Children’s National Hospital at American Heart Association Scientific Sessions 2024
![]() Experts from Children’s National Heart Center presented and shared their latest research findings at this year’s American Heart Association (AHA) Scientific Sessions, held in Chicago, Illinois, in mid-November.
Experts from Children’s National Heart Center presented and shared their latest research findings at this year’s American Heart Association (AHA) Scientific Sessions, held in Chicago, Illinois, in mid-November.
The annual AHA Scientific Sessions are attended by scientists, clinicians, researchers and other health care professionals from around the globe who have an interest in cardiovascular disease. Children’s National Hospital experts highlighted work focused on caring for the full spectrum of people who live with congenital heart disease — from tiny neonates through adulthood.
Presentations
- Transvenous cardiac re-synchronization: When is it effective in CHD? Charles Berul, M.D.
- Leveling the Playing Field: Creating Equity within Pediatric Cardiology Leadership and Salary, Wayne Franklin, M.D.
- Panel moderator: Annette Ansong, M.D.
- Debate: Patients with small coronary artery aneurysms SHOULD be discharged – US experience, Ashraf Harahsheh, M.D.
- Science of Engagement: Inclusion of Adults with Congenital Heart Disease Living with Neurodevelopmental Disability in PCOR, Anitha John, M.D., Ph.D.
- 100 Years of AHA Leading Global Health, Craig Sable, M.D.
- Best Oral Abstract: Safety of Discontinuing Secondary Antibiotic Prophylaxis After Echocardiographic Normalization in Early Rheumatic Heart Disease, GOAL-Post Study, Craig Sable, M.D., co-author
- Su2032│CMR can discriminate need for biopsy and rejection therapy in children post heart transplant, Ravi Vamsee Vegulla, M.D.
Posters and poster presentations
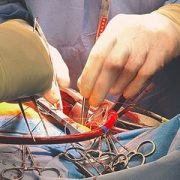
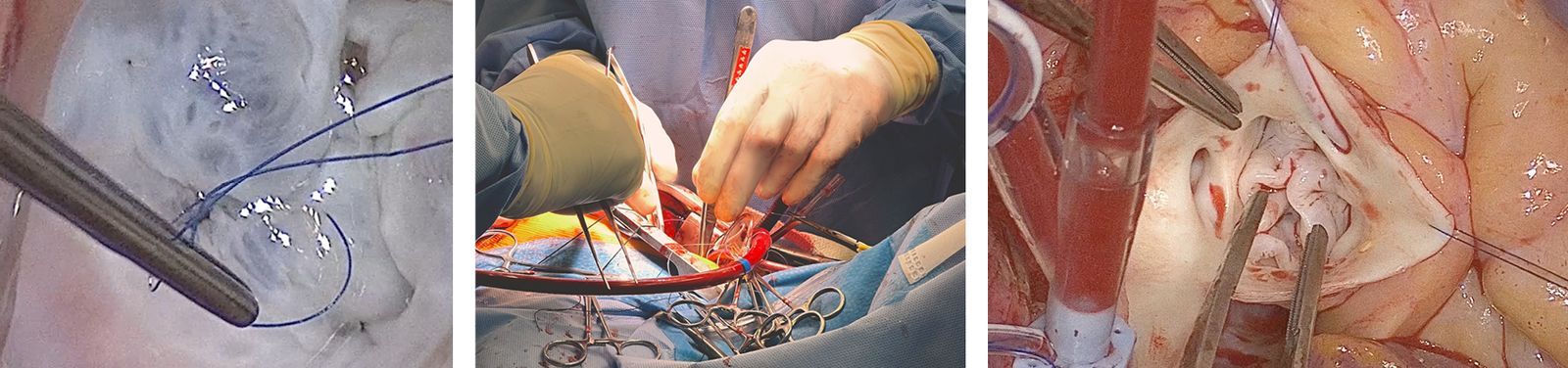
- Minimally-Invasive Intrapericardial Injections under Direct Visualization via Thoracic Cavity Access in Infant and Pediatric-sized Pre-clinical Model, Charles Berul, M.D., Ryan O’Hara, Ph.D.
- Early total cfDNA, but not donor fraction, predicts late events after heart transplantation, Shriprasad Deshpande, M.D.
- Impact of Angiotensin Receptor Neprilysin Inhibitor on Chronic Heart Failure with Reduced Ejection, Shriprasad Deshpande, M.D.
- Fraction in Adult Congenital Heart Disease Patients: A Systematic Review and Meta-analysis, Shriprasad Deshpande, M.D.
- Trough Level Prediction of Major Adverse Transplant Events: A Report from the TEAMMATE Trial, Shriprasad Deshpande, M.D.
- Thrombocytosis is Prevalent and Associated with Greater Inflammation and Coronary Artery Involvement in Both Kawasaki Disease and Multisystem Inflammatory Syndrome in Children Associated with COVID-19, Ashraf Harahsheh, M.D.
- Mesenchymal Stromal Cell Delivery through Cardiopulmonary Bypass in Pediatric Cardiac Surgery – MeDCaP Phase I Trial, Nobuyuki Ishibashi, M.D., Shriprasad Deshpande, M.D., et. al.
- Social Determinants of Health: Impact on Mortality and Care Status for Adults with CHD, Jamie Jackson, Ph.D.; Anitha John, M.D., Ph.D., co-author
- Loss to Follow-Up Among Adults with Congenital Heart Defects: A Report from Congenital Heart Disease Project to Understand Lifelong Survivor Experience (CHD PULSE), Anitha John, M.D., Ph.D., co-author
- The Burden of Adult Congenital Heart Disease in the United States, Vasupradha Suresh Kumar, M.D.
- Determining the Physiologic Effect of the Cavopulmonary Connection on Caval Flows Using 4D Flow MRI , Vasupradha Suresh Kumar, M.D.
- Shape Variations in Right Ventricular 3D Geometry are associated with adverse outcomes in Hypoplastic Left Heart Syndrome Patients: A Fontan Outcomes Registry using CMR Examination (FORCE) Study, Yue-Hin Loke, M.D.
- Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases as Biomarkers in Duchenne Muscular Dystrophy Cardiomyopathy, Christopher Spurney, M.D., co-author
- Duchenne Muscular Dystrophy Boys Have Diastolic Dysfunction Based on Cardiac Magnetic Resonance, Christopher Spurney, M.D., co-author
Read more about these presentations and posters on the AHA’s meeting website: Programming – Scientific Sessions 2024.

 2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.
2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.







 Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.
Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.



 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the