Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
For the fifteenth straight year, Children’s National ranked in 10 specialty services and is the highest U.S. News ranked children’s hospital in Washington, D.C., Maryland and Virginia. Last year, U.S. News introduced pediatric & adolescent behavioral health as a service line in its rankings. While there are no ordinal rankings for behavioral health, the Children’s National program was named one of the top 50 programs in the country for the second year in a row.
“To be named among the nation’s top children’s hospitals for nine years in a row is a reflection of the extraordinary expertise, innovation and heart that our teams bring to every child and family we serve,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “Our leadership in specialties like neurology, cancer, and diabetes and endocrinology underscores the national impact of our work, and we remain focused on setting new standards in pediatric care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“Being a top-ranked pediatric hospital means more than just excelling in a single specialty — it means being a pillar of outstanding care for your entire region,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Our rankings acknowledge these hospitals for their comprehensive excellence, helping families find the very best care conveniently located within their state and community.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/USNWR_CNBadges_Set2SideBySide_2025-26-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-07 01:00:072026-01-05 17:33:17Children’s National Hospital once again ranked among the nation’s best by U.S. News & World Report
Dr. Franklin joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair.
Children’s National Hospital named Wayne J. Franklin, MD, MBA, as the inaugural A. James & Alice B. Clark Distinguished Professor of Care.
Dr. Franklin serves as senior vice president of the Children’s National Heart and Lung Center, a role he assumed in 2024. He leads a multidisciplinary team delivering high-quality and innovative pediatric cardiac and pulmonary care. Dr Franklin oversees cardiology, cardiac surgery, cardiac intensive care, cardiovascular anesthesia and pulmonary and sleep medicine, including heart and lung transplant services.
This new endowed professorship was made possible through a generous investment from the A. James & Alice B. Clark Foundation.
The big picture
Dr. Franklin joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful to generous donors who have altogether funded 51 professorships.
Professorships support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and the donor’s commitment to advancing and sustaining knowledge.
Why it matters
Dr. Franklin is nationally recognized for his research on adult congenital heart disease, specifically single ventricle-Fontan physiology, neurocognitive outcomes, pulmonary hypertension and cardiac disease in pregnancy. He is committed to advancing pediatric cardiac care through technology and innovation to improve the lives of children and families.
“I am deeply honored to become the A. James & Alice B. Clark Distinguished Professor of Cardiac Care,” Dr. Franklin says. “My goal is to ensure that children born with heart conditions can live full, thriving lives into adulthood. I am committed to advancing the care for patients with heart disease in ways that make a lasting difference for generations to come.”
Moving the field forward
The A. James & Alice B. Clark Foundation, through their vision and generosity, is ensuring that Dr. Franklin and future holders of this professorship will launch bold, new initiatives to advance the field of cardiovascular research and care, elevate our leadership and improve the lifetimes of children and families with congenital heart disease.
The Clark family and the A. James & Alice B. Clark Foundation have been steadfast partners of Children’s National for more than 30 years. Their first transformational investment established the A. James Clark Distinguished Professorship in Molecular Genetics, one of the hospital’s earliest endowed chairs. Since then, their thoughtful and strategic philanthropy has advanced programs that give children healthier childhoods and better outcomes. Their most recent $5 million investment created the A. James & Alice B. Clark Distinguished Professorship in Cardiac Care and will help build a flagship Cardiac Exercise and Rehabilitation Program to improve lifelong outcomes for children with heart disease.
“This professorship is both a vital investment in the future and a celebration of our remarkable partnership with Children’s National,” says Courtney Clark Pastrick, board chair of the A. James & Alice B. Clark Foundation. “With Dr. Franklin as the inaugural chair, I know it will spark discoveries that give children with heart conditions the best possible start in life and the chance to thrive. We are deeply honored to stand behind advancements that truly redefine what’s possible for families.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/Wayne-Franklin-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-09-19 10:14:132026-01-05 17:13:22Wayne J. Franklin, MD, MBA, named as inaugural A. James & Alice B. Clark Distinguished Professor of Cardiac Care
In general, cardiac patients have one of the highest unplanned readmission rates (12%) after going home.
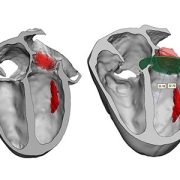
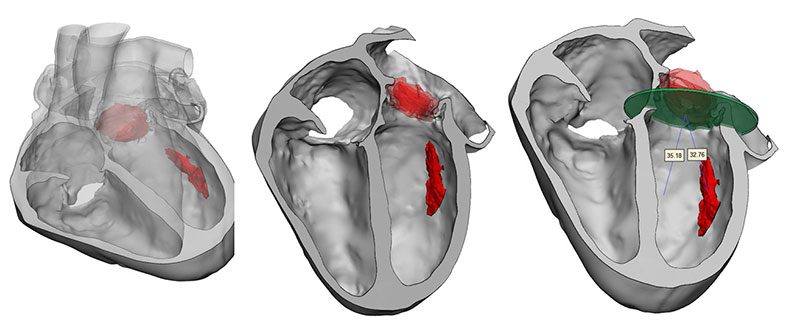
Patients with the heart muscle disease cardiomyopathy and those with single ventricle anatomy are most likely to have an unplanned readmission to the hospital within 30 days of their initial discharge, according to a study published in Pediatric Cardiology.
The study was led by cardiology fellow Michael He, MD, with support from pediatric cardiologists at Children’s National Hospital, including Ashraf Harahsheh, MD, who served as senior author.
What it means
The single center retrospective cohort study reviewed 1,848 hospitalizations that included 223 unplanned readmissions within 30 days of discharge. The authors sought to identify whether directly discharging patients from the Cardiac Intensive Care Unit (CICU) had an impact on readmissions. Typically, cardiac patients are “stepped down” to an acute care inpatient cardiology unit, the Heart and Kidney Unit (HKU) at Children’s National, prior to discharge. When census is high in the HKU, however, some patients can be sent home directly from the CICU.
The analysis showed no connection between CICU-based discharge or HKU-based discharge, but the authors found several other factors that made unplanned readmission more likely:
Single ventricle anatomy
Chromosomal anomaly
Cardiomyopathy
Tube feeding
Increased length of initial stay
Why it matters
In general, cardiac patients have one of the highest unplanned readmission rates (12%) after going home. A deeper dive into the unplanned readmission rates for this group can help care providers identify gaps in discharge instructions and other areas for quality improvement initiatives. The overall goal for these studies is to identify ways to decrease return rates to the hospital for this fragile patient population.
What’s next
The study authors note that multi-center studies of unplanned readmissions would be beneficial to determine if these findings are limited to the specific population mix at Children’s National or if they are somewhat consistent across care centers.
They also recommend that quality improvement initiatives be targeted at patient groups with the highest risk of unplanned readmission, especially those with cardiomyopathy, single ventricle anatomy or those admitted for medical care. The lower unplanned readmission rates for surgical care patients may be due in part to decades of quality improvement initiatives and processes focused on surgical patients, the authors note. “Centers should strive to adapt these processes to medical admissions as well.”
Care providers should also take particular care when assessing discharge readiness and post discharge planning for patients requiring tube feeding and those with chromosomal abnormalities and syndromes, who also had higher risks for unplanned readmissions.
“Our study hopes to lay the foundation for both local and multi-center outcome initiatives to further better the health of our patients,” the authors write.
Other authors from Children’s National include: Maria‑Theresa Balbin, Janet Kreutzer, Jenhao J. Cheng, Janika Peyasena, Lisa Hom, Mary Morgan, Tracy Baust and Yuliya Domnina, MD, medical director for quality and safety in the ICU.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/echocardiogram-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-09-17 15:34:202025-09-17 15:35:29Cardiomyopathy, single ventricle anatomy patients have highest unplanned readmission risk
Mindfulness-based interventions have been widely recognized for their effectiveness in managing stress, anxiety and depression, so the team set out to specifically design the virtual EMBRACE program for adults with CHD. It’s the first of its kind for this population.
A first-of-its-kind virtual, real-time group psychosocial intervention successfully demonstrated the promise of mindfulness interventions to address mental health challenges in adults with congenital heart disease (CHD).
The findings from a small pilot study of the Exploring Mind-Body Resilience and Coping/Cognitive Exercises (EMBRACE) program were published in the journal Pediatric Cardiology.
What this means
The study included 31 participants ranging in age from 22 to 74 years old. Collectively the group had a variety of heart conditions involving 47 heart surgeries, seven pacemakers and one implantable cardioverter defibrillator.
Participants showed meaningful improvements after the EMBRACE intervention in anxiety, depression, resilience and mindfulness scores. Also, satisfaction surveys showed that 97% found the program effective. These improvements lasted through a three-month follow-up period.
“What I gained the most from this study was learning that my emotions/feelings did not have to control my life,” says study participant Tabatha Doherty. “The program taught techniques that focused on keeping your mind in the present and not getting caught up in those feelings.”
Additionally, people who participated reported several positive qualitative outcomes, including better community connections and improved focus on self-care and self-management.
“It was impactful to be in a cohort with other patients where we could talk, share stories, offer support, and work towards a common, yet individual, goal of being able to manage daily and CHD-related stressors,” Doherty continued. “It is very rare that CHD patients have the opportunity to interact with each other, but even more rare to have an opportunity to cooperate towards a common goal.”
Why it matters
The authors write that the lifetime prevalence of anxiety and depression in adults with congenital heart disease are significantly higher than the general population – occurring in up to 30 to 50% of adults with CHD versus only 7 to 10% in the general population.
Mindfulness-based interventions have been widely recognized for their effectiveness in managing stress, anxiety and depression, so the team set out to specifically design the virtual EMBRACE program for adults with CHD. It’s the first of its kind for this population.
The study sought to improve mental health, resilience and coping skills for people with CHD while demonstrating feasibility for a large number of people.
“The most comforting aspect was the acknowledgement and validation of the mental health struggles I’ve had my entire life,” Doherty says. “The statistics they shared were not surprising, but more proof/recognition of the CHD patient’s silent struggles.”
What’s next
The program will be adjusted based on feedback from the pilot cohort and further studies will be undertaken to gauge sustainability and long-term benefits.
The work was made possible through a grant from the Adult Congenital Heart Association (ACHA) with generous support from the Meil Family Foundation.
“ACHA is proud to support groundbreaking research initiatives though our Research Program that began in 2019,” says Mark Roeder, president and CEO of ACHA. “Vicki Freedenberg, PhD, RN was awarded the Meil Family Foundation Research Award for Neurocognitive Studies in 2022. This first-of-its-kind mindfulness-based program for adults with CHD demonstrated meaningful improvements in anxiety, depression, resilience, and self-care – highlighting the critical role of mental health interventions in the CHD population.”
Roeder continued, “The EMBRACE study not only addresses the physical realities of living with CHD but also elevates the importance of mental and emotional well-being, something that ACHA will also continue to promote through our educational programming.”
Before publication in Pediatric Cardiology, the data from EMBRACE was presented as a poster at the American College of Cardiology ACC.24 meeting. Additionally, program and study co-author Rachel Steury, NP, was awarded Best Allied Health Research for this work at the International Society of ACHD in June 2024.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/08/woman-meditating-body.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-08-26 15:55:102025-08-26 15:56:02Results from first-of-its-kind mental health intervention for adults with CHD
DMD is a genetic condition that causes progressive muscle weakness, including in the heart.
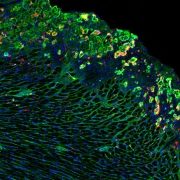
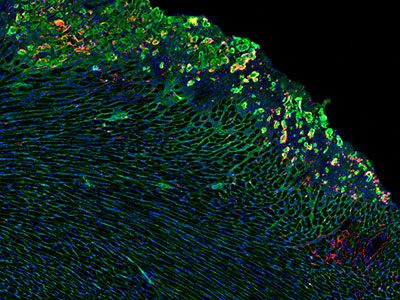
For boys with Duchenne muscular dystrophy (DMD), heart damage can begin early in life, often before symptoms are noticeable. A new study from Children’s National Hospital sheds light on why this happens and points to a promising therapy that could change how doctors protect the hearts and muscles of children living with DMD.
The findings, published in Cell Death & Disease, laid the groundwork for a newly awarded Department of Defense (DoD) clinical and translational research award that will launch in August 2025. This grant will support critical studies needed to advance this therapy toward clinical trials.
The challenge: Protecting growing hearts and muscles
DMD is a genetic condition that causes progressive muscle weakness, including in the heart. Steroids remain the standard treatment for inflammation, but long-term use can slow growth in children, contribute to muscle loss and even interfere with newer gene therapies as boys get older.
“Treating chronic inflammation is essential, but it has to be done in a way that supports cardiac muscle repair and works in concert with other emerging therapies,” says Jyoti Jaiswal, PhD, professor at Children’s National and senior author of the study.
As boys with DMD live longer thanks to exon skipping and micro-dystrophin gene therapies, there is an urgent need for treatments that keep their hearts and muscles healthy.
Understanding early heart damage
In this study, researchers focused on how and why heart damage begins in the absence of dystrophin using a severe model of DMD. They found that the problem is not just inflammation itself, but the failure to turn it off. When inflammation lingers instead of resolving naturally, it leads to scarring and tissue loss in both heart and skeletal muscle.
Instead of relying on steroids to block inflammation, the research team tested a pro-resolution therapy that works to clear inflammation through the natural healing process. The therapy activates formyl peptide receptors, which play a role in naturally switching off inflammation once tissue repair begins.
This approach successfully reduced inflammation, limited scarring and preserved healthy heart and skeletal muscle tissue. Importantly, it may also complement gene therapy approaches, potentially boosting their effectiveness.
“This is a physiological way to help the body finish the healing process,” says James Novak, PhD, associate professor at Children’s National and the lead author of the study. “It allows inflammation to do its job to help repair the tissue and subsequently clear out to prevent chronic inflammation and tissue damage.”
Building toward clinical trials
These findings helped secure a DoD grant through which, the team will pursue investigational new drug (IND)-enabling studies; a critical step toward bringing this therapy to clinical trials for children with DMD.
“This line of research represents a new way of thinking about treating Duchenne,” says Dr. Jaiswal. “We are excited to take the next step in moving it closer to patients.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/08/Jaiswal-Novak-Innov-District-Cardiac-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-08-04 10:24:122026-04-15 16:30:11New study shows resolving inflammation could prevent early heart damage in Duchenne muscular dystrophy
The commentary, appearing in the journal Pediatrics, was drafted by some of the original American Heart Association (AHA) statement authors, including Dr. Harahsheh, to call particular attention to the changes most relevant for pediatric primary care and emergency medicine practitioners.
What it means
The first AHA statement on Kawasaki disease was issued in 2017 and refined an incomplete diagnosis algorithm developed in 2004. That earlier statement outlined coronary arteriopathy stages, addressed treatments for when intravenous immunoglobulin was not effective, introduced coronary risk stratification and tailored long-term management based on whether the coronary artery was affected by the disease.
The 2024 statement sought to incorporate updated evidence and provide new guidance for practitioners based on that new evidence. These updates also consider the appearance of multisystem inflammatory syndrome in children (MIS-C), caused by exposure to SARS-CoV-2 a new condition for consideration as part of differential diagnosis for Kawasaki disease.
Why it matters
Kawasaki disease remains an orphan disease with rare but fatal complications. The 2024 updated statement provided expert analysis of the latest data, and a “roadmap for those suspected to have Kawasaki disease in their primary care provider’s office or in the emergency department” It also refines who is considered high risk for developing coronary artery aneurysm and advocates for intensification of therapy in that group. Finally, the article discusses new anti-coagulation therapies in children with giant coronary artery aneurysm.
According to the commentary authors, identifying possible Kawasaki disease as early as possible, at 4 to 5 days of fever and within 10 days of fever onset, is critical to implement treatments and reduce the risk of coronary artery aneurysms, a potentially deadly complication. This is where informed primary care or emergency department practitioners may be crucial to identifying Kawasaki disease before complications occur.
The commentary also calls attention to short- and long-term care of these patients, including needed follow-up and how primary care and emergency department providers can identify acute coronary syndrome occurring in children with Kawasaki disease at early stages to ensure swift treatment of this complication.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/Kawasaki-disease-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-11 16:27:232026-04-13 10:44:53Commentary calls out important updates to American Heart Association statements on Kawasaki disease
The multi-disciplinary team who implanted the first AVEIR leadless pacemakers at Children’s National.
Two new devices being used in adults with heart rhythm disorders — atrial and dual chamber leadless pacemakers and extravascular defibrillators — were successfully implanted in pediatric patients for the first time at Children’s National. These devices represent the latest technology in pacing and defibrillating the heart to maintain its rhythm. Though they are smaller in size, have fewer complications and longer battery life than most of the devices currently available for young patients, they have not been available for use in these younger patients until recently.
“For the first time, we’re bringing these devices that are smaller, smarter, less painful and more flexible to children and teenagers who can really benefit from them,” says Elizabeth Sherwin, MD, a pediatric cardiologist and electrophysiologist at Children’s National who led the teams completing these minimally invasive procedures.
The patient benefit
Offering implantation of these devices gives more children and adults with congenital heart disease access to the latest technologies in implantable heart rhythm devices, which may offer unique benefits for these groups.
Abbott AVEIR dual chamber leadless pacemaker is the newest FDA approved leadless pacemaker. It uses electricity to maintain heart rhythm and can be used to pace both the top and bottom chambers of the heart, which is particularly important for pediatric and adult congenital patients. These devices also:
Are designed to be removed and replaced after battery runs down, which is ideal for children and young adults who will have multiple replacements over a lifetime.
Long battery life, so fewer replacements may be necessary.
Can be placed minimally invasively
Dr. Sherwin says that the minimally invasive procedure and the lack of leads on these devices are particularly key for younger people because these factors remove or reduce the risk of complications commonly experienced with pacemakers in children. There is a reduced risk of bleeding, infection, lead movement or fracture, and long-term problems with the veins. Even better, because they are placed directly in the heart, there are no scars on the chest or visible signs of a pacemaker present.
Medtronic Aurora EV-ICD is an extravascular implantable cardioverter-defibrillator (ICD), which is implanted under the skin (subcutaneous) with a generator on the left chest wall and a lead that goes under the breastbone (sternum). The design includes:
A smaller generator.
No need to go through chest muscle, leading to less painful implantation and more comfort long term.
Emergency heart pacing through the substernal lead – both to try to terminate a fast arrhythmia to avoid need for a shock, and to treat in case the heartbeat is too slow.
Longer battery life (projected 11 years).
Avoids the need to have leads in the blood vessels, with the many potential complications that go along with transvenous leads.
For both of these newer devices, the patient’s size, weight and medical history will help determine if they are a good candidate.
The big picture
The Electrophysiology team is the first and only pediatric and congenital cardiology team trained to implant AVEIR leadless pacemakers and the Aurora EV-ICD for eligible individuals in the mid-Atlantic region. Dr. Sherwin, Charles Berul, MD, and Tom (Nak) Choi, MD, are trained to provide these procedures for people in Washington, DC, Virginia and Maryland. For both devices, Children’s National is among only a handful of children’s hospitals in the U.S. with the training and expertise to offer access to these technologies.
“This is a game-changer for kids with rhythm disorders and adults with congenital heart disease,” Dr. Sherwin says. “We are really excited to be among the first to offer these options for patients who need them.”
The Children’s National Heart Center team led activities designed to encourage skin-to-skin contact between parents and infants in the Cardiac Intensive Care Unit and Heart and Kidney Unit.
Clinicians at Children’s National Hospital and Children’s Hospital Orange County are leading a nationwide event to encourage families to practice more skin-to-skin, or kangaroo, care with newborn infants who have congenital heart disease, including throughout hospitalization.
Thirty-one hospitals across the United States will participate in this congenital heart disease focused “Skin-to-skin-a-thon,” that will include family and clinical care provider activities and education throughout pediatric cardiac intensive care units and step-down units.
The event will celebrate the tremendous benefits that research shows both families and infants gain from physical contact early in life.
Early skin-to-skin care has been shown to:
Reduce stress in both baby and the parent
Help with baby’s physiologic stability including regulating vital signs like temperature, heart rate, and blood pressure
Provide infant pain relief
Improve infant digestion and weight gain
Support good sleep/wake cycles in babies.
Increase oxytocin for mothers, which can help improve milk production/support breastfeeding
Most studies showing these benefits have included pre-term babies or those born after a healthy term. The idea of encouraging family skin-to-skin care in the hospital setting has been widely adopted in neonatal intensive care units but is not done routinely in cardiac intensive care units. One study estimated that only 6% of parents whose babies were hospitalized for congenital heart disease reported any skin-to-skin care during their stay, with most stays averaging 22 days.
“Research shows so many benefits for all infants and their parents — and our congenital heart newborns stand to gain even more from this type of contact, but often receive it far less,” says Sarah Schlatterer, MD, PhD, medical director of Neurocardiac Critical Care at Children’s National. “This awareness effort is designed to help families understand how to do this safely and also empower our bedside care providers to encourage skin-to-skin care as much as they can every day.”
The event overall is inspired and supported by the Cardiac Newborn Neurodevelopmental Network SIG of the Cardiac Neurodevelopmental Outcomes Collaborative, who planted the seed of the idea and assisted with dissemination of information and coordinating between participating hospitals.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/skin-to-skin-group-photo-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-05-15 16:34:092026-03-02 09:21:02Children’s National co-leads efforts to increase skin-to-skin care for babies with congenital heart disease
An 11-year-old boy is the first in the world to have an artificial heart valve replaced with a live tissue valve from a donated heart through a partial heart transplant. The procedure took place at Children’s National Hospital in Washington, D.C. The successful surgery, performed by the cardiac surgery team, is also the region’s first partial heart transplant.
“I am honored this family trusted our hospital and our team’s expertise to perform this life-changing first-of-its-kind procedure for Preston,” says Cardiac Surgery Chief Yves d’Udekem, MD, PhD. “I look forward to hearing about all the new activities and adventures he and his family can do once he is completely recovered from surgery.”
“Everyone is ecstatic with his progress so far,” says Lauren Porter, who is the patient’s mother. “We hope having this surgery will give him a lot more freedom to do the things he loves in his life, and we hope that by sharing our story we are helping to make procedures like this more available to kids who need them in the future.”
Artificial heart valves are the standard of care for a failing valve in a child born with congenital heart disease. But Dr. d’Udekem says they are exceptionally difficult in children. First, a traditional artificial tissue valve lasts only about a decade, so children like Preston who have their first valve inserted before age 2 will inevitably face at least two to three additional open-heart surgeries before age 40. Additionally, just like adults, an artificial mechanical heart valve requires the patient to take blood thinners and major precautions against injury for their entire lives. Research has also shown that the placement of an artificial heart valve causes the heart to change shape over time, impacting heart function later in life and leading to a shortened life span.
Replacing this valve with a living transplanted valve will give Preston freedom from a lifetime of blood-thinning medication. Research also shows these live tissue implants should grow along with him, greatly decreasing the likelihood of future open-heart surgeries.
“Everyone is ecstatic with his progress so far,” says Lauren Porter, who is the patient’s mother. “We hope having this surgery will give him a lot more freedom to do the things he loves in his life, and we hope that by sharing our story we are helping to make procedures like this more available to kids who need them in the future.”
Children’s National is the first hospital to remove a child’s previously implanted artificial valve and replace it with a live working valve from a donated heart through a relatively new procedure called a partial heart transplant. The Children’s National partial heart transplant replaced the heart’s mitral valve, which is the valve between the left upper chamber (left atrium) and the left lower chamber (left ventricle) of the heart. In general, partial heart transplants are rare. Prior to this surgery, four U.S. hospitals have used partial heart transplants to replace a failing, living heart valve with a valve from a donor heart, but no organization to date has ever replaced a prosthetic valve with a real one.
“Making this procedure an option for certain children who need a heart valve replacement is critical to having patients live their best lives and to providing hope to their family as they grow into adolescence and adulthood,” says Wayne J. Franklin, MD, senior vice president of the Children’s National Heart Center and a congenital cardiology specialist. “I am proud of our team that conducts such important research to innovate better clinical solutions for all of our patients with congenital heart disease.”
Live tissue partial heart transplants also offer an additional benefit. Donated hearts that do not qualify for use in a total heart transplant may have healthy components, like valves, that can be used for patients who don’t require total replacement. Candidates and potential donors are listed in a registry and matched according to biological factors including blood type, similar to the process for determining full heart transplant candidates.
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-04-22 10:31:052026-04-13 10:39:42REI Week 2025 empowers the future in pediatric research and innovation
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/Article_Image_400x300_Linguraru.jpg12501667Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-04-14 11:05:362026-04-10 15:37:16Podcast: Future ready: AI’s role in revolutionizing pediatric care
Dr. Franklin’s talk offered his observations of how the administrative backbone behind clinical care supports a thriving center for infants and children with congenital heart disease and their families.
Wayne Franklin, MD, FACC, senior vice president of Children’s National Heart Center, joined a panel discussion at Cardiology 2025: The 28th Annual Update on Pediatric and Congenital Heart Disease. The panel, Healthcare Administration in Pediatric and Congenital Cardiovascular Disease: Sharing Challenges and Creating Solutions, sought to identify the traits that successful U.S. healthcare programs, and especially pediatric cardiovascular programs, have in common.
Dr. Franklin’s talk, “Structuring Administration for Pediatric & Congenital Cardiovascular Care,” offered his observations of how the administrative backbone behind clinical care supports a thriving center for infants and children with congenital heart disease and their families.
The big picture
Dr. Franklin noted that the best programs are finding successful combinations of the right ingredients to make the “secret sauce” — focus on high quality care being delivered in ways that are financially sustainable. More than ever, this is hard to accomplish.
Today’s pediatric programs are often organized in an academic model where clinicians are employed by a university or medical school, typically within a Department of Pediatrics, with pediatric subspecialties all falling together under that department. While the academic model has been successful up to this point, there may be valuable lessons to learn and opportunities for further success by looking at outcomes from other models in the broader adult healthcare sector.
Key takeaways
Dr. Franklin offered several examples of key models for pediatric heart centers to consider. They include:
A multi-disciplinary, “service-line centered” structure: All doctors, nurses, advanced practice providers and support staff aligned together under a “center” or “institute” model, similar to the Cleveland Clinic’s Institutes of Excellence.
A blended, “privademic” structure for clinicians, where they are direct employees of a hospital, but not of a larger university or healthcare system.
Clinician leadership and engagement in business administration structure and function, to make sure that patients remain front and center in business decisions.
Dedicated quality and safety teams that are driven by data and outcomes, foster frequent and early communication and ensure care providers actively engage with these efforts.
A model that supports innovations in care and investments in research to continue advancing best practices for patients and families.
A system for education and training to make sure the next generation can effectively carry on the established culture of excellence.
What matters most
No matter the structure, the most important and common theme among successful health systems, hospitals and even specific heart programs, is steadfast, organization-wide dedication to decision making driven by what is best for patients. This approach should drive a focus on early detection and/or prevention, and lead to positive outcomes, which ultimately brings financial sustainability.
A pacemaker modified in a novel way to work better for the smallest children, including newborns, is safe and effective to stabilize heart rhythms for at least two years, according to a study published in Circulation: Arrhythmia and Electrophysiology, a journal of the American Heart Association.
The study includes the findings from 29 infants who received the novel pediatric pacemaker, which is no bigger than a AAA battery, at multiple institutions in the United States. A majority of them (79%) were born premature, weighing less than five pounds (2.3 kg).
The devices remain stable, with effective pacing, normal electrical parameters and battery longevity aligned with projections for up to two years. This design and application provides a viable alternative to standard-size generators and addresses a vital unmet need for these small patients. In fact, though the study includes data from the first 29 cases, the number of children who have received these devices across the United States today has doubled to nearly 60.
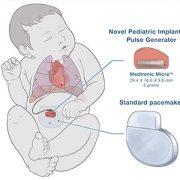
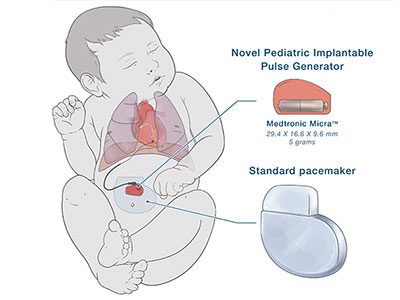
The specially modified pediatric-sized implantable pacemaker includes a Medtronic Micra sub-assembly that connects to an epicardial lead. While this makes the leadless pacemaker into one that uses leads, the resulting device is significantly smaller than any commercially available pacemaker previously on the market in the U.S.
The novel pediatric implantable pulse generator is about a quarter of the size of a traditional pacemaker.
Why it matters
“The need for an urgent permanent pacemaker in newborns is quite rare, but when needed, it is often an emergency,” said lead author Charles Berul, MD, a cardiologist and electrophysiologist at Children’s National Hospital in a press release from the American Heart Association. “Babies who were very small often cannot get a permanent pacemaker and must undergo multiple temporary pacing wires or other techniques in the hopes of getting them big enough to undergo a standard pacemaker placement.”
Dr. Berul also notes that a smaller pacemaker may also help frail elderly patients and be a better choice for some children and adults.
What’s next: Better delivery
Innovating smaller devices is a good start. However, when a newborn or young child needs any pacemaker or defibrillator, they face open chest surgery. Their arteries and veins are just too small for even the smallest size transvenous pacemaker catheter.
In December of 2024, a team that included experts from Children’s National Hospital traveled to Uganda to continue work on a pilot program applying artificial intelligence (AI) to the diagnosis of rheumatic heart disease (RHD). Ugandan health care providers have been trained and equipped to acquire echocardiograms for their patients but lack expertise in consistently being able to diagnose RHD by detecting leaky heart valves. The team created a tool that uses AI to predict RHD by identifying leaky heart valves on handheld ultrasound devices, then prompts a referral for a full echocardiogram.
The goal is to find ways to help people in Uganda diagnose RHD early, before a patient is in need of surgery, and initiate antibiotics so their heart can return to normal. The team of researchers, including fellow Kelsey Brown, MD, helped to implement additional steps toward this goal in December. According to Dr. Brown, the results were excellent. After four days of seeing patients, over 450 people were screened. The AI tool has an 86% accuracy rating. After returning from Uganda, the research team plans to work on the AI tool and further improve its accuracy rating. Eventually, the vision is that this tool can roll out on a larger scale for more places around the world to access it.
Craig Sable, MD, Marius Linguraru, DPhil, MA, MSc, and Pooneh Roshanitabrizi, PhD, from our Sheikh Zayed Institute, who developed the AI algorithms, worked in partnership with the Rheumatic Heart Disease Research Collaborative (RRCU) in Uganda. This trip was also made possible thanks to a grant funded through the Children’s National Global Health Initiative. Special thank you to our AI partner, US2.AI, who made the deployment of the AI models onto a tablet that provided real-time results, possible.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/RHD-AI-Uganda-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-02-26 10:43:202025-05-06 13:49:45Children’s National brings AI into the RHD early diagnosis equation
Drs. d’Udekem and Franklin at the 28th Annual Update on Pediatric and Congenital Cardiovascular Disease.
The 28th Annual Update on Pediatric and Congenital Cardiovascular Disease took place from February 19-23, 2025, at the Disney Yacht & Beach Club Resort in Lake Buena Vista, Florida. The conference, themed “Hope, Heal, Learn,” emphasized critical advancements and practices in pediatric cardiovascular care. Children’s National Heart Center experts presented their latest research findings, insights and innovations during the conference.
Speaker: Does the Nature and Size of the Fontan Pathway Make a Difference?
Speaker: 3rdAnnual Thomas L. Spray Surgery Lecture
Awards and recognitions
3rd Annual Thomas L. Spray Surgery Lecture in Pediatric and Congenital Cardiovascular Surgery Selected Speaker: And We Thought That the Fontan Was the Last Operation, Yves d’Udekem, MD, PhD
Top 8 Nursing Abstracts: Early Outcomes of Lost to Follow Up Outreach in Pediatric Congenital Heart Disease Survivors, Arielle Scarpati, NP
Poster and abstract presentations
An Unusual Case of Partial Anomalous Pulmonary Venous Connection with Dual Connection to the Superior Vena Cava and Left Atrium, David Finkelstein, MD, MS
Early Outcomes of Lost to Follow Up Outreach in Pediatric Congenital Heart Disease Survivors, Arielle Scarpati, NP
Pseudoaneurysm of Mitral-Aortic Intervalvular Fibrosa with Left Ventricular Dilation of Arrhythmias, David Finkelstein, MD
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/CHOP-conference-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-02-25 13:01:172026-01-05 13:37:50Heart Center experts contribute to Annual Update on Pediatric and Congenital Cardiovascular Disease
Children who had heart surgery and come from less advantaged neighborhoods in the Washington, D.C., region are much more likely to die in the long term than those from neighborhoods with more wealth and opportunity.
Children who had heart surgery and come from less advantaged neighborhoods in the Washington, D.C., region are much more likely to die in the long term than those from neighborhoods with more wealth and opportunity. The finding was part of a presentation, Socioeconomic Disadvantage Is Associated with Higher Long-Term Mortality After Cardiac Surgery, presented by Jennifer Klein, MD, MPH, cardiologist at Children’s National Hospital, during the Society of Thoracic Surgeons (STS) Annual Meeting in Los Angeles.
What is it?
Clinical and demographic data were collected for 2,546 people who underwent corrective surgery for congenital heart disease over a 15-year period (2007-2022) in a single-center retrospective analysis. Using the Child Opportunity Index (COI), an index that uses environmental/health, educational, and socioeconomic domains to assess patients’ neighborhoods, the two lowest COI quintile neighborhoods were designated as “disadvantaged” while the two highest COI quintile neighborhoods were designated as “advantaged.” Multivariable mixed model analyses were conducted to understand the factors associated with overall mortality.
The research showed that patients from disadvantaged neighborhoods suffered in a great proportion both overall mortality [n=168 (13.6%) vs 66 (8.4%), p< 0.001] and major complications [n=168 (13.6%) vs 81 (10.3%), p< 0.001]. The positive association between neighborhood disadvantage and long-term mortality was maintained in stepwise logistic regression multivariable analysis after controlling for differences between surgical complexity and other clinical risk factors.
What it means
“Previous research has shown disparities like this,” says Dr. Klein. “What’s significant here is that the disparity for children from disadvantaged neighborhoods grows over time. That means corrective interventions won’t be implemented in the operating room or within the first 30 days after surgery. They need to happen in a cardiologist’s office, in the schools, and in the community long after a child goes home from the hospital.”
The findings from this particular study are also noteworthy as they are the first to include significantly greater numbers of patients who are more likely to experience this risk (48.5% of the study group). Previous research has sought to look at this research question but analysis may have been skewed by an over-representation of socioeconomically advantaged patients.
What’s next
Differences in mortality risk continue to grow greater as more time passes, the authors note, indicating that the disparity is not a product of surgical technique or disparities in care delivery at the time of surgery.
Instead, their outcomes are being influenced by factors outside the operating room. This opens a new avenue of research focused on identifying the “why.”
“What happens after they go home?” Klein asks. “Can they access medications? Do they come back for follow-up appointments? Can they afford food?”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/cardiac-surgery-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-30 11:43:322026-03-02 09:20:52Socioeconomic disadvantage associated with higher long-term mortality after heart surgery
Denver D. Brown, MD, nephrologist at Children’s National Hospital, presented at Kidney Week 2024 on the connection between metabolic acidosis and cardiovascular disease risk in children with chronic kidney disease (CKD).
Denver D. Brown, MD, nephrologist at Children’s National Hospital, presented at Kidney Week 2024 on the connection between metabolic acidosis and cardiovascular disease risk in children with chronic kidney disease (CKD). This research aimed to investigate whether untreated metabolic acidosis could potentially contribute to cardiovascular outcomes in children with CKD, a group at high risk for cardiovascular disease and death from cardiovascular complications. Dr. Brown explains her motivation, findings and future directions for this critical research.
Q: Why did you choose to research this topic?
A: My interest in this area stems from my research interest in pediatric CKD outcomes, with a specific focus on the consequences of metabolic acidosis as well as my larger passion which is to improve the quality and longevity of life for children with CKD. There are several adult focused studies investigating theorized links between untreated metabolic acidosis and poor outcomes such as CKD progression, worse bone health/growth and higher cardiovascular risk. However, in the pediatric CKD population, the consequences of chronic metabolic acidosis remain largely unexplored but is of importance since data shows that nearly one third of children with metabolic acidosis are not receiving treatment to correct their acidosis.
Cardiovascular disease is the number one cause of death in children with CKD. Even though overt cardiovascular disease often does not manifest until adulthood, we do see risk factors emerging during childhood such as high blood pressure and abnormal cholesterol levels. So, if metabolic acidosis contributes to cardiovascular disease risk, it’s crucial to identify and treat it — especially since metabolic acidosis is very treatable
This research was in collaboration with the Chronic Kidney Disease in Children (CKiD) study, which is the largest cohort study of pediatric CKD across North America. It provided robust data on laboratory values, blood pressure, cardiovascular measurements and echocardiograms which allowed me to look deeper into the potential cardiovascular implications of metabolic acidosis.
Q: Where do you see this research going?
A: My ultimate goal is to conduct clinical trials focused on the pediatric CKD population. Children are not well represented in CKD trials as pediatric CKD is relatively rare, making recruitment for studies challenging. However, we can’t keep applying adult data to children because the causes and manifestations of CKD in kids are different.
It is my hope that this research serves as evidence that can be used for a pediatric clinical trial that investigates the benefits of alkali therapy, the treatment for metabolic acidosis. I envision studying how alkali therapy impacts not only cardiovascular outcomes but also growth and other important health domains. The data gathered from my study could ultimately be used in a multi-site trial, aiming to test alkali therapy on a broader scale across various pediatric CKD centers.
Q: Is any work being done between nephrologists and cardiologists to address this issue?
A: This specific study was more exploratory. In adults, the data on the link between metabolic acidosis and cardiovascular disease is mixed. Some studies suggest a connection, while others find no such effect when treating metabolic acidosis. My current work is focused on gathering data to determine if there’s a potential link in the pediatric population and whether it should be examined further in a future trial.
I haven’t collaborated directly with cardiologists on this research. However, this could lead to collaboration with cardiologists down the line.
Q: How is Children’s National Hospital leading the way in this research?
A: Although my research data wasn’t exclusively from Children’s National, the hospital played a pivotal role in the CKiD study, both as an enrollment site and through the involvement of Marva Moxey-Mims, M.D., chief of Nephrology at Children’s National, who played a key role in the CKiD study design and initiation.
Children’s National actively participates in, and encourages, novel and innovative research studies. Being at an institution that prioritizes and contributes to research that advances the health of children has been instrumental in my research career.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/10/Denver-Brown.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-29 09:45:292025-01-29 09:47:25The link between metabolic acidosis and cardiovascular disease in children with CKD
The Children’s National Heart Center is leading the way to find new and better treatments for cardiac problems as early as possible, during pregnancy and just after birth.
These critical stages are vital for a child’s lifelong heart health. “The innovations we are pursuing have the potential to transform the landscape of cardiac treatment,” says Wayne Franklin, M.D., F.A.C.C., Heart Center senior vice president.
“By focusing on the earliest stages of life, we can significantly alter the trajectory of children’s heart health, creating a lifetime of possibilities.”
Mending a Broken Heart
Abby with her sister and parents.
Abby, who just turned 1, is a smiley baby who loves to play peek-a-boo with her sister, Ruby. “We marvel that she is perfectly healthy,” says her father, Dan. He and wife Kelsey love to linger over ordinary moments. Her given name, Abigail, means “a father’s joy.”
When Kelsey was 18 weeks pregnant, she and Dan learned their baby had signs of heart injury, which led to a dangerous rhythm problem called “complete heart block.” The previous year, their infant son died from the same condition, which was discovered too late. The family prepared for another loss. But early detection of the problem and advanced care that started in the womb made all the difference for Abby. Children’s National prenatal cardiology experts began monitoring Abby’s development from the earliest possible moment and were able to intervene before devastating injury occurred.
Before Abby’s diagnosis, in light of the previous pregnancy, Kelsey enrolled in a clinical trial. The research sought a better way to identify and treat the heart condition Abby was at risk for. Anita Krishnan, M.D., a pediatric cardiologist and clinician scientist, met the family during their initial visit and arranged a monitoring plan that included frequent visits to make sure Abby’s heart was working normally. Soon after Kelsey’s first visit, doctors noted a problem.
Mary Donofrio, M.D., F.A.A.P., F.A.C.C., F.A.S.E., a leading pediatric and fetal cardiologist and The Van Metre Companies Professor of Fetal Cardiology, led the team that initiated lifesaving in utero therapy, followed Abby’s progress in the womb and planned for her arrival. The goal was to extend the pregnancy for as long as possible so she would survive birth and the heart surgery that would follow.
Abby’s prognosis improved as weeks passed. As a newborn, she would be a candidate for an infant pacemaker the size of a penny. It would help regulate her heartbeat and enable her to live a “normal” life.
Pericardial port for pediatric pacemaker delivery, developed by Dr. Charles Berul and team.
Kelsey and Dan met with Charles Berul, M.D., emeritus chief of Cardiology and The Van Metre Companies Professor of Cardiology, and his team. There was uncertainty about whether Abby’s heart was too damaged for the pacemaker to work, but Dr. Berul, who has spent decades refining designs for this type of device, expressed confidence. Abby would be the world’s 27th infant, and the fifth at Children’s National, to have one implanted.
“To have him say, ‘We’ve developed this device, we know what we’re doing, all of the other babies who have had this are doing well and we’ll be right here in the room with you,’ was pretty incredible,” Dan says.
Kelsey’s monitoring in the clinical trial and the innovative therapy that started before birth likely helped Abby survive until she was born at 32 weeks at MedStar Washington Hospital Center. Dr. Donofrio and the Children’s National care team were in the delivery room and rushed Abby to our Cardiac Intensive Care Unit. Dr. Donofrio arranged for mom and daughter to pass in the hall on the way. “I heard her cry and felt relief for the first time,” Kelsey says.
Abby’s pacemaker enabled her heart to beat properly on its own. She soon moved to our Neonatal Intensive Care Unit. In two months, she went home with her family. Kelsey and Dan monitor her pacemaker with a handheld device that sends reports to her team at the hospital.
“We’re lucky to have doctors nearby who are at the forefront of this lifesaving research. Children’s National took care of us with a great deal of humanity. Now we can focus on being a family,” says Dan.
In 2024, Children’s National Hospital continued to make remarkable strides across diverse areas of pediatric medicine, from groundbreaking technological innovations to critical health advocacy. The following compilation showcases ten significant stories that demonstrate the breadth and depth of the hospital’s impact, as featured in major national news outlets including NBC Nightly News, CNN, The Washington Post, The New York Times, NPR, The Today Show, Healio, and POLITICO. Delve into our 2024 news highlights for more.
Charles Berul, M.D., and a patient family talk about the pill-sized pacemaker that saved the life of Abby, an infant born with deadly heart defects. (NBC Nightly News)
Sivabalaji Kaliamurthy, M.D., addiction psychiatrist and director of the Addictions Program, spoke to CNN about the impact of drug addiction on teen health and the lack of resources available to treat opioid use disorder. (CNN)
Susma Vaidya, M.D., M.P.H., associate medical director of the IDEAL Clinic, shared her concerns about childhood obesity treatment recommendations issued today by a leading panel of independent U.S. health experts. (The Washington Post)
Shideh Majidi, M.D., M.S.C.S., and Emily Frymark, clinical dietitian, spoke about how the food pharmacy, created in partnership with the Capital Area Food Bank, benefits patients with diabetes and other chronic conditions. (The Washington Post)
Kendric Cromer, a 12-year-old boy being treated at Children’s National Hospital, became the first person in the world with sickle cell disease to begin a commercially approved gene therapy that may cure the condition. “This is a big effort,” says David Jacobsohn, M.D., ScM, M.B.A. (The New York Times)
Mikael Petrosyan, M.D., associate chief of General and Thoracic Surgery, discusses the stress medical staff face when treating young victims of gun violence. (NPR)
Landon, an 11-year-old patient, rang the bell at Children’s National Hospital with family, friends, doctors and nurses cheering after finishing his final round of chemotherapy. (The Today Show)
Monika Goyal, M.D., M.S.C.E., pediatric emergency medicine specialist and co-director of the Center for Translational Research, emphasized the need for awareness in addressing period poverty in teenagers and young adults. (Healio)
Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer, participates in a panel discussion covering AI data collection, associated risks, reliance and other topics related to artificial intelligence. (POLITICO)
Children’s National patient Kendric Cromer, 12, became one of the first children ever to be treated with a newly approved gene therapy that will free him from the sickle cell disease that has stolen his childhood. (The New York Times)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/12/2024-News-Logo-Collage-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-12-26 11:34:102024-12-26 11:49:26Children’s National in the News: 2024


 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.