
New Becker muscular dystrophy drug on the horizon
Muscular dystrophies are a collection of genetic disorders that affect boys and cause progressive loss of muscle strength and disability throughout childhood. They impact the protein dystrophin, and other proteins associated with it, which helps strengthen muscles and protect them from injury.
A new corticosteroid – vamorolone – improves symptoms of Becker muscular dystrophy (BMD) with fewer side effects than the off-label treatments currently offered to patients, according to new research from Children’s National Hospital published in iScience.
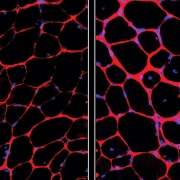
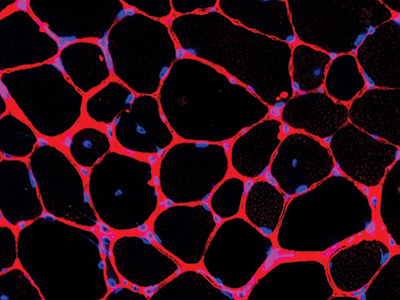
Currently, there are no drugs approved to treat BMD, an inherited disorder that causes progressive muscle weakness. In preclinical models, daily treatment with vamorolone improved muscle strength and structure with results comparable to prednisolone, which is sometimes prescribed to patients with BMD. Unlike prednisolone, vamorolone is not known to stunt growth, weaken bone and cause negative behaviors.
“Patients with muscular dystrophy can fall anywhere on the spectrum from asymptomatic to facing life-threatening cardiac complications,” said Christopher Heier, Ph.D., principal investigator at the Center for Genetic Medicine Research at Children’s National. “We are excited to have our eye on a drug that may help manage the disease progression, without all the harmful side effects of the steroids currently being offered.”
The big picture
Muscular dystrophies are a collection of genetic disorders that affect boys and cause progressive loss of muscle strength and disability throughout childhood. They impact the protein dystrophin, and other proteins associated with it, which helps strengthen muscles and protect them from injury.
The FDA has approved four drugs to help mitigate the impact of Duchenne muscular dystrophy (DMD), the most severe and most common form of the disease, with dozens more drugs in the research pipeline for that disease subtype. In some cases, these drugs convert DMD into BMD, which is less severe but still greatly affects the quality of life. As a result, the number of patients living with BMD is growing, yet only two drugs are being studied to treat the Becker form of the disease.
Why we’re excited
The Food and Drug Administration is nearing approval for vamorolone to treat DMD. Researchers including Nikki McCormack, Ph.D., a postdoctoral fellow at Children’s National, found it has an added characteristic that makes it particularly helpful to BMD. “Excitingly, by reducing inflammatory signaling in the muscle, we find vamorolone can actually help to correct the underlying dystrophin protein deficiency in BMD through a newly discovered RNA-targeting mechanism.”
Investigators at Children’s National have been interested in expanding vamorolone’s possible use to BMD. Their work builds upon research finished late last year, when they created the first preclinical model to study drugs that could treat BMD. The model provides tremendous hope for those suffering from BMD around the world.
“By creating a pre-clinical model to test possible treatments, we are creating hope for boys living with this life-changing disorder,” said Alyson Fiorillo, Ph.D., principal investigator at the Center for Genetic Medicine Research at Children’s National. “This model, and the drugs it will lead to, will revolutionize how we treat those children living with this disorder.”






 Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.





 A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.
A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.



 A
A 




