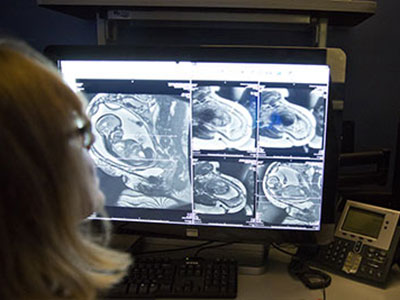
The brain’s fluid-filled spaces during growth

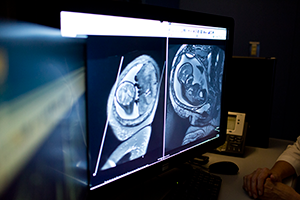
Catherine Limperopoulous, Ph.D., and her colleagues used volumetric MRIs to assess how the ventricles, cerebrospinal fluid and the rest of the fetal brain normally change over time.
The human brain is not one solid mass. Buried within its gray and white matter are a series of four interconnected chambers, called ventricles, which produce cerebrospinal fluid. These ventricles are readily apparent on the fetal ultrasounds that have become the standard of prenatal care in the United States and most developed countries around the world. Abnormalities in the ventricles’ size or shape – or both – can give doctors an early warning that fetal brain development might be going awry.
But what is abnormal? It is not always clear, says Catherine Limperopoulos, Ph.D., director of the Developing Brain Research Laboratory at Children’s National Health System. Limperopoulos explains that despite having many variations in fetal ventricles, some infants have completely normal neurodevelopmental outcomes later. On the other hand, some extremely subtle variations in shape and size can signal problems.
On top of these complications are the tools clinicians typically use to assess the ventricles. Limperopoulos explains that most early indications of ventricle abnormalities come from ultrasounds, but the finer resolution of magnetic resonance imaging (MRI) can provide a more accurate assessment of fetal brain development. Still, both standard MRI and ultrasound provide only two-dimensional pictures, making it difficult to quantify slight differences in the volume of structures.
To help solve these problems, Limperopoulos and her colleagues recently published a paper in Developmental Neuroscience that takes a different tack. The team performed volumetric MRIs – a technique that provides a precise three-dimensional measure of structural volumes – on the brains of healthy fetuses to assess how the ventricles, cerebrospinal fluid and the rest of the brain normally change over time. Limperopoulos’ team recently performed a similar study to assess normal volumetric development in the brain’s solid tissues.
Previous studies published on comparable topics typically used information gathered from subjects who initially had clinical concerns but eventually were dismissed from these studies for not having worrisome diagnoses in the end. This might not truly reflect a typical population of pregnant women, Limperopoulos says.
Working with 166 pregnant women with healthy pregnancies spanning from 18 to 40 weeks gestation, the researchers performed volumetric MRIs on their singleton fetuses that covered every week of this second half of pregnancy. This technique allowed them to precisely calculate the volumes of structures within the fetal brain and get an idea of how these volumes changed over time within the group.
Their results show that over the second and third trimester:
- The lateral ventricles, the largest ventricles found in the cerebrum with one for each brain hemisphere, grew about two-fold;
- The third ventricle, found in the forebrain, grew about 23-fold;
- The fourth ventricle, found in the hindbrain, grew about eight-fold;
- And the extra-axial cerebrospinal fluid, found under the lining of the brain, increased about 11-fold.
The total brain volume increased 64-fold over this time, with the parenchyma – the solid brain tissue that encompasses gray and white matter – growing significantly faster than the cerebrospinal fluid-filled spaces.
Limperopoulos points out that the ability to measure the growth of the brain’s fluid-filled spaces relative to the surrounding brain tissue can provide critical information to clinicians caring for developing fetuses. In most cases, knowing what is normal allows doctors to reassure pregnant women that their fetus’ growth is on track. Abnormalities in these ratios can provide some of the first signals to alert doctors to blockages in cerebrospinal fluid flow, abnormal development, or the loss of brain tissue to damage or disease. Although the neurodevelopmental outcomes from each of these conditions can vary significantly, traditional ultrasounds or MRIs might not be able to distinguish these possibilities from each other. Being able to differentiate why cerebrospinal fluid spaces have abnormal shapes or sizes might allow doctors to better counsel parents, predict neurological outcomes, or potentially intervene before or after birth to mitigate brain damage.
“By developing a better understanding of what’s normal,” Limperopoulos says, “we can eventually identify reliable biomarkers of risk and guide interventions to minimize risks for vulnerable fetuses.”