Using Fitbit data from the the largest long-term study of brain development and child health in the United States, researchers employed machine learning to test whether physiological markers could accurately predict ADHD diagnoses.
A new study published in Frontiers in Child and Adolescent Psychiatry reveals that common wearable devices like Fitbits may hold the key to improving how we identify Attention-Deficit/Hyperactivity Disorder (ADHD) in adolescents. By analyzing patterns in heart rate, activity levels and energy expenditure, researchers were able to predict ADHD diagnoses with striking accuracy, offering a glimpse into a future where objective, real-time data supports earlier and more personalized mental healthcare.
A fresh approach to a common challenge
ADHD affects approximately 1 in 10 children and adolescents in the United States. It is typically diagnosed based on parent and teacher reports, clinical interviews and behavioral observations. While effective, these methods rely heavily on subjective interpretation and can sometimes miss important nuances in how symptoms appear over time. This study, led by Muhammad Mahbubur Rahman, PhD, and colleagues at Children’s National, sought to determine whether wearable health data could help fill that gap.
Turning Fitbit metrics into meaningful insights
The study used data from 450 adolescents who were part of the larger Adolescent Brain Cognitive Development (ABCD) study, the largest long-term study of brain development and child health in the United States. Each participant wore a Fitbit, which captured three key activity and physiological measures:
Resting Heart Rate (RHR) – the number of heart beats per minute while the body is at rest
Sedentary Time – time spent with little or no physical activity
Energy Expenditure – estimated calories burned through physical activity
When the researchers compared these measures between teens with and without ADHD, they found statistically significant differences. Teens with ADHD had consistently higher resting heart rates and showed distinctive patterns in both their movement and stillness.
To go further, the team applied a machine learning model to test whether these physiological markers could accurately predict ADHD diagnoses. The model performed extremely well with 89% accuracy, 88% precision, 90% recall and a 0.95 area under the curve (AUC). These results suggest that the combination of passive, continuous data and predictive modeling could serve as a valuable screening tool, particularly in settings where full clinical evaluations are difficult to access.
A path toward more accessible mental healthcare
The implications are big. If validated in larger and more diverse populations, wearable-derived data could offer a low-cost, low-burden way to flag teens who might benefit from further ADHD evaluation. This could lead to earlier support, fewer misdiagnoses and more tailored treatment strategies.
Importantly, this approach isn’t about replacing clinicians, it’s about giving them better tools. Real-world, real-time data from wearables could act as an additional layer of insight that supports more precise, individualized care. As wearable technology becomes more embedded in daily life, its role in healthcare, especially adolescent mental health, is poised to grow.
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-04-22 10:31:052025-06-10 12:20:52REI Week 2025 empowers the future in pediatric research and innovation
Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.
The awardees, selected from a highly competitive field of ten finalists, are:
Sibel Health, Chicago – Hospital-to-home monitoring for pediatric heart conditions
The competition is presented by the Alliance for Pediatric Device Innovation (APDI), a nonprofit consortium led by Children’s National Hospital and funded through the Food and Drug Administration (FDA), and Additional Ventures, a nonprofit focused on accelerating research progress and improving clinical care for individuals born with single ventricle heart defects. Along with grant funding, awardees gain access to support services and technical expertise provided by APDI and Additional Ventures in areas that include engineering, regulatory, reimbursement, clinical trials study design and data science services.
According to the Centers for Disease Control and Prevention, about 40,000 children are born annually with a congenital heart defect. Children with heart conditions need medical devices tailored to their specific physiological needs. There is a significant unmet need for pediatric devices designed to monitor and treat young patients effectively in cardiology, interventional cardiology, cardiac surgery and electrophysiology. This competitive grant program is designed to identify and support the development and commercialization of devices addressing these needs.
“Congratulations to our awardees, whose innovative technologies show great promise in advancing care for pediatric heart patients,” said Kolaleh Eskandanian, Ph.D., M.B.A., vice president and chief innovation officer at Children’s National and APDI program director and principal investigator. “We are thrilled to welcome this new cohort into our pediatric device accelerator, where they will have the opportunity to collaborate with clinician-scientists at Children’s National and connect to Additional Ventures’ network. Along with these collaborations, the awardees will benefit from a full range of APDI wraparound services designed to support the development of devices specifically for pediatric patients, helping them navigate the complex path to market.”
The competition was held in conjunction with the 12th Annual Symposium on Pediatric Device Innovation, presented by Children’s National and co-located with The MedTech Conference powered by AdvaMed. Focused on transforming pediatric care with exclusive innovations for children, this year’s symposium featured panel discussions and keynote presentations with leading experts in pediatrics and medical technology to exchange information and ideas on critical issues in pediatric device development and pediatric healthcare innovation gaps.
“Additional Ventures is thrilled to support this new class of innovators whose products will make a profound impact in the management and care of pediatric heart patients,” said Additional Ventures CEO Kristie Keller, Ph.D. “We welcome them to our growing community of inventors, researchers and clinicians, and we look forward to working together with our awarded teams and ADPI to bring these products to market. We hope that this competition both inspires and activates the community and brings much-needed new entrants and new ideas to pediatric-first device development.”
APDI is one of five nonprofit consortia in the FDA’s Pediatric Device Consortia grant program. It receives funding to provide a platform of services, expertise and grants that support pediatric innovators in bringing medical devices to the market that specifically address the unmet needs of children. Led by Children’s National, APDI partners include Johns Hopkins University, CIMIT at Mass General Brigham, Tufts Medical Center, MedStar Health Research Institute, MedTech Color and OrthoPediatrics Corp.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/10/CNH-Cardio-Pitch-Winners-2024-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-10-17 10:29:132025-03-10 14:03:04Winners announced in pediatric medical device competition focused on cardiology
Oracle Health and Children’s National Hospital, announced the winners of the third annual Bear Institute’s Pediatric Accelerator Challenge for Kids (Bear PACK), a start-up competition aimed at fostering digital health innovation for children. The winners — Bend Health Inc., Kismet Health, RareCareNow, and Thynk Inc. — were recognized across four innovation tracks for their efforts to improve child health outcomes, enhance the care experience for patients, family, and clinicians and reduce the cost of care for patients and health systems.
With more than 250 standalone pediatric hospitals in the U.S. today, there is a significant opportunity for technology startups focused on pediatric care to overcome unique funding and go-to-market challenges to more successfully build and sustain their businesses and have a positive impact on the lives of thousands of children and their families.
“Bear PACK targets the entire pediatric healthcare community to help close the gap in innovative solutions dedicated to helping children, said Jessica Herstek, M.D., chief medical information officer, Children’s National Hospital. “Together, Oracle Health and Children’s National Hospital are helping startups accelerate innovation and technology adoption by showcasing new products and connecting startups with pediatric healthcare providers and administrators.”
“With less than one percent of global digital health funding being allocated for children’s health1, the Bear PACK challenge has never felt more important or needed,” said Nasim Afsar, M.D., MBA, MHM, senior vice president and chief health officer, Oracle Health. “Working with Children’s National Hospital, we’re continuing to make meaningful progress on bringing more digital health solutions for kids to market, helping to improve pediatric patient experience and health outcomes globally.”
The 2023 winners in each category are:
Early-State Innovation: RareCareNow
Using a telehealth platform, RareCareNow is helping patients who have been diagnosed and are seeking treatment for rare and genomic diseases in the U.S. With molecular diagnostics integrated earlier in the care process, patients can more quickly identify and connect with a specialist using RareCareNow’s network of physicians providing care specific to their needs. Patients will not only receive genetic counseling and treatment plans but will have a long-term provider for ongoing care coordination and symptom management.
“Our goal is to reimagine how genomic medicine is practiced by bringing cutting edge molecular diagnostics into the care process earlier and then providing ongoing care and coordination for all patients so they can benefit from their genomic results. While we’re improving access to care for patients with genomic and rare diseases, we also aim to ease the uncertainty of the diagnosis and the diagnostic odyssey. By embracing telehealth and technology, we will enable patients and families to be more proactively involved in their own care.” — Alexander Katz, chief medical officer and co-founder, RareCareNow
Designed by and for providers, Kismet Health’s pediatric virtual care platform offers a digital playspace that allows clinicians to communicate with patients through their language of play, increasing overall patient engagement and effectiveness. Kismet’s collaborative care technology allows providers to bring healthcare access to families where and when they need it most, allowing for longitudinal care throughout the entire year and more equitable outcomes.
“It’s an honor to be selected for this innovative program with like-minded individuals who are also passionate about revolutionizing the future of pediatric healthcare. Kismet has launched with digital health companies and smaller clinics, with the goal now to integrate with EHRs like Oracle Health’s to expand to children’s hospitals, health systems, and government programs — ultimately meeting families where they are and closing the gap in care access.” — Christie Sander, co-founder, president and COO, Kismet Health
Thynk Inc. developed an immersive game designed to help children improve cognitive skills and overall mental wellness in a safe and fun environment. Youth play an adventure game on a mobile device while wearing a headset that uses proprietary EEG technology that reads brainwaves to determine their level of focused attention. This measured focus level also controls the speed and success of the in-game character as it completes various missions, and the difficulty level adjusts accordingly. With regular use, children can improve 13 cognitive skills including focused attention, impulse management, and develop their self-regulation skills, all of which are important for academic success and personal growth.
“Our product has proven lasting effects in improving focus and attention for children who may be struggling with such skills. The outcomes of eight successful clinical studies with more than 300 users of our product have shown improvements in behavior, test scores, homework completion, and math and reading fluency. In addition to teaming with healthcare organizations, we’re working to also reach underserved populations who may lack access to the tools needed to improve cognitive skills.” — Christopher Tracy, co-founder, board director and chief operating officer, Thynk Inc.
Bend Health designed a virtual mental health platform for kids and their families to increase access, reduce wait times, and decrease costs of pediatric mental healthcare. As the only provider using the Collaborative Care Model in partnership with pediatric primary care, Bend’s data-driven platform allows primary care providers to easily refer and connect patients with virtual therapists. They then receive regular updates on care progress, more closely aligning medical and behavioral care. Offering services such as coaching, therapy, and expedited psychiatric care, Bend integrates virtual video visits, chat messaging, and digital experiences to achieve better outcomes through measurement-based care. Collaborating with leading insurers, employers, health systems, and providing self-pay options, Bend Health ensures widespread accessibility to its services.
“At Bend Health, pediatricians receive regular patient progress updates, empowering them to make informed care decisions based on timely mental health measures. Bend’s collaborative care teams enable practitioners to accurately diagnose children and provide a holistic approach that consistently achieves clinically significant results for both kids and their families. Our six peer-reviewed studies demonstrate these positive outcomes, with 80% of kids showing improvement in 60-90 days, and 4 out of 5 caregivers reporting reduced stress within a month of joining Bend.” — Dr. Monika Roots, President and Co-Founder, Bend Health
1Children’s digital health innovation received less than 1% ($167 million) of global digital health funding ($22 billion) in 2020, according to StartUp Health’s annual report on digital health funding.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/01/Bear-Institute-PACK-logo-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-02-08 10:56:372024-12-30 12:52:28Winners of the third annual Bear Institute PACK Event
In December 2022, the Bear Institute, along with Children’s National Hospital and Oracle Health, hosted the second annual Bear Institute PACK (Pediatric Accelerator Challenge for Kids), a start-up competition aimed to foster pediatric digital health innovation.
Bear Institute PACK is inclusive of the entire pediatric health care community and addresses the large disparity in digital health innovation funding dedicated to children versus the rest of the population. “We have to do more for children, a population that can’t advocate for itself,” says Matt Macvey, M.B.A., MS, executive vice president and chief information officer at Children’s National Hospital. “Bear Institute PACK is an all-hands effort to provide increased support to those start-ups trying to bring new solutions to market for kids.”
Start-ups share their innovations and receive valuable feedback from expert judges while competing for a chance to win an on-site pilot and software development support. The competition features three rounds of judging: an initial review of applications from the Bear Institute PACK team, judging from participating pediatric healthcare providers and administrators and review from an expert panel of judges during finalist start-ups’ live pitches. This year’s start-up participants competed across four innovation tracks in the following areas of development: Early-Stage Innovation, Concept Validation, Early Commercialization and Growth Trajectory.
This 2022 winners, in four innovation tracks, are:
Early-Stage Innovation (“Even the biggest ideas start small”) Winner: PigPug Health Its solution uses neurofeedback, a non-invasive approach to treating brain-related conditions, and artificial intelligence to help children with ADHD and autism become more socialized.
Concept Validation (“Now it’s time to test it”) Winner:Global Continence, Inc.
Its Soluu™, Bedwetting Mitigation Device, helps rapidly and permanently mitigate bedwetting with a neuromodulation process.
Early Commercialization (“Countdown to launch”) Winner:PyrAmes Inc.
Its solution Boppli™ provides continuous, non-invasive blood pressure monitoring and streams data via Bluetooth to a mobile device.
Growth Trajectory (“The investment is growing”) Winner:maro
Its full stack child development kit equips a child’s caretakers (at home, school and clinic) with easy access to tools and data needed to help them navigate tough conversations including mental health, diversity, empathy, and puberty and helps identify mental health at-risk students in schools.
“I was very impressed with this year’s start-up participants and their caliber of talent and passion for what they do. The finalist judges were tasked with selecting one winner in each innovation track, but the work each participant is doing for kids makes them all winners,” says Rebecca Laborde, Ph.D., chief scientist, vice president of Health Innovation and Scientific Advisory, Oracle Health. “Thank you to the entire pediatric healthcare community that comes together to help make this event a success. We believe that by bringing together like-minded individuals with the same goals, we can make a real difference in pediatric healthcare.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/01/Bear-Institute-PACK-logo-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2023-01-19 15:05:492024-11-14 11:49:20Bear Institute Pediatric Accelerator Challenge for Kids winners announced
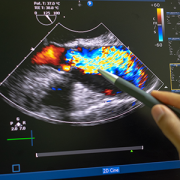
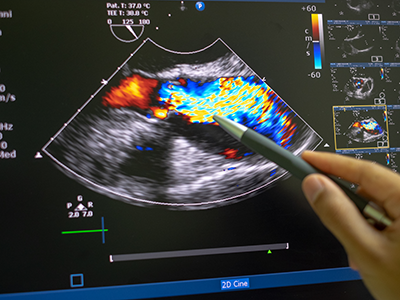
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians.
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians. Even better, this novel model diagnoses this deadly heart condition from echocardiography images of varying quality — including from low-resource settings — a huge challenge that has delayed efforts to automate RHD diagnosis for children in these areas.
Why it matters
Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
Though widely eradicated in nations such as the United States, rheumatic fever remains prevalent in developing countries, including those in sub-Saharan Africa. Recent studies have shown that, if detected soon enough, a regular dose of penicillin may slow the development and damage caused by RHD. But it has to be detected.
The hold-up in the field
Diagnosing RHD requires an ultrasound image of the heart, known as an echocardiogram. However, ultrasound in general is very variable as an imaging modality. It is full of texture and noise, making it one of the most challenging to interpret visually. Specialists undergo significant training to read them correctly. However, in areas where RHD is rampant, people who can successfully read these images are few and far between. Making matters worse, the devices used in these low resource settings have their own levels of varying quality, especially when compared to what is available in a well-resourced hospital elsewhere.
The research team hypothesized that a novel, automated deep learning-based method might detect successfully diagnose RHD, which would allow for more diagnoses in areas where specialists are limited. However, to date, machine learning has struggled the same way the human eye does with noisy ultrasound images.
Children’s National leads the way
Using approaches that led to successful objective digital biometric analysis software for non-invasive screening of genetic disease, researchers at the Sheikh Zayed Institute for Pediatric Surgical Innovation, including medical imaging scientist Pooneh Roshanitabrizi, Ph.D., and Marius Linguraru, D.Phil., M.A., M.Sc., principal investigator, partnered with clinicians from Children’s National Hospital, including Craig Sable, M.D., associate chief of Cardiology and director of Echocardiography, and cardiology fellow Kelsey Brown, M.D., who are heavily involved in efforts to research, improve treatments and ultimately eliminate the deadly impacts of RHD in children. The collaborators also included cardiac surgeons from the Uganda Heart Institute and cardiologists from Cincinnati Children’s Hospital Medical Center.
Dr. Linguraru’s team of AI and imaging scientists spent hours working with cardiologists, including Dr. Sable, to truly understand how they approach and assess RHD from echocardiograms. Building the tool based on that knowledge is why this tool stands apart from other efforts to use machine-learning for this purpose. Orienting the approach to the clinical steps of diagnosis is what led to the very first deep learning algorithm that diagnoses mild RHD with similar success to the specialists themselves. After the platform was built, 2,136 echocardiograms from 591 children treated at the Uganda Heart Institute fed the learning algorithm.
What’s next
The team will continue to collect data points based on clinical imaging data to refine and validate the tool. Ultimately, researchers will look for a way that the algorithm can work directly with ultrasound/echocardiogram machines. For example, the program might be run through an app that sits on top of an ultrasound device and works on the same platform to communicate directly with it, right in the clinic. By putting the two technologies together, care providers on the ground will be able to diagnose mild cases and prescribe prophylactic treatments like penicillin in one visit.
Children’s National Hospital continues in its efforts to educate and advocate about ways to address the unique challenges facing pediatric medical device innovation, such as small market size and a lack of industry investment. In a recent commentary for IEEE Pulse, the publication of the IEEE Engineering in Medicine and Biology Society, Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital and principal investigator of the National Capital Consortium for Pediatric Device Innovation (NCC-PDI), discussed how the FDA and children’s hospitals are stepping in to bridge critical funding gaps and build an accessible infrastructure that safely accelerates the development and commercialization of pediatric medical devices.
“Our goal is to provide direct funding [with] expert advising and support services to innovators of pediatric medical devices,” says Eskandanian.
“Our goal is to provide direct funding [with] expert advising and support services to innovators of pediatric medical devices,” says Eskandanian. “The notion that innovation follows investment, that really gave us the idea of competitions where if we announced a challenge and we could put grant money behind it—and open it to the entire world — then we could attract small businesses and start-up companies that could come forward and start thinking about developing a medical device more specifically for the pediatric population.”
Now in its 8th year, NCC-PDI’s “Make Your Medical Device Pitch for Kids!” competition focuses on identifying and supporting innovators that address specific unmet pediatric needs. This year’s competition focuses on innovations in pediatric devices that treat congenital heart disease (CHD), with an emphasis on electrophysiology (EP) devices such as pacemaker systems, ablation catheters, wearable monitoring devices and related technologies that address arrhythmias in children. While the last decade brought great advances in technologies that improve the care of adult arrhythmias, pediatric patients have been left behind, with only five devices approved for use in children in the same period.
To learn more about the consortium’s efforts to advance pediatric innovation, visit the NCC-PDI website.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/01/newborn-baby.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-04-12 15:37:402025-03-10 11:23:06Creating accessible platforms for innovation is essential to advancing children’s health
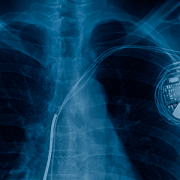
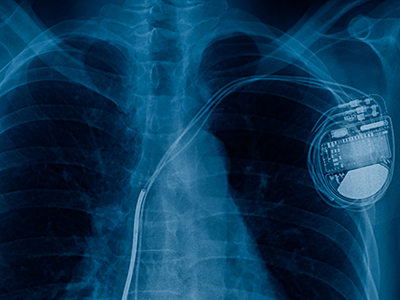
While the last decade brought great advances in technologies that improve the care of adult arrhythmias, pediatric patients have been left behind, with only five devices approved for use in children in the same period.
Congenital heart disease (CHD) affects six out of 1,000 babies born in the U.S. each year and is often complicated by arrhythmias, a condition where the heart beats too rapidly, too slowly or irregularly due to a misfiring of the body’s electrical impulses. While the last decade brought great advances in technologies that improve the care of adult arrhythmias, pediatric patients have been left behind, with only five devices approved for use in children in the same period. As a result, pediatric specialists are often using off-label or improvised devices to treat pediatric arrhythmias, including the smallest newborns.
Recognizing this unmet need, the National Capital Consortium for Pediatric Device Innovation (NCC-PDI), in collaboration with MedTech Innovator, is accepting applications through April 12, 2021, for its annual “Make Your Medical Device Pitch for Kids!” competition. This year’s competition focuses on innovations in pediatric devices that treat CHD, with an emphasis on electrophysiology devices such as pacemaker systems, ablation catheters, wearable monitoring devices and related technologies that address arrhythmias in children.
“NCC-PDI was created, with the support of the Food and Drug Administration (FDA), to seek out and address significant unmet needs in pediatric medical devices,” says Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “We have learned from the experts that pediatric-specific technologies for treating arrhythmias would be a game changer in the care of their patients, so we are focusing our competition and grant awards on this opportunity.”
“We have learned from the experts that pediatric-specific technologies for treating arrhythmias would be a game changer in the care of their patients, so we are focusing our competition and grant awards on this opportunity,” says Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI.
Using a virtual format, semi-finalists chosen from all submissions will make their first pitch on May 12, 2021. Up to 10 finalists selected from this event earn participation in a special pediatric-focused track of the MedTech Innovator accelerator program, the largest medtech accelerator in the world, beginning in June 2021. These innovators then participate in the pediatric competition finals in September 2021 where judges will award up to $150,000 in FDA-sponsored grants to the devices selected as most impactful and commercially viable.
How significant is the need for pediatric devices to address arrhythmias? In a recent survey of members conducted by the Pediatric and Congenital Electrophysiology Society (PACES), the vast majority (96%) said they believe there is a deficiency in devices available to serve the needs of pediatric patients. Conducted with the U.S.FDA, the survey also asked respondents to identify the biggest unmet need, which physicians identified as cardiovascular implantable electronic devices that are smaller, have better battery life and have pediatric-specific algorithms. Specifically, a leadless pacemaker designed for pediatric care was consistently on the most-wanted list.
NCC-PDI is one of five members in the FDA’s Pediatric Device Consortia Grant Program created to support the development and commercialization of medical devices for children, which lags significantly behind the advancement of adult medical devices. NCC-PDI is led by the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland with support from partners MedTech Innovator, BioHealth Innovation and design firm Archimedic.
Eskandanian says that enhancing access to resources for pediatric innovators is also one of the aims of the Children’s National Research & Innovation Campus, a first-of-its-kind focused on pediatric health care innovation, with the first phase currently open on the former Walter Reed Army Medical Center campus in Washington, D.C. With its proximity to federal research institutions and agencies, universities, academic research centers, as well as on-site incubator Johnson and Johnson Innovation – JLABS, the campus provides a rich ecosystem of public and private partners which, like the NCC-PDI network, will help bolster pediatric innovation and commercialization.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/03/x-ray-showing-pacemaker.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-03-25 10:08:432025-03-10 11:13:06Medical device pitch competition focuses on pediatric electrophysiology devices for CHD
The 8th Annual Pediatric Device Innovation Symposium presented by @ChildrensNatl in conjunction with @Devices4kids took place Sept. 28-30.
The 8th Annual Pediatric Device Innovation Symposium presented by Children’s National Hospital in conjunction with the National Capital Consortium for Pediatric Medical Devices (NCC-PDI) kicked off on Monday, Sept. 28, 2020 with a panel featuring three fellow members of the FDA-funded Pediatric Device Consortia (PDC) Grants Program discussing real-world evidence and the vital role that innovation and technology play in advancing healthcare for the pediatric population.
As described by the FDA, real-world evidence (RWE) is the clinical evidence regarding the usage and potential benefits or risks of a medical product, derived from the analysis of patient data. RWE can be generated by different study designs or analyses, including but not limited to, randomized trials, including large simple trials, pragmatic trials and observational studies (prospective and/or retrospective).
The symposium panel, “Pediatric Device Consortia Update on the Use of Real-World Evidence (RWE) for Pediatric Device Innovation” examined real-world evidence (RWE) demonstration projects from Southwest Pediatric Device Consortium, UCSF-Stanford Pediatric Device Consortium and the West Coast Consortium for Technology and Innovation in Pediatrics (CTIP). The panel was moderated by Juan Espinoza, M.D., FAAP, director of CTIP.
“Real-world evidence projects are critical to the advancement of pediatric medical device innovation,” said Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital, and principal investigator for NCC-PDI. “Bringing together our colleagues in pediatric healthcare through the symposium helps us together identify solutions that will bring medical device innovations to the market faster to benefit the children and families we all serve.”
Here are some of the key discussion points made by panelists regarding current RWE demonstration projects:
Emerging medical and consumer technologies are enabling the diabetes community to take great strides toward truly personalized, real-time, data-driven management.
“Connected” technologies such as smartphone apps, wearable devices and sensors create an ecosystem of data driven-tools that can link patients and care teams for precision management of conditions like diabetes, including predicting a hypoglycemic event.
RWE has an important future in treating rare diseases by using existing data and harnessing that to improve treatment among pediatric patients.
Through the rich data in academic healthcare systems, practitioners are better equipped to provide RWE to address important regulatory and research questions.
The creation of a pediatric device patient database, which provides real-time updates to clinical, device and patient-generated health data, offers several regulatory, safety and research advantages in advancing device innovation.
Kolaleh Eskandanian, PhD, MBA, PMP, vice president and chief innovation officer at Children’s National Hospital, and principal investigator for NCC-PDI.
The FDA currently supports RWE demonstration projects that are focused on understanding data quality, improving RWE tools and evaluating RWE approaches to study design and data analytics. Dr. Espinoza highlighted the importance of ongoing dialogue on the use of RWE as it pertains to innovations that advance pediatric healthcare across the board.
“Thank you to the NCC-PDI team for creating this opportunity for PDCs to talk about the impact of real-world evidence on pediatric medical device development and the projects we have to move that field forward,” said Dr. Espinoza, director of CTIP and principal investigator on the PDC’s RWE Demonstration Project. “These projects are intended to inform the FDA and the industry’s approach to RWE including study design, data standards, fitness for use and regulatory decision making and reproducibility. This is complicated work that involves research, IT infrastructure, clinical care and operations.”
NCC-PDI, which is led by the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland, is one of five members of the FDA’s Pediatric Device Consortia Grant Program. To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, with seven devices having received either their FDA market clearance or CE marking.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/Symposium_Final.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-10-16 10:21:382025-03-10 11:19:22Real-world evidence and the impact on pediatric device innovation
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/NCC-PDI-device-competition.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-10-02 12:53:032025-03-10 11:29:24Medical device competition announces six winners to share in $250K
Sixteen finalists have been selected in the “Make Your Medical Device Pitch for Kids!” special COVID-19 edition competition presented by the National Capital Consortium for Pediatric Device Innovation (NCC-PDI). Representing innovations in COVID-19-related pediatric medical devices, the finalists will compete in a virtual pitch event held on July 20,2020 where up to $250,000 in awards will be given. Winners will receive grant funding of up to $50,000.
This competition focuses on pediatric medical devices that support home health monitoring and telehealth, and improve sustainability, resiliency and readiness in diagnosing and treating children during a pandemic.
“As COVID -19 continues to threaten the health of families and children across the nation, we must continue to seek new and better ways to deliver quality care during a pandemic and offer technology solutions to reopen more safely,” says Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “Competitions like this are vital to get ahead of the healthcare challenge that COVID-19 presents in the world of pediatrics. By supporting innovation, we provide critical breakthroughs that can positively impact the lives of the children and families we serve.”
Along with grant funding, one company from the competition will be selected by Johnson & Johnson Innovation – JLABS to receive a one-year residency at JLABS @ Washington, DC, which will be located on the new Children’s National Research & Innovation Campus currently under construction. In addition to the 2021 JLABS residency, the awardee will have access to the JLABS community and expert mentoring by the Johnson & Johnson family of companies.
The 16 pediatric device innovations that judges selected for the final competition include:
Adipomics – simple and fast, one-step COVID-19 diagnostic kit for home or school use
Bloom Standard (Kaaria) – wearable, AI-driven ultrasound for infant cardiac and pulmonary screening and diagnostics
CereVu Medical – remote COVID-19 sensor, monitor and centralized data hub that measures blood oxygen saturation, muscle aches, temperature and trouble breathing
Children’s Hospital of Philadelphia – a transparent reusable DIY origami facemask that reveals facial expressions & improves communication
Children’s National Hospital – Lab-on-a-chip device for high-throughput combination drug screening
Hopscotch – gamified cognitive behavioral therapy-based computer exercises to encourage kids to stay engaged and complete treatment programs
Medichain – cost effective, accurate COVID-19 test with results in minutes and can detect the virus in the early stage
Medipines – monitor device that displays critical respiratory parameters analyzed from a patient’s breathing sample
OtoPhoto – a smart otoscope that quickly and accurately aids diagnosis of ear infections for home telehealth use
OxiWear – continuous wear oxygen-monitoring device used to reduce patient insecurity
REALTROMINS – real time, continuously updated predictive analytics to identify impending mortality in children
SurgiPals – digital assistant and urine biochemical sensor to aid in outpatient care of children with COVID-19
TGV-Dx – a novel, phenotype-based test system for rapid selection of effective antibiotic regimen
VitaScope – quick, accurate infant vital signs to facilitate high-quality virtual care
Vitls – wearable platform for remote patient monitoring of the vitals clinicians require to assess a patient
X-Biomedical – rugged, portable smart ICU ventilator for pediatric and adult patients
Funding for the competition is made possible by a grant from the Food and Drug Administration (FDA) and a philanthropic gift from Mei Xu, founder of e-commerce platform Yes She May, a site dedicated to women-owned brands.
In addition to this COVID-19 special edition event, NCC-PDI recently revealed the ten finalists in its prestigious 8th annual “Make Your Medical Device Pitch for Kids!” competition. Cardiovascular, NICU, and orthopaedic and spine device innovations are the focus of the fall competition, taking place October 7, 2020 as part of the 8th Annual Symposium on Pediatric Device Innovation, presented by Children’s National and co-located with The MedTech Conference powered by AdvaMed.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/NCC-PDI-COVID19-Edition-Competition-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-07-15 15:50:342025-03-10 11:04:24“COVID-19-edition” of pediatric medical device competition announces finalists
The telehealth command center located a few steps away from the cardiac ICU at Children’s National Hospital.
The cardiac critical care team at Children’s National Hospital has developed an innovative Tele-Cardiac Critical Care model aiming to keep constant watch over the most fragile children with critical heart disease in the cardiac ICU. The system combines traditional remote monitoring and video surveillance with an artificial intelligence algorithm trained to flag early warning signs that a critically ill infant may suffer a serious event like cardiac arrest while recovering from complex cardiac surgery. This second set of eyes helps bedside teams improve patient safety and quality of care.
These high risk post-operative patients are often neonates or small infants born with the most complex and critical congenital heart diseases that require surgery or interventional cardiac catheterization in their first days or weeks of life. At these early stages after crucial cardiac surgery, these patients can decompensate dangerously fast with few outward physical symptoms.
The AI algorithm (T3) monitors miniscule changes in oxygen delivery and identifies any mismatch with a child’s oxygen needs. It also tracks and displays small changes in vital sign trends that could lead to a serious complication. The cardiac ICU command center staff then analyzes additional patient data and alerts the bedside team whenever needed.
The Tele-Cardiac Critical Care program started two years ago. In that time, the program has contributed to a significant decrease in post-operative cardiac arrest for this patient population.
“It’s easy to see how a model like this could be adapted to other critical care scenarios, including our other intensive care units and even to adult units,” says Ricardo Munoz, M.D., chief of Cardiac Critical Care and executive director of Telehealth. It allows the physicians and nurses to keep constant watch over these fragile patients without requiring a physician to monitor every heartbeat in person for every patient at every hour of the day to maintain optimal outcomes for all of them.”
Dr. Munoz and Alejandro Lopez-Magallon, M.D., medical director of Telehealth and cardiac critical care specialist, presented data from the pilot program at the American Telemedicine Association’s virtual Annual Meeting on June 26, 2020.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/telemedicine-control-room.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-07-14 14:14:012020-07-14 14:15:50Telehealth and AI reduce cardiac arrest in the cardiac ICU
Karin S. Walsh, Psy.D., and Gerard Gioia, Ph.D., in the Division of Neuropsychology pilot robotic telepresence technology to improve video visits.
The telehealth program at Children’s National Hospital continues to expand access to remote specialty care for families, as well as increase consultation and liaison services to hospitals and clinicians who lack specialty care services on site. The Children’s National Division of Neuropsychology has been a leader in adopting multiple telehealth services including direct-to-consumer video visits, psychotherapy video visits, provider consultations and provider training and supervision.
Telehealth as a whole has been shown to increase access to care, with video visits in particular showing greater clinical and educational impact compared to telephone communications. Despite this, one key limitation has been the immobility of technology used to capture video visits.
To solve for immobility, Karin S. Walsh, Psy.D., is leading a pilot study testing the feasibility and acceptability of telepresence robotics in the division. Robot telepresence devices provide a unique approach to video visits, allowing for extended physical mobility and presence, while expanding interactions between providers and patients, supervisors and trainees and in educational interactions. Traditional video visits demonstrate good feasibility and acceptability by patients, families and staff. This new approach aims to increase the “presence” of the provider and further improve clinical impact, educational impact and patient satisfaction.
The division will initially incorporate two robots into clinical care beginning in May 2020. The pilot study is expected to be carried out over the next 12-18 months, which is particularly timely given the COVID-19 pandemic. The robots, from Double Robotics, offer a high-tech, secure, integrated platform in a device that is user friendly and effective for moving freely through the clinical environment.
“With the addition of the telepresence robots, we anticipate an increase in the quality of care and access for patients and families to neuropsychological specialty care,” says Dr. Walsh. “In addition, given the geographic separation of the program – faculty and trainees are spread across six different locations – the versatile technology will increase the division’s ability to include clinicians with particular expertise into clinical sessions and consultations, as well as in training programs.”
After the pilot study, the team will assess the acceptability of robotic telepresence technology and the special qualities that this modality may offer to enhance quality of care within neuropsychology and within collaborating medical teams.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/Walsh-Neuropsyc-Robotic-Telepresence.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-05-04 14:34:432020-05-04 14:34:43Neuropsychology pilots robotic telepresence technology for telehealth
Children’s National Health System is home to the Rare Disease Institute, the National Organization for Rare Disease’s first Center of Excellence, the largest clinical genetics program in the United States.
With the advent of DNA databanks, informatics, new technology, pediatric consortiums and global partnerships, clinical researchers have never been in a better position to diagnose and treat rare diseases. A rare disease is categorically defined as a condition that affects less than 200,000 people. However, 25 to 30 million Americans, about one in 10, have a rare disease.
Accelerations in genetic research and diagnostic criteria remain one of the most significant accomplishments in medicine, but these breakthroughs invite new challenges: How will researchers provide ongoing care and treatment for patients navigating a rare disease? How can doctors and researchers multiply themselves to ensure everyone has the latest information and resources they need? How can researchers use existing trials to augment other fields? How can we diagnose, catalogue and treat hundreds of new rare diseases each year, while accelerating the research and care of 7,000 existing rare conditions?
If these questions intrigue you, excite you and make you want to collaborate with scientific peers, welcome to the field of genetics. A common theme researchers and families talk about is that rare diseases affect a small proportion of the population, but have a huge impact.
On April 10, 1,200 international researchers, lawmakers, scientists and drug developers from 50 countries will meet in Oxon Hill, Md., 10 miles south of Washington, for a three-day summit, the World Orphan Drug Congress USA, to discuss how to unify efforts to enhance and maximize care for rare disease patients.
Here are eight themes to keep in mind:
Rare diseases are chronic diseases. The human genome project has enabled the molecular mapping of 8,000 diseases with genetic underpinnings. Of these diseases, 600 diseases have therapies. A child born with a urea cycle disorder had a 5% chance of surviving the disease 40 years ago. Now the survival rate is 95%. Helping children survive is essential, but we need to think about the best treatments and standards for long-term care.
Rare diseases are expensive. In Western Australia, according to the 2010 Western Australia Population Cohort, rare diseases account for less than 5% of hospital visits but for 10% of hospital costs. Similar data from Cleveland finds one-third of pediatric hospital visits have a genetic link but account for half of hospital costs.
Rare diseases share common links. We’ve diagnosed 7,000 rare diseases but there are more to unravel. For example, breast cancer has over 30 molecular subtypes – some of which turn into rare diseases. By better understanding these molecular pathways, we may be able to inform common fields of medicine.
Dr. Marshall Summar, a medical geneticist, speaks about the future of rare disease research and treatment at a Rare Disease 101 lecture hosted by the Rare Disease Congressional Caucus on Capitol Hill on Feb. 27. To sustain discoveries, Dr. Summar mentions a digital-first, flexible mindset is essential. Standard language and scalable, universal reference structures are required.
Global partnerships create research repositories. Gold-standard research models – double blind, controlled studies with numerous participants – aren’t possible if five people in the world share the same disease. To increase the number of study participants, global partnerships and longitudinal registries are essential.
Standard language helps. To avoid replicating existing research and to help teams quickly reference findings, we need to adopt standardized language to quantify measurements. Researchers from Berlin and Brazil may help inform the etiology of and future treatments for PKU, but they need to manage, store, access and share their collective findings, while remaining flexible.
The science is here. The FDA is approving more drugs for rare diseases than ever before including gene therapy and micro organs, or Rare Diseases-on-chip models. The challenge with treating so many rare diseases isn’t developing new research, but creating therapies and studies to accommodate this patient volume. About 250 rare disease discoveries happen each year. At the current rate, it will take 2,000 years to treat them all.
Progress is here. The Orphan Drug Act fast-tracked approval for rare disease treatments and therapies, and nearly half of all drugs coming in for FDA approval are for rare diseases. However, only 5% of rare diseases have FDA-approved drugs.
We need to replicate geneticists. To provide optimal care, doctors need to standardize education models and use new forms of technology, such as artificial intelligence and deep learning, to share resources faster via patient education portals, resources for families, CME courses and virtual connections with pediatricians or families.
On March 24, 2019, George Washington University will host their annual George Hacks Medical Hackathon. Among the participants are Seema Khan, M.D., a gastroenterologist, and Kelley Shirron, MSN, CPNP, a nurse practitioner, at Children’s National Health System.
The event is a 24-hour innovation competition at George Washington University that will feature pitches addressing needs for patients battling cancer, medical and social innovation solutions for the aging community and more.
Below, Seema Khan and Kelley Shirron provide insight about the My EoE and BearScope mobile app they are pitching for the competition:
What is the idea surrounding the mobile app you are developing?
We encounter a lot of cases where the patient diagnosis of eosinophilic esophagitis (EoE) and its follow up care are delayed due to a lack of understanding regarding the nature of symptoms, miscommunications related to type of treatment and scheduling as a whole. From the moment the patient visits the doctor to the point of when an endoscopy is scheduled, the process warrants improvement and we believe this mobile app can assist tremendously. The availability of a mobile app like this can make it easier for patients to have better preparation for their procedures.
What are some obstacles that you encounter in relation to endoscopies?
We often experience instances where patients inadvertently violate their NPO (nothing by mouth) order, which results in complete cancellation of their endoscopy procedure. In a case like this, the patient would have to wait another few weeks before they can reschedule an appointment. An NPO violation leads to wasted resources. Mom and Dad took off work, the patient missed school, experienced unnecessary fasting and now they have to do it all over again, resulting in a delay of diagnosis.
How will the mobile app help patients with these issues?
We would like for the mobile app to allow patients to monitor their symptoms, corresponding to their period of treatment. The treatment for our patients is a very important process which requires close adherence. For example, the treatment can be tricky because it resembles the same diet that many kids with food allergies have to adhere to. With this mobile app, the patient could have easy access to that information and identify their food avoidances. The mobile app would identify foods they should avoid in their diet and the seasons they should avoid for scheduling of their scopes due to known seasonal allergies.
How do you envision your patients personally benefitting from the device?
We believe our mobile app can help patients avoid unnecessary pitfalls. For example, the mobile app can incorporate a game or an alarm to remind the patient to drink water or to take their medicine when necessary. A notification can pop up to remind the patient to stop eating and drinking and can detail what that means. Those notifications also include alerts for no gum chewing, hard candies, drinking coffee, etc.
Sometimes patients accidently go to the wrong location. It’s really heartbreaking to experience that because in some cases the patient hasn’t eaten in eight to 12 hours. Many times they’ve endured the pre -colonoscopy “clean out” for those also undergoing a colonoscopy and now we have to reschedule their procedure, all because of a location mix-up. We’re thinking of ways to integrate with WAZE or other navigational apps into this application to help patients coordinate their routes better, which is a helpful feature to have in Washington, D.C. An address of their procedure location could be pre-entered into the mobile app by their provider to avoid location mix-ups. By incorporating this feature, it will help us provide patients with efficient and prompt care.
What excites you about this project?
We’re excited about this because this mobile app could improve the delivery of health care by helping patients and their families identify possible associations between their diet and their symptoms. The content in the app will also help them be better prepared for their diagnostic procedure, and will hopefully reduce last-minute cancellations due to misunderstandings. These capabilities are fun to think about and we’re excited about the creativity that will be incorporated into this project.
Children’s National will also be hosting the 2019 Clinical and Translational Science Institute (CTSI) Healthcare Hackathon on March 29th. The half day hackathon will feature both medical and public health applications developed by participating teams.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/03/Girl-using-smartphone-with-dad.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-03-12 13:20:372024-12-30 12:46:51Children’s National to participate in Hackathon
Dr. Bear Bot’s “robot-only” parking space in the Cardiac ICU. Alejandro Lopez-Magallon, M.D., is featured on the robot display screen, where he drives the robot from his location in the command center, in order to visit patient rooms and capture additional medical information and connect with patients, parents, and attending nurses and physicians.
The telemedicine robot at Children’s National arrived in late August 2018 and recently completed a 90-day test period in the tele-cardiac intensive care unit (cardiac ICU) at Children’s National. The bot travels between rooms as a virtual liaison connecting patients and attending nurses and physicians with Ricardo Munoz, M.D., executive director of the telemedicine program and the division chief of critical cardiac care, and Alejandro Lopez-Magallon, M.D., a cardiologist and medical director of the telemedicine program.
Drs. Munoz and Lopez-Magallon use a nine-screen virtual command center to remotely monitor patient vitals, especially for infants and children who are recovering from congenital heart surgery, flown in for an emergency diagnostic procedure, such as a catheterization, or who are in the process of receiving a heart or kidney transplant. Instead of traveling to individual rooms to check in on the status of one patient, the doctors can now monitor multiple patients simultaneously, enhancing their ability to diagnose, care for and intervene during critical events.
If Drs. Munoz or Lopez-Magallon need to take an X-ray or further examine a patient, they drive the robot from its ‘robot-only’ parking space adjacent to the nurse’s station, and connect with attending doctors and nurses in the teaming area. The onsite clinicians accompany one of the telemedicine doctors, both of whom remain in the command center but appear virtually on the robot’s display screen, to the patient’s room to capture additional medical information and to connect with patients and families.
Over time, the telemedicine team will measure models of efficiency in the tele-cardiac ICU, such as through-put, care coordination, and standards of safety, quality and care, measured by quality of life and short- and long-term patient health outcomes. This test run will serve as a model for future command centers offering remote critical care.
(R) Ricardo Munoz, M.D., executive director of the telemedicine program and the division chief of critical cardiac care, and Alejandro Lopez-Magallon, M.D., a cardiologist and the associate medical director of the telemedicine program in the tele-cardiac ICU command center.
“As technology and medicine advance, so do our models of telemedicine, which we call virtual care,” says Shireen Atabaki, M.D., M.P.H., an emergency medicine physician at Children’s National, who manages an ambulatory virtual health program, which enables patients to use virtual health platforms to connect with doctors, but from the comfort of their home. “We find the patient-centered platforms and this new technology saves families’ time and we’re looking forward to studying internal models to see how this can help our doctors, enabling us to do even more.”
The ongoing virtual connection program that Dr. Atabaki references launched in spring 2016 and has enabled 900 children to connect to a doctor from a computer, tablet or smart phone, which has saved families 1,600 driving hours and more than 41,000 miles over a two-year period. Through this program, virtual care is provided to children in our region by 20 subspecialists, including cardiologists, dermatologists, neurologists, urgent care doctors, geneticists, gastroenterologists and endocrinologists.
To extend the benefits of virtual communication, while saving mileage and time, Dr. Atabaki and the telemedicine team at Children’s National will partner with K-12 school systems, local hospitals and health centers and global health systems.
The Children’s National robot was named Dr. Bear Bot after a 21-day voting period with patients and staff, beating 14 other child-selected names, including SMARTy (Special Medical Access to Remote Technology), Dr. Bot and Rosie. Dr. Bear Bot celebrated with an official reveal party on Valentine’s Day, which was streamed to over 220 patients through the hospital’s closed-circuit television and radio station.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/02/Dr-Bear-Bot.png425300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-02-15 11:16:342024-06-05 12:50:30Advances in telemedicine start with new cardiac critical care robot
The virtual reality surgical system projects images into the operating room, allowing neurosurgeons to revisit the surgical plan in real time.
Neurosurgeons at Children’s National Health System are getting a new three-dimensional (3D) perspective on their cases thanks to an FDA-approved breakthrough virtual reality surgical system.
Children’s National is the first pediatric health system in metropolitan Washington, D.C., to use this state-of-the art system, created by Surgical Theater. It seamlessly integrates patient-specific surgical planning and navigation, professional education and rehearsal.
The technology acquisition was made possible through a generous gift from Sidney & Phyllis Bresler, in honor of their children Alex, Jonathan and Amanda and grandson Theo Charles Bresler, and in loving memory of Joshua Stouck.
“Virtual reality modeling enables us to further explore, analyze and find the best approach for each unique surgical procedure,” said Children’s National President and CEO Kurt Newman, M.D. “This generous gift from Sidney & Phyllis Bresler should translate into better outcomes for many of the more than 17,500 patients who receive surgery at our hospital each year, and will benefit generations to come. We are deeply grateful for the Breslers’ commitment to pediatric innovation.”
The 3D, 360-degree view gives surgeons a cutting-edge digital tool to plan procedures in depth using an accurate capture of the patient’s unique anatomy, and also allows the surgeon to illustrate the surgical path in greater detail than ever before for patients and their families.
“Technology such as Surgical Theater’s represents a quantum leap for neurosurgeons, both in and out of the operating room,” said Robert Keating, M.D., chief of Neurosurgery at Children’s National, in a press release from the company. “It allows us to marry state-of-the-art 3D simulation to the real world; for the patient and family as well as doctors in training, and ultimately offers a new tool for the neurosurgical armamentarium in approaching complex lesions in the brain, such as AVM’s, tumors, epilepsy and functional cases.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/surgical-theater.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-22 11:03:582023-07-03 10:43:30Virtual reality allows surgical planning from every angle
Andrew Dauber, M.D., hosts an AMA chat with Reddit’s science community and offers feedback about height, growth disorders and pediatric endocrinology.
Andrew Dauber, M.D., MMSc., the division chief of endocrinology at Children’s National, spoke about epigenetics – how genes are expressed – and about all things related to pediatric endocrinology in a recent Ask Me Anything (AMA) chat with Reddit’s science community.
We’ve selected highlights from several questions Dr. Dauber received. You can view the full AMA discussion on Reddit.
Q1: What will the future of type 1 diabetes treatment look like?
As a pediatric endocrinologist, Dr. Dauber sees a lot of patients with type 1 diabetes. He predicts technology will pave the way for advancements with continuous glucose monitoring and encourage a ‘real-time’ interaction between patients and providers:
“I anticipate that within a few years, everyone will have access to continuous glucose monitoring technology and that these will be seamlessly connected to insulin pumps or artificial pancreas technologies,” types Dr. Dauber in response to the first AMA question. “I also think there will be more virtual interaction between medical providers and patients with doctors and nurses reviewing blood sugar data in the cloud.”
Q2: What height range is considered normal for a growing child? What is the difference between short stature and a height problem?
The Centers for Disease Control and Prevention has a growth chart, which shows ‘normal’ ranges, based on statistical definitions of height in the general population.
“The truth is that I know plenty of people who have heights below the ‘normal’ population, and they don’t think they have a problem at all,” says Dr. Dauber. “From a genetics point of view, the question can be reframed: When do we call a genetic variant a ‘mutation’ versus a rare variant in the population? For example: If there is a genetic change that 1 in a 1,000 people have that causes you to be 2 inches shorter – is that a problem? Is that a disease?”
“From a clinical perspective, I tend to have a discussion with my patients and their families and ask them how their stature is affecting their lives and whether changing that would really make a meaningful difference,” adds Dr. Dauber. “I believe that this is a very personal decision but people need to be realistic about expected outcomes.”
Q3: What are your favorite case studies about atypical growth or height patterns?
Dr. Dauber references two case studies about growth and puberty:
The growth case study refers to the PAPPA2 gene, which was particularly meaningful for Dr. Dauber since he got to know the family and was able to provide answers to a previously undiagnosed medical mystery about short stature. This research is also opening future studies and analysis about the regulation of IGF-1 bioavailability.
The puberty case study looks at the opposite end of growth and development: precocious puberty. In this case an inherited MKRN3 gene mutation resulted in new insight about the regulation of pubertal timing: Deficiency of MKRN3 caused central precocious puberty in humans. Girls who had inherited the mutated genes from their father (an imprint gene) started to develop breasts before age 6. The results were published in The New England Journal of Medicine.
Q4: What are the differences with consistent and inconsistent growth disorders? Could one arm or leg experience accelerated or stunted growth?
“Most genetic disorders that affect growth will have a uniform effect throughout the body as they are likely to affect all aspects of the skeleton,” says Dr. Dauber. “That being said, there are some notable exceptions such as Russell-Silver syndrome which presents with body asymmetry. There are also somatic mutations (mutations which are just present in some cells in the body) that can lead to segmental areas of overgrowth leading to asymmetry.”
Q5: Can you predict height and growth by looking at genetic factors? What are your thoughts about polygenic risk scores?
“Polygenic risk scores will probably play more of a role in the future to help determine risk of a certain disease,” says Dr. Dauber. “Right now, for most conditions, the risk score does not explain a substantial enough fraction of the variation to help with prediction.”
Dr. Dauber discusses how this works for height, a highly hereditable trait, in The Journal for Clinical Endocrinology and Metabolism. In the review, Dr. Dauber and the study co-authors note that individuals with extreme heights are more likely to have abnormal stature as a result of a severe mutation that causes a growth disorder. For these individuals, whole exome sequencing may reveal gene mutations.
However, the study authors note that for now, the role of these technologies in individuals with extreme stature but without any syndromic features has not been rigorously and systematically explored. (Dr. Dauber and a team of endocrinologists from leading children’s hospitals are currently using electronic health records to study and track these types of genetic clues over time.)
Q6: The general public is excited about genetics and ongoing research, especially with consumer applications – such as genetic tests, including 23andMe. What misconceptions about genetics do people have? What ethical concerns do geneticists share right now?
“Many people think that genetics is completely deterministic,” says Dr. Dauber. “In reality, most genetic variants influence a person’s predisposition toward a trait or disease but don’t actually determine the outcome. Also, the genetic sequence itself is just the first step. Epigenetics, gene regulation, and gene-environment interactions are all important and we are just scratching the surface of understanding these areas.”
“I think that people engaged in genetics research are very interested in the ethical questions,” adds Dr. Dauber. “The problem is that technology is advancing at such a rapid pace, that often consumers are using technologies in ways that we haven’t yet had time to figure out the ethics for. The medical community is often playing catch up.”
Q7: Aside from using gene modifications to cure diseases, where or when should we draw the line in terms of enhancement?
“I think genetic modification for enhancement is a very dangerous slippery slope that we should avoid,” says Dr. Dauber. “We really don’t know the full effect of many genes and by enhancing them, we could be causing lots of problems that we can’t anticipate. There is a reason that evolution is a slow process that happens over millions of years. I think we need to start with the most devastating diseases and try to cure those first.”
Q8: Would it be ethical to use CRISPR on the genes for short stature to produce tall offspring if the risks are sufficiently small? This would be similar to what Dr. He did, but without the ethical violations.
“This is a fascinating question and it will become more of an issue over time,” says Dr. Dauber. “Where do we draw the line between fixing, preventing disease and enhancing physical function? Personally, I think using genome editing to promote height is a terrible idea. Our current perception that taller height is more desirable is a social construct and varies by culture. This idea also changes over time.”
Q9: Overall, how does this fit into meeting unmet medical needs?
“I would be very wary about trying to design our children’s physical features,” Dr. Dauber notes. “We need to figure out as a society what diseases are sufficiently problematic that we feel comfortable trying to eliminate them via genome editing.”
Q10: How many genes control acromegaly? Is it possible (in theory) to Top of Formselect them just to gain the positive effects of gigantism without the health risks?
Dr. Dauber explains that acromegaly, a condition often referred to as gigantism, is caused by a growth hormone-producing tumor. There are a few genes known to cause these tumors, including the AIP, and there was recently a genetic cause of X-linked gigantism, which was published in The New England Journal of Medicine.
“This basic idea is a good one,” notes Dr. Dauber. “We can find genes that when mutated can cause tall stature – and then try to manipulate those pathways. A great example is the NPR2 gene, which when mutated can cause short or tall stature. This pathway is being targeted for therapeutics related to achondroplasia.”
The National Institutes of Health (NIH) refers to achondroplasia as ‘short-limbed dwarfism,’ which results in an average-sized trunk with short limbs, especially arms and legs, due to a lack of cartilage turning into bone. The average height of an adult male with achondroplasia is 4 feet, 4 inches, while the average height of adult females with achondroplasia is less than 4 feet, 1 inch. In this case, manipulating growth pathways may help alleviate health problems associated with achondroplasia: lack of mobility or range of motion, an enlarged head, apnea, ear infections and spinal stenosis, or a compression or pinching of the spinal cord.
Q11: Give us a history lesson. Why are there variations of height within populations, such as Asia and Latin America?
“The average height in a population is due to the influence of literally thousands of common genetic variants,” says Dr. Dauber. “These population differences have evolved over thousands of years due to a combination of migration and selection. There is a well-known difference in the genetic makeup of various populations which likely underlies the differences across the globe. There are even differences within Europe.”
Q12: Are there examples of pseudoscience or theories about growth, such as recommendations to eat a certain food instead of taking growth hormones to correct for a growth disorder, which runs contrary to scientific evidence, that drive you crazy?
“I don’t really get bothered by crazy theories, but it is upsetting when patients and their families get swindled into spending their money on therapies that aren’t truly effective,” says Dr. Dauber. “People ask me all the time if a certain food or exercise can make their child taller. The bottom line is that in a well-nourished (and healthy) child, there is no magical food that is going to make them tall.”
Q13: According to almost every theory of how life evolved on Earth, from religion to evolution, we all have one common ancestor. In theory doesn’t that make us all cousins?
“Yes, just very distant ones,” says Dr. Dauber. “People always point out the vast number of differences between races but in fact we are all more than 99.9 percent identical on a genetic level.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/Dauber-Reddit-AMA.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-27 10:27:082024-05-16 14:49:48Thirteen questions for a pediatric endocrinologist
Rebecca Cady, vice president and chief risk officer at Children’s National Health System, is the recipient of the 2018 American Society for Health Care Risk Management (ASHRM ) Professional of the Year award. Cady’s dedication to advancing the risk management industry has been demonstrated through her commitment to innovation in the face of industry challenges.
Recently, she directed the implementation process for reporting safety incidents via a mobile app created by RL Solutions. Children’s National was one of the early adopters of the mobile app technology that has allowed staff to instantaneously provide feedback about unsafe conditions directly from their smartphones.
“The mobile app enables staff to report an event quickly so that it doesn’t get lost or forgotten and something can be done about it,” Cady says. “We already were working on a project to increase incident reporting, so integrating the mobile app was an important addition for providers looking to report issues of concern.”
Cady is in charge of the Children’s National enterprise risk management department and management of their litigation program; including serving as counsel to the compliance officer and Human Resources. She also oversees operations of Children’s clinical risk management program, ombudsman program, workers’ compensation program and the insurance program; including managing the organization’s captive insurance company.
Her approach consistently applies diverse tools and strategies of risk management, such as enterprise risk management (ERM), strategic risk management, risk financing and insurance. At Children’s National, she has built an ERM infrastructure that enables faster understanding of risk management and adoption by staff at all levels. This led to adopting incident reporting on mobile devices and resulted in overall improvements in hospital performance.
Previously, Cady served as interim vice president, chief compliance and privacy officer at Children’s National. Prior to joining Children’s National, she was a partner at Grace Hollis Lowe Hanson & Schaeffer LLP.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/11/Rebecca-Cady.png400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-11-08 11:44:352018-11-19 10:47:46Rebecca Cady named Health Care Risk Management Professional of the Year by ASHRM














 Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.
Six medical technology innovators focused on pediatric cardiology were selected to receive grants of $50,000 each in the “Make Your Medical Device Pitch for Kids!TM” competition in Toronto. The funds will help awardees bring their devices to the market and improve care for children with heart conditions.