Chief of Cardiac Surgery Yves d’Udekem, M.D., calls this “fourth-dimensional imaging” that identifies if blood flows swiftly, smoothly, or is subjected to swirls or turbulences that impede the effectiveness of the flow.
Cardiac imaging specialists and cardiac surgeons at Children’s National Hospital are applying advanced magnetic resonance imaging visualization techniques to understand the intricacies of blood flow within the heart chambers of children with single ventricle heart defects like hypoplastic left heart syndrome (HLHS).
The data allows surgeons to make critical corrections to the atrioventricular valve — the valve between the atrium and ventricle of the heart — before a child undergoes the single ventricle procedure known as the Fontan.
Yves d’Udekem, M.D., chief of Cardiac Surgery at Children’s National, says that eliminating leakage of the atrioventricular valve before a child undergoes the Fontan may improve a child’s quality of life after Fontan and reduce the likelihood of heart failure, transplant or death long term.
The big picture
Patients with only one functioning pumping chamber, or ventricle, have been on the same treatment trajectory for decades. However, critical international efforts to collect and analyze long-term outcomes for patients with Fontan circulations have led surgeons like d’Udekem to rethink what quality of life and a positive outcome means for these patients. This includes patients in the Australia and New Zealand Fontan Registry founded by d’Udekem while at Royal Children’s Hospital in Australia.
Research based on data in the patient registries shows that atrioventricular valve leakage plays a critical role in the outcomes for patients with single ventricle defects. For children with Fontan circulation, significant leakage of this valve leads to worse outcomes.
Moving the field forward
Treatment decisions for children with single ventricle heart defects are often made based on commonly used heart imaging to determine the effect of valve leakage based on two limited, key variables: the size and the squeeze of the heart. However, this is a late effect and may not reflect the true impact on children with single ventricle hearts.
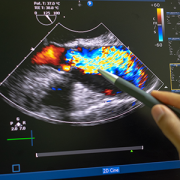
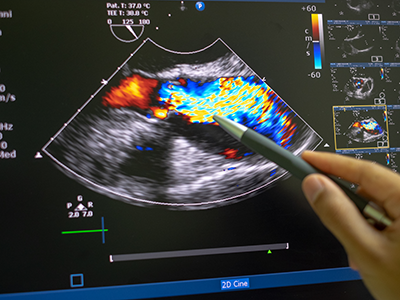
The team at Children’s National — including d’Udekem and Yue-Hin Loke, M.D., cardiac MRI specialist and director of the 3D Cardiac Visualization Laboratory — use cardiac MRI to measure the flow between heart chambers. Special software can measure abnormal flow and energy losses inside the heart, drawing on principles of physics and engineering.
“Dr. Loke not only gathers three-dimensional imaging of the heart through every heartbeat, he also gathers brand new types of colored imaging of blood flow itself, showing how effectively it is propelled by the heart,” says d’Udekem. “This ‘fourth-dimensional imaging’ identifies whether the blood flows swiftly, smoothly or whether it is subjected to swirls or turbulences that impede the effectiveness of the flow.”
Children’s National leads the way
Harnessing the visualization technology and analysis for clinical care of patients with single ventricle defects is relatively new in the United States, but it has become a vital part of the routine, clinical pre-Fontan evaluations at Children’s National.
Few locations in the United States have the mechanisms and expertise to study abnormal flow patterns in children with single ventricle defects. Children’s National collaborates with engineers to help parse the information into clear-cut takeaways for the clinical teams to use in their treatment planning.
Also, while other centers have access to this technology, not many centers have cardiac surgeons like d’Udekem who have an active interest in applying the key learnings from this data as quickly as possible to improve outcomes for patients.
Loke describes the collaboration at Children’s National as a “unique crossroads of clinical need and clinical interest to help these kids in very bold ways.”
What’s next
d’Udekem and Loke are engaged in a comprehensive project that analyzes the impact of atrioventricular valve leakage to ensure that the flow inside the heart is optimized before a Fontan procedure.
The research will map the efficiency of blood flow between the atrium and ventricle before surgery and after a surgical correction is made. The goal is to test the hypothesis that better atrioventricular circulation before Fontan can make a big difference for patients’ long-term quality of life and overall health.














 A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.
A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.











 Children’s National Hospital named
Children’s National Hospital named 

 Children’s National Hospital in Washington, D.C., was ranked No. 5 nationally in the U.S. News & World Report 2022-23 Best Children’s Hospitals annual rankings. This marks the sixth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide. In addition, its
Children’s National Hospital in Washington, D.C., was ranked No. 5 nationally in the U.S. News & World Report 2022-23 Best Children’s Hospitals annual rankings. This marks the sixth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide. In addition, its 


 Children’s National Hospital named
Children’s National Hospital named 

