
In contrast to the prevailing view that the novel coronavirus known as COVID-19 does not seriously impact children, a new study finds that children who contract the virus can become very ill—many of them critically so, according to physician researchers at Children’s National Hospital. Their results, published in the Journal of Pediatrics and among the first reports from a U.S. institution caring for children and young adults, shows differences in the characteristics of children who recovered at home, were hospitalized, or who required life support measures. These findings highlight the spectrum of illness in children, and could help doctors and parents better predict which pediatric patients are more likely to become severely ill as a consequence of the virus.
In late 2019, researchers identified a new coronavirus, known as SARS-CoV-2, which causes COVID-19. As the disease spread around the world, the vast majority of reports suggested that elderly patients bear the vast majority of the disease burden and that children are at less risk for either infection or severe disease. However, study leader Roberta DeBiasi, M.D., M.S., chief of the Division of Infectious Diseases at Children’s National, states that she and her colleagues began noticing an influx of children coming to the hospital for evaluation of a range of symptoms starting in mid-March 2020, who were tested and determined to be infected with COVID-19. One quarter of these children required hospitalization or life support.
“It was very apparent to us within the first several weeks of the epidemic that this was a very different situation than our colleagues on the West Coast of the US had described as their experience just weeks before,” DeBiasi says. “Right away, we knew that it was important for us to not only care for these sick children, but to examine the factors causing severe disease, and warn others who provide medical care to children.”
To better understand this phenomenon, she and her colleagues examined the medical records of symptomatic children and young adults who sought treatment at Children’s National for COVID-19 between March 15 and April 30, 2020. Each of these 177 children tested positive using a rapid assay to detect SARS-CoV-2 performed at the hospital. The researchers gathered data on each patient, including demographic details such as age and sex; their symptoms; whether they had any underlying medical conditions; and whether these patients were non-hospitalized, hospitalized, or required critical care.
The results of their analysis show that there was about an even split of male and female patients who tested positive for COVID-19 at Children’s National during this time period. About 25% of these patients required hospitalization. Of those hospitalized, about 75% weren’t considered critically ill and about 25% required life support measures. These included supplemental oxygen delivered by intubation and mechanical ventilation, BiPAP, or high-flow nasal cannula – all treatments that support breathing – as well as other support measures such as dialysis, blood pressure support and medications to treat infection as well as inflammation.
Although patients who were hospitalized spanned the entire age range, more than half of them were either under a year old or more than 15 years old. The children and young adults over 15 years of age, Dr. DeBiasi explains, were more likely to require critical care.
About 39% of all COVID-19 patients had underlying medical conditions, including asthma, which has been highlighted as a risk factor for worse outcomes with this infection. However, DeBiasi says, although underlying conditions were more common as a whole in hospitalized patients – present in about two thirds of hospitalized and 80% of critically ill – asthma didn’t increase the risk of hospitalization or critical illness. On the other hand, children with underlying neurological conditions, such as cerebral palsy, microcephaly, or global developmental delay, as well as those with underlying cardiac, hematologic, or oncologic conditions were significantly more likely to require hospitalization.
In addition, although early reports of COVID-19 suggested that fever and respiratory symptoms are hallmarks of this infection, Dr. DeBiasi and her colleagues found that fewer than half of patients had both concurrently. Those with mild, upper respiratory symptoms, such as runny nose, congestion, and cough were less likely to end up hospitalized than those with more severe respiratory symptoms, such as shortness of breath. The frequency of other symptoms including diarrhea, chest pain and loss of sense of smell or taste was similar among hospitalized and non-hospitalized patients.
Dr. DeBiasi notes that although other East Coast hospitals are anecdotally reporting similar upticks in pediatric COVID-19 patients who become seriously ill, it’s currently unclear what factors might account for differences from the less frequent and milder pediatric illness on the West Coast. Some factors might include a higher East Coast population density, differences between the genetic, racial and ethnic makeup of the two populations, or differences between the viral strains circulating in both regions (an Asian strain on the West Coast, and a European strain on the East Coast).
Regardless, she says, the good news is that the more researchers learn about this viral illness, the better prepared parents, medical personnel and hospitals will be to deal with this ongoing threat.
Other researchers from Children’s National who participated in this study include Xiaoyan Song, Ph.D., M.Sc., Meghan Delaney, D.O., M.P.H., Michael Bell, M.D. , Karen Smith, M.D., Jay Pershad, M.D., Emily Ansusinha, Andrea Hahn, M.D., M.S., Rana Hamdy, M.D., M.P.H., MSCE, Nada Harik, M.D., Benjamin Hanisch, M.D., Barbara Jantausch, M.D., Adeline Koay, MBBS, MS.c., Robin Steinhorn, Kurt Newman, M.D. and David Wessel, M.D.
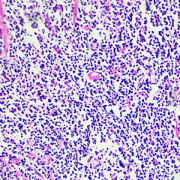
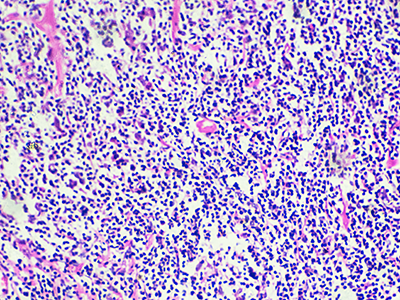
Each year, about 9,000 new patients are diagnosed with Hodgkin lymphoma, 10-15% of them children.
Each year, about 9,000 new patients are diagnosed with Hodgkin lymphoma, 10-15% of them children. Despite a relatively high cure rate for children with Hodgkin lymphoma, there are many debilitating long-term side effects of the treatments currently used. Additionally, 15-20% of children have a relapse and only half of them experience a long-term cure. Diffuse large B cell Lymphomas are another type of aggressive lymphoma that are difficult to cure, especially when they do not respond to upfront chemotherapy (refractory). Patients who experience relapse have to undergo more intensive chemotherapy followed by autologous stem cell transplantation and yet often times their lymphoma comes back.
Physicians at Children’s National Hospital, in partnership with the Huntsman Cancer Institute at the University of Utah School of Medicine, are enrolling patients in a clinical trial to test the safety of administering PD-1 inhibitor Nivolumab given prior to and following the infusions of the patients’ own TAA-T cells which have been trained to target tumor cells in the laboratory. Nivolumab is currently approved by the FDA for relapsed Hodgkin lymphoma. Nivolumab acts by unleashing the brakes put on by the lymphoma cells, and by doing so, Nivolumab allows the immune system to overcome the tumor’s escape mechanism.
“We believe that if our T cells are deemed safe when given in combination with already approved drugs, we may be able to impact multiple lives and reduce long-term toxicities from conventional chemotherapies,” said Hema Dave, M.D., an oncologist at Children’s National. “We’re hopeful that combination immunotherapies will produce more durable responses than when immunotherapies are given alone as a single agent and, additionally, that they will reduce the use of cytotoxic chemotherapy.”
The investigators will collect blood from the patients to isolate peripheral blood mononuclear cells. They will then make special cells called dendritic cells to stimulate the T cells. Then they will add special mixtures of tumor proteins WT1, PRAME and Survivin and provide a cytokine milieu favorable to T cell expansion/activation, inducing selective expansion of T cells targeted to kill tumor cells. This process trains the T cells to recognize the tumor proteins and become specialized TAA-T cells. The cells will be grown and frozen until ready for use. While the T cells are growing, the patients will be given Nivolumab.
“We’re really trying to test if priming the patients with Nivolumab will make their T cells more effective when they get infused,” says Dr. Dave. “The Nivolumab will help prepare the immune system. Then, when we infuse the T cells, our hope is that the environment is primed for the T cells to expand, grow and work to attack the cancer. If we can prime the immune system and make it more conducive for the T cells, then maybe they will have a better chance to get to the lymphoma cells and thus have a more sustained response.”
Patients will then receive two infusions of the TAA-T cells and be monitored for side effects. The anticipated enrollment is 18 patients over the next 2-3 years. If there is a positive response in patients enrolled in this safety trial, it could expand to test for efficacy of the novel combination immunotherapy.
For more information about this trial, contact:
Hema Dave, M.D.
202-476-6397
hkdave@childrensnational.org
Fahmida Hoq, MBBS, MS
202-476-3634
fhoq@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly every aspect of pediatric cancer care, our work is making great advancements in childhood cancer.

“The study was impactful because it established the activity of vincristine/irinotecan against Wilms tumor. Based on these findings, this chemotherapy combination will be applied more broadly in the treatment of Wilms tumor,” says study leader Jeffrey S. Dome, M.D, Ph.D.
Wilms tumor, the most common kidney cancer of childhood, may be classified into different subtypes based on its appearance under the microscope. The “favorable histology” subtype is associated with an excellent survival rate of approximately 90%, whereas the “diffuse anaplastic” subtype is associated with survival rates of only 55% for patients with stage II-IV disease.
The Children’s Oncology Group AREN0321 study, led by Jeffrey S. Dome, M.D, Ph.D., vice president of the Center for Cancer and Blood Disorders at Children’s National Hospital, tested the anti-tumor activity of the chemotherapy combination vincristine and irinotecan in patients with metastatic diffuse anaplastic Wilms tumor.
The study also evaluated whether a new treatment regimen containing carboplatin in addition to the currently used agents (vincristine, doxorubicin, cyclophosphamide and etoposide) would improve patient outcomes. The results, published in the March 5th issue of the Journal of Clinical Oncology, showed that the vincristine/irinotecan combination is highly active. Out of the group, 78% of patients who received this combination had an objective tumor response.
The study also demonstrated that additional chemotherapy drugs can reduce the rate of relapse, but it is likely that we have reached the limit of what children can tolerate. “Future gains will likely be made by using agents with novel mechanisms of action, such as immunotherapy and new drugs that target the molecular abnormalities of Wilms tumor cells,” says Dr. Dome.
Moreover, the additional chemotherapy agents improved cancer-free survival rates to levels unprecedented for diffuse anaplastic Wilms tumor. However, the decrease in relapse rate came at the cost of increased toxicity.
“The study was impactful because it established the activity of vincristine/irinotecan against Wilms tumor. Based on these findings, this chemotherapy combination will be applied more broadly in the treatment of Wilms tumor,” Dr. Dome added.
Children’s National Hospital collects patients’ blood, extracts T-cells and replicates them in the presence of specific proteins found on cancer cells which, in essence, teaches the T-cells to target specific tumor markers. Training the T-cells, growing them to sufficient quantities and ensuring they are safe for administration takes weeks. But when patients return to the outpatient clinic, their T-cell infusion lasts just a few minutes.
For the third consecutive year, Children’s National was selected to compete in STAT Madness, an annual bracket-style competition that chooses the year’s most impactful biomedical innovation by popular vote. Children’s entry, “Immunotherapy of relapsed and refractory solid tumors with ex vivo expanded multi-tumor associated antigen specific cytotoxic T lymphocytes,” uses the body’s own immune system to attack and eliminate cancer cells in pediatric and adult patients with solid tumor malignancies.
In 2018, Children’s first-ever STAT Madness entry advanced through five brackets in the national competition and, in the championship round, finished second. That innovation, which enables more timely diagnoses of rare diseases and common genetic disorders, helping to improve kids’ health outcomes around the world, also was among four “Editor’s Pick” finalists, entries that spanned a diverse range of scientific disciplines.
An estimated 11,000 new cases of pediatric cancer were diagnosed in children 14 and younger in the U.S. in 2019. And, when it comes to disease, cancer remains the leading cause of death among children, according to the National Institutes of Health. An enterprising research team led by Children’s National faculty leveraged T-cells – essential players in the body’s immune system – to treat pediatric and adult patients with relapsed or refractory solid tumors who had exhausted all other therapeutic options.
“We’re using the patient’s own immune system to fight their cancer, rather than more traditional chemotherapy drugs,” says Catherine M. Bollard, M.D., director of the Center for Cancer & Immunology Research at Children’s National and co-senior author of the study. “It’s more targeted and less toxic to the patient. These T-cells home in on any cancer cells that might be in the body, allowing healthy cells to continue to grow,” Dr. Bollard adds.
That means patients treated in the Phase I, first-in-human trial didn’t lose their hair and weren’t hospitalized for the treatment. After a quick clinical visit for their treatment, they returned to normal activities, like school, with good energy levels.
“With our specially trained T-cell therapy, many patients who previously had rapidly progressing disease experienced prolonged disease stabilization,” says Holly J. Meany, M.D., a Children’s National oncologist and the study’s co-senior author. “Patients treated at the highest dose level showed the best clinical outcomes, with a six-month, progression-free survival of 73% after tumor-associated antigen cytotoxic T-cell (TAA-T) infusion, compared with 38% with their immediate prior therapy.”
The multi-institutional team published their findings from the study online July 29, 2019, in the Journal of Clinical Oncology.
“Our research team and our parents are delighted that some patients treated in our study continue to do well following T-cell therapy without additional treatment. In some cases, two years after treatment, patients do not appear to have active disease and are maintaining an excellent quality of life,” says Amy B. Hont, M.D., the study’s lead author. “One of these was a patient whose parents were told his only other option was palliative care. Our innovation gives these families new hope,” Dr. Hont adds.
The 2020 STAT Madness #Core64 bracket opened March 2, and the champion will be announced April 6.
In addition to Drs. Hont, Meany and Bollard, Children’s National co-authors include C. Russell Cruz, M.D., Ph.D., Robert Ulrey, MS, Barbara O’Brien, BS, Maja Stanojevic, M.D., Anushree Datar, MS, Shuroug Albihani, MS, Devin Saunders, BA, Ryo Hanajiri, M.D., Ph.D., Karuna Panchapakesan, MS, Payal Banerjee, MS, Maria Fernanda Fortiz, BS, Fahmida Hoq, MBBS, MS, Haili Lang, M.D., Yunfei Wang, DrPH, Patrick J. Hanley, Ph.D., and Jeffrey S. Dome, M.D., Ph.D.; and Sam Darko, MS, National Institute of Allergy and Infectious Diseases.
Financial support for the research described in this post was provided by the Children’s National Hospital Heroes Gala, Alex’s Army Foundation, the Children’s National Board of Visitors and Hyundai Hope on Wheels Young Investigator Grant to Support Pediatric Cancer Research, the Children’s National Research Institute Bioinformatics Unit, the Clinical and Translational Science Institute and the National Institutes of Health under award No. UL1-TR001876.
Of the 200 million people around the globe infected with Schistosomiasis, about 100 million of them were sickened by the parasite Schistosoma haematobium.
Of the 200 million people around the globe infected with Schistosomiasis, about 100 million of them were sickened by the parasite Schistosoma haematobium. As the body reacts to millions of eggs laid by the blood flukes, people can develop fever, cough and abdominal pain, according to the Centers for Disease Control and Prevention. Schistosomiasis triggered by S. haematobium can also include hematuria, bladder calcification and bladder cancer.
Despite the prevalence of this disease, there are few experimental models specifically designed to study it, and some tried-and-true preclinical models don’t display the full array of symptoms seen in humans. It’s also unclear how S. haematobium eggs deposited in the host bladder modulate local tissue gene expression.
To better understand the interplay between the parasite and its human host, a team led by Children’s National Hospital injected 6,000 S. haematobium eggs into the bladder wall of seven-week-old experimental models.
After four days, they isolated RNA for analysis, comparing differences in gene expression in various treatment groups, including those that had received the egg injection and experimental models whose bladders were not exposed to surgical intervention.
Using the Database for Annotation, Visualization and Integrated Discovery (DAVID) – a tool that helps researchers understand the biological meaning of a long list of genes – the team identified commonalities with other pathways, including malaria, rheumatoid arthritis and the p53 signaling pathway, the team recently presented during the American Society of Tropical Medicine and Hygiene 2019 annual meeting. Some 325 genes were differentially expressed, including 34 genes in common with previous microarray data.
“Of particular importance, we found upregulation in genes associated with inflammation and fibrosis. We also now know that the body may send it strongest response on the first day it encounters a bolus of eggs,” says Michael Hsieh, M.D., Ph.D., director of transitional urology at Children’s National, and the research project’s senior author. “Next, we need to repeat these experiments and further narrow the list of candidate genes to key genes associated with immunomodulation and bladder cancer.”
In addition to Dr. Hsieh, presentation co-authors include Lead Author Kenji Ishida, Children’s National; Evaristus Mbanefo and Nirad Banskota, National Institutes of Health; James Cody, Vigene Biosciences; Loc Le, Texas Tech University; and Neil Young, University of Melbourne.
Financial support for research described in this post was provided by the National Institutes of Health under award No. R01-DK113504.
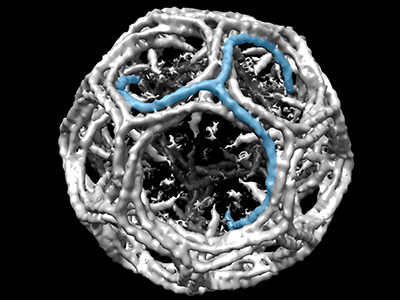
IPSE, one of the important proteins excreted by the parasite Schistosoma mansoni, infiltrates human cellular nuclei through clathrin-coated vesicles, like this one.
IPSE, one of the important proteins excreted by the parasite Schistosoma mansoni infiltrates human cellular nuclei through clathrin-mediated endocytosis (a process by which cells absorb metabolites, hormones and proteins), a research team led by Children’s National Hospital reported during the American Society of Tropical Medicine and Hygiene 2019 annual meeting.
Because the public health toll from the disease this parasite causes, Schistosomiasis, is second only to malaria in global impact, research teams have been studying its inner workings to help create the next generation of therapies.
In susceptible host cells – like urothelial cells, which line the urinary tract – IPSE modulates gene expression, increasing cell proliferation and angiogenesis (formation of new blood vessels). On a positive note, neurons appear better able to fend off its nucleus-infiltrating ways.
“We know that IPSE contributes to the severity of symptoms in Schistosomiasis, which leads some patients to develop bladder cancer, which develops from the urothelial lining of the bladder. Our team’s carefully designed experiments reveal IPSE’s function in the urothelium and point to the potential of IPSE playing a therapeutic role outside of the bladder,” says Michael Hsieh, M.D., Ph.D., director of transitional urology at Children’s National and the research project’s senior author.
In addition to Dr. Hsieh, research co-authors include Evaristus Mbanefo, Ph.D.; Kenji Ishida, Ph.D.; Austin Hester, M.D.; Catherine Forster, M.D.; Rebecca Zee, M.D., Ph.D.; and Christina Ho, M.D., all of Children’s National; Franco Falcone, Ph.D., University of Nottingham; and Theodore Jardetzky, Ph.D., and Luke Pennington, M.D., Ph.D., candidate, both of Stanford University.
Financial support for research described in this post was provided by the National Institutes of Health under award No. R01-DK113504.


Recently, Kurt Newman, M.D., president and CEO of Children’s National Hospital, authored an opinion piece for the popular political website, The Hill. In the article, he called upon stakeholders from across the landscape to address the significant innovation gap in children’s healthcare versus adults.
As Chair of the Board of Trustees of the Children’s Hospital Association, Dr. Newman knows the importance of raising awareness among policy makers at the federal and state level about the healthcare needs of children. Dr. Newman believes that children’s health should be a national priority that is addressed comprehensively. With years of experience as a pediatric surgeon, he is concerned by the major inequities in the advancements of children’s medical devices and technologies versus those for adults. That’s why Children’s National is working to create collaborations, influence policies and facilitate changes that will accelerate the pace of pediatric healthcare innovation for the benefit of children everywhere. One way that the hospital is tackling this challenge is by developing the Children’s National Research & Innovation Campus, which will be the nation’s first innovation campus focused on pediatric research.
Malignant peripheral nerve sheath tumors (MPNST) are aggressive soft tissue sarcomas and the most common malignancy associated with neurofibromatosis type 1 (NF1).
Malignant peripheral nerve sheath tumors (MPNST) are aggressive soft tissue sarcomas and the most common malignancy associated with neurofibromatosis type 1 (NF1). Half of all MPNST are seen in NF1 patients, and MPNST is a leading cause of mortality in young patients with NF1. Researchers led by AeRang Kim, M.D., Ph.D., a pediatric oncologist at Children’s National Hospital, are now searching for a medical treatment for this rare disease that currently has dismal survival rates.
“Through consortia efforts, we’ve been able to open and accrue in single histology trials of really rare diseases such as MPNST for which there are no known curative therapies other than surgery, and surgery is very difficult or not feasible in many patients,” says Dr. Kim, the principal investigator for the SARC031 trial sponsored by the Sarcoma Alliance for Research through Collaboration. “In this trial in particular, our hope is to find a new therapy that will benefit patients with MPNST for which we have no known effective medical therapies.”
Using a combination of drugs that target specific pathways involved in MPNST growth, Dr. Kim and colleagues at four other institutions offering the SARC031 trial will monitor patients to see if the drugs shrink, slow down or stop the growth of MPNSTs. Based on preclinical data demonstrating substantial MPNST shrinkage in mice treated with a combination of MEK and mTOR inhibitors, SARC031 is a trial of the MEK inhibitor selumetinib in combination with the mTOR inhibitor sirolimus for patients with unresectable or metastatic MPNST. The primary objective is to determine the clinical benefit of the combination.
SARC031: A Phase 2 Trial of the MEK Inhibitor Selumetinib (AZD6244 Hydrogen Sulfate) in Combination with the mTOR Inhibitor Sirolimus for Patients with Unresectable or Metastatic Malignant Peripheral Nerve Sheath Tumors
For more information about this trial, contact:
AeRang Kim, M.D., Ph.D.
202-476-2800
AeKim@childrensnational.org
Click here to view Open Phase 1 and 2 Cancer Clinical Trials at Children’s National.
The Children’s National Center for Cancer and Blood Disorders is committed to providing the best care for pediatric patients. Our experts play an active role in innovative clinical trials to advance pediatric cancer care. We offer access to novel trials and therapies, some of which are only available here at Children’s National. With research interests covering nearly aspect of pediatric cancer care, our work is making great advancements in childhood cancer.

Children’s National Hospital and Virginia Tech create formal partnership that includes the launch of a Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus.
Children’s National Hospital and Virginia Tech recently announced a formal partnership that will include the launch of a 12,000-square-foot Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus. The campus is an expansion of Children’s National that is located on a nearly 12-acre portion of the former Walter Reed Army Medical Center in Washington, D.C. and is set to open its first phase in December 2020. This new collaboration brings together Virginia Tech, a top tier academic research institution, with Children’s National, a U.S. News and World Report top 10 children’s hospital, on what will be the nation’s first innovation campus focused on pediatric research.

“Virginia Tech is an ideal partner to help us deliver on what we promised for the Children’s National Research & Innovation Campus – an ecosystem that enables us to accelerate the translation of potential breakthrough discoveries into new treatments and technologies,” says Kurt Newman, M.D., president and CEO, Children’s National. “Our clinical expertise combined with Virginia Tech’s leadership in engineering and technology, and its growing emphasis on biomedical research, will be a significant advance in developing much needed treatment and cures to save children’s lives.”
Earlier this year, Children’s National announced a collaboration with Johnson & Johnson Innovation LLC to launch JLABS @ Washington, DC at the Research & Innovation Campus. The JLABS @ Washington, DC site will be open to pharmaceutical, medical device, consumer and health technology companies that are aiming to advance the development of new drugs, medical devices, precision diagnostics and health technologies, including applications in pediatrics.
“We are proud to welcome Virginia Tech to our historic Walter Reed campus – a campus that is shaping up to host some of the top minds, talent and innovation incubators in the world,” says Washington, D.C. Mayor Muriel Bowser. “The new Children’s National Research & Innovation Campus will exemplify why D.C. is the capital of inclusive innovation – because we are a city committed to building the public and private partnerships necessary to drive discoveries, create jobs, promote economic growth and keep D.C. at the forefront of innovation and change.”
Faculty from the Children’s National Research Institute and the Fralin Biomedical Research Institute at Virginia Tech Carilion (VTC) have worked together for more than a decade, already resulting in shared research grants, collaborative publications and shared intellectual property. Together, the two institutions will now expand their collaborations to develop new drugs, medical devices, software applications and other novel treatments for cancer, rare diseases and other disorders.
“Joining with Children’s National in the nation’s capital positions Virginia Tech to improve the health and well-being of infants and children around the world,” says Virginia Tech President Tim Sands, Ph.D. “This partnership resonates with our land-grant mission to solve big problems and create new opportunities in Virginia and D.C. through education, technology and research.”
The partnership with Children’s National adds to Virginia Tech’s growing footprint in the Washington D.C. region, which includes plans for a new graduate campus in Alexandria, Va. with a human-centered approach to technological innovation. Sands said the proximity of the two locations – just across the Potomac – will enable researchers to leverage resources, and will also create opportunities with the Virginia Tech campus in Blacksburg, Va. and the Virginia Tech Carilion Health Science and Technology campus in Roanoke, Va.
Carilion Clinic and Children’s National have an existing collaboration for provision of certain specialized pediatric clinical services. The more formalized partnership between Virginia Tech and Children’s National will drive the already strong Virginia Tech-Carilion Clinic partnership, particularly for children’s health initiatives and facilitate collaborations between all three institutions in the pediatric research and clinical service domains.
Children’s National and Virginia Tech will engage in joint faculty recruiting, joint intellectual property, joint training of students and fellows, and collaborative research projects and programs according to Michael Friedlander, Ph.D., Virginia Tech’s vice president for health sciences and technology, and executive director of the Fralin Biomedical Research Institute at VTC.
“The expansion and formalization of our partnership with Children’s National is extremely timely and vital for pediatric research innovation and for translating these innovations into practice to prevent, treat and ultimately cure nervous system cancer in children,” says Friedlander, who has collaborated with Children’s National leaders and researchers for more than 20 years. “Both Virginia Tech and Children’s National have similar values and cultures with a firm commitment to discovery and innovation in the service of society.”
“Brain and other nervous system cancers are among the most common cancers in children (alongside leukemia),” says Friedlander. “With our strength in neurobiology including adult brain cancer research in both humans and companion animals at Virginia Tech and the strength of Children’s National research in pediatric cancer, developmental neuroscience and intellectual disabilities, this is a perfect match.”
The design of the Children’s National Research & Innovation Campus not only makes it conducive for the hospital to strengthen its prestigious partnerships with Virginia Tech and Johnson & Johnson, it also fosters synergies with federal agencies like the Biomedical Advanced Research and Development Authority, which will collaborate with JLABS @ Washington, DC to establish a specialized innovation zone to develop responses to health security threats. As more partners sign on, this convergence of key public and private institutions will accelerate discoveries and bring them to market faster for the benefit of children and adults.
“The Children’s National Research & Innovation Campus pairs an inspirational mission to find new treatments for childhood illness and disease with the ideal environment for early stage companies. I am confident the campus will be a magnet for big ideas and will be an economic boost for Washington DC and the region,” says Jeff Zients, who was appointed chair of the Children’s National Board of Directors effective October 1, 2019. As a CEO and the former director of President Obama’s National Economic Council, Zients says that “When you bring together business, academia, health care and government in the right setting, you create a hotbed for innovation.”
Ranked 7th in National Institutes of Health research funding among pediatric hospitals, Children’s National continues to foster collaborations as it prepares to open its first 158,000-square-foot phase of its Research & Innovation Campus. These key partnerships will enable the hospital to fulfill its mission of keeping children top of mind for healthcare innovation and research while also contributing to Washington D.C.’s thriving innovation economy.


When asked about this award, Dr. Pei noted “I am so deeply grateful to receive this support from the V Foundation for Cancer Research…I will use these resources to aid our goal of discovering new therapies to treat medulloblastoma.”
Yanxin Pei, Ph.D., assistant professor in the Brain Tumor Institute and the Children’s Research Institute at Children’s National Hospital in Washington, D.C., has recently been awarded a prestigious grant by the V Foundation for Cancer Research to support her groundbreaking work in finding new treatments for childhood medulloblastoma.
Dr. Pei, who joined Children’s National in 2014 after training in the Wechsler-Reya lab at the Sanford-Burnham Institute in La Jolla, CA, has focused her work on the biology of medulloblastoma, the most common malignant brain tumor in children, with a major emphasis on the study of the medulloblastoma subtype most resistant to treatment. Children with this form of medulloblastoma have less than a 30% chance of survival five years from their diagnosis.
Having already developed one of the most important mouse models of this disease, Dr. Pei’s present V Foundation for Cancer Research Award, which includes becoming a V scholar, will explore the role of metabolism in the development of metastasis in MYC-amplified medulloblastomas (the most virulent form of medulloblastoma).
The V Foundation for Cancer Research Award is one of a series of prestigious awards Dr. Pei has received over the past 18 months for her work, including an NIH-sponsored 5-year award (ROI) evaluating other aspects of medulloblastoma development and resistance to therapy, and grants from the Rally Foundation, the Meghan Rose Bradley Foundation and the Children’s Cancer Foundation.
When asked about this award, Dr. Pei noted “I am so deeply grateful to receive this support from the V Foundation for Cancer Research…I will use these resources to aid our goal of discovering new therapies to treat medulloblastoma.”
Her cutting-edge work is generating national and international attention and firmly places Dr. Pei as an international leader in medulloblastoma research.
A new study suggests that medulloblastoma-specific germline microsatellite variations mark those at-risk for medulloblastoma development.
Brian Rood, M.D., oncologist and medical director at the Brain Tumor Institute, and Harold “Skip” Garner, Ph.D., associate vice provost for research development at Edward Via College of Osteopathic Medicine, published a report in the Society for Neuro-Oncology’s Neuro-Oncology Journal about using a novel approach to identify specific markers in germline (non-tumor) DNA called microsatellites that can differentiate children who have the brain tumor medulloblastoma (MB) from those who don’t.
“Ultimately, the best way to save children from brain tumors and prevent them from bearing long-term side effects from treatment is to prevent those tumors from occurring in the first place,” says Dr. Rood. “New advancements hold the potential to finally realize the dream of cancer prevention, but we must first identify those children at-risk.”
While analyzing germline sequencing data from a training set of 120 MB subjects and 425 controls, the doctors identified 139 individual microsatellites whose genotypes differ significantly between the groups. Using a genetic algorithm, they were able to construct a subset of 43 microsatellites that distinguish MB subjects from controls with a sensitivity and specificity of 92% and 88% respectively.
“We made discoveries in an untapped part of the human genome, enabled by unique bioinformatics data mining approaches combined with clinical insight,” said Dr. Garner. “Our findings establish new genomic directions that can lead to high accuracy diagnostics for predicting susceptibility to medulloblastoma.”
What the doctors discovered and demonstrated in the study was that MB-specific germline microsatellite variations mark those at risk for MB development and suggest that other mechanisms of cancer predisposition beyond heritable mutations exist for MB.
“This work is the first to demonstrate the ability of specific DNA sequences to differentiate children with cancer from their healthy counterparts,” added Dr. Rood.
Contributing Authors to this research study included: Brian R. Rood, M.D., Harold R. Garner, Ph.D., Samuel Rivero-Hinojosa, Ph.D., and Nicholas Kinney, Ph.D.


The Center at Sibley offers state-of-the-art, pencil beam proton therapy equipment, as well as next-generation imaging technologies such as dual energy CT-guided treatment that reduces the range of error, and the latest innovation in biomatrix magnetic resonance imaging designed to target moving tumors in organs like the lung and liver.
Pediatric cancer patients in the Greater Washington region now have access to one of the most advanced, lifesaving proton therapy technologies offered in the U.S. The Johns Hopkins Proton Therapy Center opened Oct.28, 2019, at Sibley Memorial Hospital in collaboration with Children’s National Hospital.
The proton collaboration with Children’s National expands an existing collaboration between Children’s National and Johns Hopkins Medicine that established the pediatric radiation oncology program at Sibley, which treats a wide range of children’s cancer. Now, Sibley will offer the only proton center in the Washington D.C. region with a dedicated pediatric team, staff who are trained in pediatrics instead of adult providers who also treat children.
“This collaboration allows us to bring the latest technology to the region and offer the most advanced cancer treatment to help children live better lives,” says Kurt Newman, M.D., president and CEO at Children’s National. “As one of the Top 10 children’s hospitals in the nation, our goal is to ensure that patients and families are receiving the best care possible.”
The Center at Sibley offers state-of-the-art, pencil beam proton therapy equipment, as well as next-generation imaging technologies such as dual energy CT-guided treatment that reduces the range of error, and the latest innovation in biomatrix magnetic resonance imaging designed to target moving tumors in organs like the lung and liver. A large mechanical arm called a gantry can move the beam 360 degrees around the patient, treating the tumor from several angles as it destroys tumor cells layer by layer.
“Proton therapy is an advanced technology that allows radiation to be delivered precisely to cancer tissue,” says Jeffrey Dome, M.D., Ph.D., vice president for Cancer and Blood Disorders at Children’s National. “This provides a significant advantage compared with conventional radiation therapy, especially in children, where sparing the healthy tissue that surrounds the tumor may be critical for normal growth and development. Proton therapy shows great promise to reduce long-term side effects of radiation treatment.”
The Center at Sibley will have a fully integrated research room, which will allow clinical, basic science and medical physics faculty to advance clinical trial research, translational research and technology development research in proton therapy. Leading experts and oncologists will study proton outcomes for sarcoma, gynecological tumors, pancreatic and liver tumors, lymph node cancers and tumors located near the heart and major blood vessels, such as lung or breast cancers. In addition, the researchers will examine how the proton energy that kills cancer cells interacts with non-cancerous cells and tissue surrounding the tumors.
The JJohns Hopkins Proton Therapy Center opens in phases. The first treatment room opened October 2019. The second room is scheduled to open in spring 2020, and the third room and fixed beam research room are scheduled to open in fall 2020.
Mihailo Kaplarevic, Ph.D., the newly minted Chief Research Information Officer at Children’s National Hospital and Bioinformatics Division Chief at Children’s National Research Institute, will provide computational support, advice, informational guidance, expertise in big data and data analyses for researchers and clinicians.
Kaplarevic’s new job is much like the role he played most recently at the National Heart, Lung and Blood Institute (NHLBI), assembling a team of researchers and scientists skilled in computing and statistical analyses to assist as in-house experts for other researchers and scientists.
NHLBI was the first institute within the National Institutes of Health (NIH) family to set up a scientific information office. During his tenure, a half-dozen other NIH institutions followed, setting up the same entity to help bridge the enormous gap between basic and clinical science and everything related to IT.
“There is a difference compared with traditional IT support at Children’s National – which will remain in place and still do the same sort of things they have been doing so far,” he says of The Bear Institute for Health Innovation. “The difference is this office has experience in research because every single one of us was a researcher at a certain point in our career: We are published. We applied for grants. We lived the life of a typical scientist. On top of that, we’re coming from the computational world. That helps us bridge the gaps between research and clinical worlds and IT.”
Ultimately, he aims to foster groundbreaking science by recognizing the potential to enhance research projects by bringing expertise acquired over his career and powerful computing tools to help teams achieve their goals in a less expensive and more efficient way.
“I have lived the life of a typical scientist. I know exactly how painful and frustrating it can be to want to do something quickly and efficiently but be slowed by technological barriers,” he adds.
As just one example, his office will design the high-performance computing cluster for the hospital to help teams extract more useful clinical and research data with fewer headaches.
Right now, the hospital has three independent clinical systems storing patient data; all serve a different purpose. (And there are also a couple of research information systems, also used for different purposes.) Since databases are his expertise, he will be involved in consolidating data resources, finding the best way to infuse the project with the bigger-picture mission – especially for translational science – and creating meaningful, actionable reports.
“It’s not only about running fewer queries,” he explains. “One needs to know how to design the right question. One needs to know how to design that question in a way that the systems could understand. And, once you get the data back, it’s a big set of things that you need to further filter and carefully shape. Only then will you get the essence that has clinical or scientific value. It’s a long process.”
As he was introduced during a Children’s National Research Institute faculty meeting in late-September 2019, Kaplarevic joked that his move away from pure computer science into a health care and clinical research domain was triggered by his parents: “When my mom would introduce me, she would say ‘My son is a doctor, but not the kind of doctor who helps other people.’ ”
Some of that know-how will play out by applying tools and methodology to analyze big data to pluck out the wheat (useful data) from the chaff in an efficient and useful way. On projects that involve leveraging cloud computing for storing massive amounts of data, it could entail analyzing the data wisely to reduce its size when it comes back from the cloud – when the real storage costs come in. “You can save a lot of money by being smart about how you analyze data,” he says.
While he expects his first few months will be spent getting the lay of the land, understanding research project portfolios, key principal investigators and the pediatric hospital’s biggest users in the computational domain, he has ambitious longer-term goals.
“Three years from now, I would like this institution to say that the researchers are feeling confident that their research is not affected by limitations related to computer science in general. I would like this place to become a very attractive environment for up-and-coming researchers as well as for established researchers because we are offering cutting-edge technological efficiencies; we are following the trends; we are a secure place; and we foster science in the best possible way by making computational services accessible, affordable and reliable.”
Previously, researchers discovered that loss of heterozygosity (LOH) on chromosomes 1 and 16 is associated with a significantly increased risk of relapse of Wilms tumor.
About 650 children are diagnosed each year in the U.S. with Wilms tumor, the most common pediatric kidney cancer. The vast majority of patients respond well to the current standard of care involving a combination of surgery, chemotherapy and radiation. However, approximately 20% of patients with “favorable histology” Wilms tumor experience recurrence.
Previously, researchers discovered that loss of heterozygosity (LOH) on chromosomes 1 and 16 is associated with a significantly increased risk of relapse. A research team in the Children’s Oncology Group (COG), led by Jeffrey Dome, M.D., Ph.D., vice president of the Center for Cancer and Blood Disorders at Children’s National Hospital, sought to determine whether an augmented chemotherapy regimen can overcome the negative effect of LOH.
More than 2,500 patients with Wilms tumor were enrolled in the biology and classification study over a 7–year period. Tumor tissue was tested for LOH and patients with LOH at both chromosomes 1 and 16 received more intensive chemotherapy regimens compared to the standard approach. The results showed that the increased treatment provided a statistically significant benefit in the 4-year event-free survival, with trends toward improved overall survival. For low-stage disease (stage I-II), the four-year event-free survival was 87.3%, compared to a historical rate of 68.8%. Similarly, for advanced stage disease (stage III/IV) four-year event-free survival was 90.2%, compared with 61.3% historically.
Although the new regimens involved additional chemotherapy agents compared to the standard regimens, the short-term toxicities were expected and manageable. There is an increased risk of long-term toxicity including infertility and second malignancies, which requires careful discussion with families. Future studies will seek to mitigate these risks with newer chemotherapy agents.
By better understanding which patients might benefit from more intensive treatment regimens through precision medicine, doctors can tailor therapy according to the risk of relapse, Dr. Dome says.
“This study represents a significant milestone in the treatment of Wilms tumor because it is the first to demonstrate that patient outcome can be improved using a molecular biomarker to guide treatment,” he explains. “We have entered the age of precision medicine for Wilms tumor.”


Lee Savio Beers, M.D., FAAP, Medical Director of Community Health and Advocacy at the Child Health Advocacy Institute (CHAI) at Children’s National Hospital carved out a Monday morning in late-September 2019, as she knew the American Academy of Pediatrics (AAP) would announce the results of its presidential election, first by telephone call, then by an email to all of its members. Her husband blocked off the morning as well to wait with her for the results. She soon got the call that she was elected by her peers to become AAP president-elect, beginning Jan. 1, 2020. Dr. Beers will then serve as AAP president in 2021 for a one-year term.
That day swept by in a rush, and then the next day she was back in clinic, caring for her patients, some of them teenagers whom she had taken care of since birth. Seeing children and families she had known for such a long time, some of whom had complex medical needs, was a perfect reminder of what originally motivated Dr. Beers to be considered as a candidate in the election.
“When we all work together – with our colleagues, other professionals, communities and families – we can make a real difference in the lives of children. So many people have reached out to share their congratulations, and offer their support or help. There is a real sense of collaboration and commitment to child health,” Dr. Beers says.
That sense of excitement ripples through Children’s National.
“Dr. Beers has devoted her career to helping children. She has developed a national advocacy platform for children. I can think of no better selection for the president-elect role of the AAP. She will be of tremendous service to children within AAP national leadership,” says Kurt Newman, M.D., Children’s National Hospital President and CEO.
AAP comprises 67,000 pediatricians, and its mission is to promote and safeguard the health and well-being of all children – from infancy to adulthood.
The daughter of a nuclear engineer and a schoolteacher, Dr. Beers knew by age 5 that she would become a doctor. Trained as a chemist, she entered the Emory University School of Medicine after graduation. After completing residency at the Naval Medical Center, she became the only pediatrician assigned to the Guantanamo Bay Naval Station.
That assignment to Cuba, occurring so early in her career, turned out to be a defining moment that shapes how she partners with families and other members of the team to provide comprehensive care.
“I was a brand-new physician, straight out of residency, and was the only pediatrician there so I was responsible for the health of all of the kids on the base. I didn’t know it would be this way at the time, but it was formative. It taught me to take a comprehensive public health approach to taking care of kids and their families,” she recalls.
On the isolated base, where she also ran the immunization clinic and the nursery, she quickly learned she had to judiciously use resources and work together as a team.
“It meant that I had to learn how to lead a multi-disciplinary team and think about how our health care systems support or get in the way of good care,” she says.
One common thread that unites her past and present is helping families build resiliency to shrug off adversity and stress.
“The base was a difficult and isolated place for some families and individuals, so I thought a lot about how to support them. One way is finding strong relationships where you are, which was important for patients and families miles away from their support systems. Another way is to find things you could do that were meaningful to you.”
Cuba sits where the Atlantic Ocean, Caribbean Sea and Gulf of Mexico meet. Dr. Beers learned how to scuba dive there – something she never would have done otherwise – finding it restful and restorative to appreciate the underwater beauty.
“I do think these lessons about resilience are universal. There are actually a lot of similarities between the families I take care of now, many of whom are in socioeconomically vulnerable situations, and military families when you think about the level of stress they are exposed to,” she adds.
Back stateside in 2001, Dr. Beers worked as a staff pediatrician at the National Naval Medical Center in Bethesda, Maryland, and Walter Reed Army Medical Center in Washington, D.C. In 2003, Dr. Beers joined Children’s National Hospital as a general pediatrician in the Goldberg Center for Community Pediatric Health. Currently, she oversees the DC Collaborative for Mental Health in Pediatric Primary Care, a public-private coalition that elevates the standards of mental health care for all children, and is Co-Director of the Early Childhood Innovation Network. She received the Academic Pediatric Association’s 2019 Public Policy and Advocacy Award.
As a candidate, Dr. Beers pledged to continue AAP’s advocacy and public policy efforts and to further enhance membership diversity and inclusion. Among her signature issues:
“I am humbled and honored to have the support of my peers in taking on this newest leadership role,” says Dr. Beers. “AAP has been a part of my life since I first became a pediatrician, and my many leadership roles in the DC chapter and national AAP have given me a glimpse of the collective good that pediatricians can accomplish by working together toward common strategic goals.”
AAP isn’t just an integral part of her life, it’s where she met her future husband, Nathaniel Beers, M.D., MPA, FAAP, President of The HSC Health Care System. The couple’s children regularly attended AAP meetings with them when they were young.
Just take a glimpse at Lee Beers’ Twitter news feed. There’s a steady stream of images of her jogging before AAP meetings to amazing sunrises, jogging after AAP meetings to stellar sunsets and always, always, images of the entire family, once collectively costumed as The Incredibles.
“I really do believe that we have to set an example: If we are talking about supporting children and families in our work, we have to set that example in our own lives. That looks different for everyone, but as pediatricians and health professionals, we can model prioritizing our families while still being committed to our work,” she explains.
“Being together in the midst of the craziness is just part of what we do as a family. We travel a lot, and our kids have gone with us to AAP meetings since they were infants. My husband even brought our infant son to a meeting at the mayor’s office when he was on paternity leave. Recognizing that not everyone is in a position to be able to do things like that, it’s important for us to do it – to continue to change the conversation and make it normal to have your family to be part of your whole life, not have a separate work life and a separate family life.”


Dr. Bornhorst talks with her patient Maddox Gibson, who is part of the compassionate use trial of selumentinib for which she serves as site principal investigator.
A class of drugs originally approved for stopping tumor growth in adult cancers including melanoma and small cell lung cancer may be the key to treating plexiform neurofibromas in neurofibromatosis type 1 (NF1), too. If effective, doctors will finally have a treatment to offer for children with complicated plexiform neurofibromas that can’t be removed via surgery.
These drugs, including selumentinib, work by inhibiting the activity of the mitogen-activated protein kinase enzymes MEK1 and MEK2. The enzymes have a direct impact on the activity of the cellular signaling pathway MAPK/ERK, which can be overactive some cancers.
Ongoing pre-clinical studies made possible by national and international neurofibromatosis research collaborations demonstrated that this same pathway is overactive in children with NF1 who have plexiform neurofibromas. The compelling findings from these studies set the stage for clinical trials to test the safety and efficacy of selumetinib and other MEK inhibitors as a therapy for pediatric NF1 patients with inoperable plexiform neurofibromas.
At Children’s National, these studies are run by clinicians such as Miriam Bornhorst, M.D., clinical director of the Gilbert Family Neurofibromatosis Institute and AeRang Kim, M.D., Ph.D. Children’s is one of only four sites in the United States to participate in a National Institutes of Health-led clinical trial to study the use of selumetinib in NF1. Dr. Kim is the site principal investigator and Dr. Bornhorst serves as co-principal investigator on phase 2 of the trial.
“Any time we find a medication that works with NF1, we’re excited, especially because for so many years, we didn’t have any of these options for these families,” Dr. Bornhorst says. “We’re offering something these families have never had before – a treatment that may stop growth and maybe even keep these tumors from returning. It means we’re doing more than managing symptoms – we’re really treating them.”
NF1 affects a relatively small number of people, particularly children. However, researchers and clinicians who are dedicated to the condition have banded together via collaborations and consortia to fuel research and development of new therapies across multiple institutions in the U.S. and abroad.
“Patients come to see me who’ve been at our clinic for years and I’ll talk about MEK inhibitors, and they are just shocked to hear there may be a new option,” Dr. Bornhorst says.
The NIH trial continues to collect data at four U.S. centers, with the ultimate goal of submitting the results for FDA review. Additional data is also collected from patients who didn’t qualify for the trial but who received the drug for compassionate use, an effort led by Dr. Bornhorst. The information collected from that compassionate use trial also helps investigators make the case to broaden the eligibility criteria for future trials.
“The medications are showing that they work,” Dr. Bornhorst notes. “Now we need to determine how to identify the patients who we know will need these therapies.”
To meet that need, other studies, led by both Dr. Bornhorst and Dr. Kim, seek radiographic and blood biomarkers that will identify children with NF1 who are more likely to develop plexiform neurofibromas, and whose plexiforms may progress to something malignant.


Protein-coding genes comprise a mere 1% of DNA. While the other 99% of DNA was once derided as “junk,” it has become increasingly apparent that some non-coding genes enable essential cellular functions.
Wei Li, Ph.D., a principal investigator in the Center for Genetic Medicine Research at Children’s National in Washington, D.C., proposes to develop statistical and computational methods that sidestep existing hurdles that currently complicate genome-wide CRISPR/Cas9 screening. The National Institutes of Health has granted him $2.23 million in funding over five years to facilitate the systematic study of genes, non-coding elements and genetic interactions in various biological systems and disease types.
Right now, a large volume of screening data resides in the public domain, however it is difficult to compare data that is stored in one library with data stored at a different library. Over the course of the five-year project, Li aims to:
Ultimately, Li’s work will examine a range of disease types. Take cancer.
“There is abundant information already available in the public domain, like the Project Achilles from the Broad Institute. However, no one is looking to see what is going in inside these tumors,” Li says. “Cancer is a disease of uncontrolled cell growth that makes tumors grow faster.”
Li and colleagues are going to ask which genes control this process by looking at genes that hit the brakes on cell growth as well as genes that pump the gas.
“You knock out one gene and then look: Does the cell grow faster or does it grow more slowly? If the cell grows more slowly, you know you are knocking out a gene that has the potential to stop tumor growth. If cells are growing faster, you know that you’re hitting genes that suppress cancer cell growth.”
In a nutshell, CRISPR (clustered regularly interspaced short palindromic repeats) screens knock out different genes and monitor changes in corresponding cell populations. When CRISPR first became popular, Li decided he wanted to do something with the technology. So, as a Postdoc at Harvard, he developed comprehensive computational algorithms for functional screens using CRISPR/Cas9.
To reach as many people as possible, he offered that MAGeCK/MAGeCK-VISPR software free to as many researchers as possible, providing source code and offering internet tutorials.
“So far, I think there are quite a lot of people using this. There have been more than 40,000 software downloads,” he adds. “It’s really exciting and revolutionary technology and, eventually, we hope the outcomes also will be exciting. We hope to find something really helpful for cancer patients.”
Research reported in this publication was supported by the National Human Genome Research Institute of the National Institutes of Health under award number R01HG010753.
