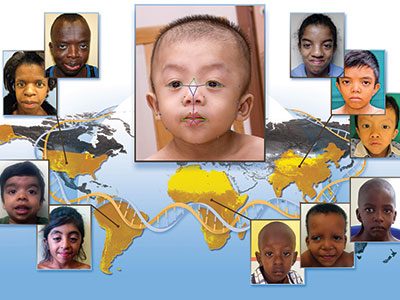
Use of dietary supplements in children with Down syndrome

There is a widespread practice of parents giving dietary supplements to children with Down syndrome in the hope of improving intelligence or function, according to new research published in The Journal of Pediatrics. The study, conducted by experts at Children’s National Rare Disease Institute (CNRDI), examined the prevalence, perceived impact, cost and other factors related to dietary supplement use in children with Down syndrome.
The survey finds nearly half of 1,167 respondents – 49 percent – have given or currently give dietary supplements to their children in an effort to improve health and development. On average, children receive three of the more than 150 supplements reported, with nearly 30 percent of users beginning supplementation before the child’s first birthday.
Amy Feldman Lewanda, M.D., a medical geneticist at CNRDI and lead author on the study, notes that the results also reveal a troubling trend – nearly 20 percent of parents who report using dietary supplements do not inform their pediatrician.
“While we know supplements are given by parents in hopes of improving developmental outcomes for children with Down syndrome, many of these supplements contain concerning ingredient profiles that can have adverse effects in infants and children that are too young to communicate their symptoms,” says Dr. Lewanda. “Additionally, these supplements have no proven safety or efficacy, so it’s important for families to consult with their pediatrician or primary care provider to help determine any risk, ill effects or conflicts with existing treatment.”
Reasons for not informing pediatricians about supplement use vary, according to the study results. The most common reason reported was that the doctor has never specifically asked about nutritional supplements. While some parents indicate they do not view supplement use as important medical information to divulge, others feel that their pediatrician may not be knowledgeable about these types of supplements or may dismiss the practice entirely, as some reportedly have done in the past.

Amy Feldman Lewanda, M.D., a medical geneticist at CNRDI and lead author on the study.
The most popular class of products reported by 25.8 percent of respondents taking supplements are antioxidants, such as curcumin, a byproduct of turmeric, and epigallocatechin-3-gallate (ECGC), the polyphenol compound in green tea. Vitamins, both single and multivitamins, rank second, accounting for 18.9 percent of supplement use. B vitamins were the most popular among single vitamin use. The third most popular supplement category, reported by 15.8 active or previous supplement users, contains proprietary products or combination supplements, such as Nutrivene-D or HAP-CAPS (High Achievement Potential Capsules).
According to Dr. Lewanda, chemical analyses of herbal supplements find some contain anabolic steroids or pharmaceuticals that aren’t listed in the ingredients. Hepatoxicity has been cited among 60 herbs, herbal drugs and herbal supplements. The problem, she notes, is that these products aren’t regulated, like pharmaceuticals are, and similarly, they aren’t thoroughly tested for their safety and efficacy.
The study also notes potential concerns about consuming hyper-concentrated forms of fat-soluble vitamins, including vitamin E and vitamin K, which stay in the body until the vitamins are used. One particular supplement, Speak, provides 5,000 percent of the recommended daily value limits of vitamin E. Fat-soluble vitamins and/or herbal supplements pose unknown health risks – including liver damage.
Among study respondents who actively provide supplements to their children, roughly 87 percent feel they are effective. Those who stopped administering supplements to their children cite lack of efficacy and cost – approximately $90.53 per month on average – as leading reasons for discontinuing use. Approximately 17 percent of respondents note side-effects of supplement use, specifically gastrointestinal disturbance, which was the most common side effect among active and previous supplement users.
“This research gives pediatricians a bit of a wake-up call on what’s trending in the Down syndrome community and the dialogue taking place online, in parent support groups and outside of the doctor’s office,” says Marshall Summar, M.D., director of CNRDI and co-author on the study. “The goal is for pediatricians and parents to work as a team in providing the best care possible for every child, so we hope this research provides physicians greater insight and encourages more open dialogue with patient families about supplement use. Since many of these supplements have active ingredients, it is vitally important that the primary care provider be aware of them.”