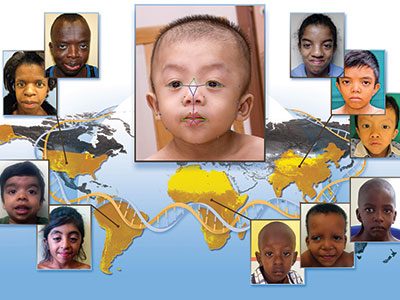
New research on genetic evaluation of short stature, discussed by Andrew Dauber, M.D., M.M.Sc.

In this study, the authors at Shanghai Children’s Medical Center utilized next-generation sequencing (NGS) to analyze the data of patients with short stature to better understand the etiologies of short stature.
Andrew Dauber, M.D., M.M.Sc., division chief of Endocrinology at Children’s National Hospital, shared expert commentary on a recent study published in The Journal of Clinical Endocrinology & Metabolism that explores associated risk factors of short stature as identified by exome sequencing in children.
In this study, the authors at Shanghai Children’s Medical Center utilized next-generation sequencing (NGS) to analyze the data of patients with short stature to better understand the etiologies of short stature.
The big picture
“This was a large-scale study looking at 814 children with short stature and at least one more clinical feature suggestive of a genetic condition who underwent comprehensive genetic testing at Shanghai Children’s Medical Center,” explains Dr. Dauber. In this study, the authors identified a potential genetic etiology in 361 of the patients, which is 44% of the cohort.
“It is important to note that the yield of genetic testing was highly variable depending on the clinical presentation of the child,” said Dr. Dauber. “For example, patients with associated congenital anomalies or a suspected skeletal dysplasia had a diagnostic yield of 56% and 65% respectively, while patients with isolated severe short stature (defined as a height below -3 SDS) only had a yield of 11%.”
Dr. Dauber noted that the overall high yield is reflective of the types of patients who are referred to this specialty center, and the expected yield in a more general pediatric setting is likely much lower.
The patient benefit
“This study helps shed light on the prevalence of those patients in a large cohort of children presenting for evaluation of short stature,” shared Dr. Dauber. “I am hopeful that targeted treatments will improve growth in these children.”
While this study provides new insights into the underlying causes behind short stature in patients with differing phenotypes, the authors indicate that additional large-scale studies on short stature exome sequencing are warranted.
Moving the field forward
Dr. Dauber also pointed to the fact that the authors note a large number of the patients in this study had undiagnosed Rasopathies, such as Noonan syndrome. “There were also 31 patients with FGFR3 mutations, 6 patients found with ACAN (Aggrecan) mutations and 2 with NPR2 mutations,” said Dr. Dauber.
“At Children’s National, we are currently conducting a clinical trial of vosoritide, a novel growth promoting agent which targets the growth plate in children with selected genetic conditions including Noonan syndrome and patients with mutations in FGFR3, ACAN, and NPR2,” included Dr. Dauber. Preliminary results from this clinical trial were recently presented by Dr. Dauber at the Pediatric Endocrine Society annual meeting.
You can read the full study Clinical Profiles and Genetic Spectra of 814 Chinese Children With Short Stature in The Journal of Clinical Endocrinology & Metabolism.