Children’s National at the American Epilepsy Society Annual Meeting
 Several experts from Children’s National Hospital will be sharing their knowledge at the upcoming American Epilepsy Society Annual Meeting in Orlando, December 1-5. Here’s a sample of what you can expect.
Several experts from Children’s National Hospital will be sharing their knowledge at the upcoming American Epilepsy Society Annual Meeting in Orlando, December 1-5. Here’s a sample of what you can expect.
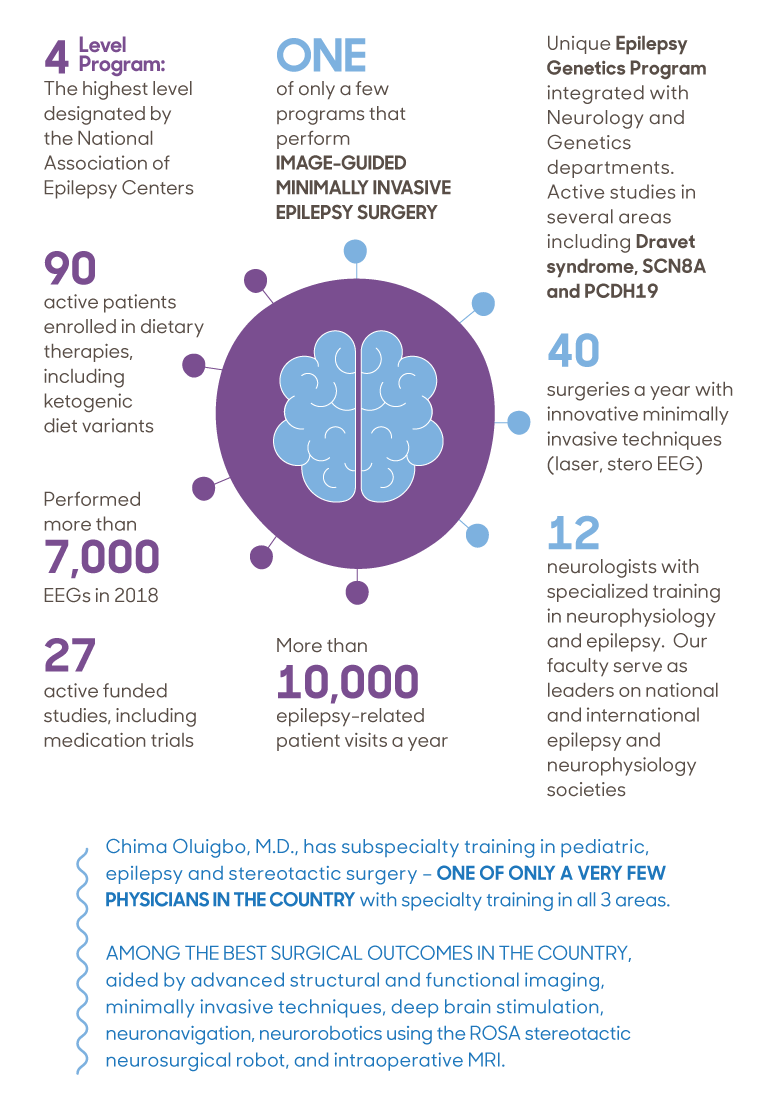
- Chima Oluigbo, M.D., a pediatric neurosurgeon, will be on panel with other surgeons discussing different surgical techniques and approaches related to epilepsy surgery followed by hands-on practice at teaching stations. He will focus on extra-temporal epilepsy scenarios and will be presenting on Nuances of Temporal Lobe Surgery in the Pediatric Population at the Neurosurgery Symposium highlighting Surgical Controversies in Temporal Lobe Epilepsies.
- Ersida Buraniqi, M.D., a child neurologist, will be part of a special interest group on critical care and discuss advances in electroencephalography (EEG) and multimodal neuro-monitoring for seizures in the intensive care unit (ICU). Dr. Buranigui will be doing a special presentation on EEG features to predict electrographic seizures and mortality in the pediatric intensive care unit (PICU).
- Dana Harrar, M.D., director of Pediatric Stroke Program and co-director of Critical Care Neurology, is presenting at an invitation-only resident EEG course, providing an interactive structured curriculum on pediatric and adult EEG. Dr. Harrar will be focusing on doing an ICU-EEG nomenclature overview.
- Madison Berl, Ph.D., director of Neuropathy Research and of the Intellectual and Developmental Disabilities Research Center Program, will be presenting during the AES Annual Course. The topic “It’s About Time” will focus on the critical importance the timing in epilepsy care plays in patient outcome. Dr. Berl will be presenting on neuropsych outcomes.
- Leigh Sepeta, Ph.D., director of Inpatient Neuropsychology, is the vice-chair of the special interest group on neuropsychology. Additionally, Freya Prentice, M.Sc., will be doing a presentation during this session on functional mapping of the cognitive memory circuit in pediatric epilepsy.
| Date | Time | Presenter(s) | Title |
| 12/2/23 | 8:00 am | Chima Oluigbo, M.D., FRCSC, FAANS | Skills Workshop | Epilepsy Surgery Workshop: Techniques and Clinical Scenarios |
| 12/2/23 | 5:30 pm | Chima Oluigbo, M.D., FRCSC, FAANS | SIG | Epilepsy Surgery: Homunculus Revisited: Managing Central Lobe Epilepsies |
| 12/2/23 | 5:30 pm | Ersida Buraniqi, M.D. | SIG | Critical Care: Advances in EEG and Multimodal Neuro-monitoring for Seizures in the ICU |
| 12/2/23 | 7:00am | Dana Harrar M.D. | Resident EEG Course |
| 12/3/23 | 9:00 am | Chima Oluigbo, M.D., FRCSC, FAANS | Neurosurgery Symposium | Surgical Controversies in Temporal Lobe Epilepsies |
| 12/3/23 | 8:45 am | Madison Berl, Ph.D. | Annual Course | It’s About Time: Timing in Epilepsy Evaluation and Treatment |
| 12/4/23 | 7:00 am | Leigh Sepeta, M.D. | SIG | Neuropsychology: Mapping Cognition in Epilepsy: From the Lab to the Clinic |
| 12/4/23 | 7:00 am | Freya Prentice, M.D. | SIG | Neuropsychology: Mapping Cognition in Epilepsy: From the Lab to the Clinic |
| 12/5/23 | 7:00 am | Dana Harrar M.D. | SIG | Epilepsy Education: Epilepsy Education Throughout the Training Pipeline |



 Children’s National Hospital named
Children’s National Hospital named 

 The choice between stereoelectroencephalography (SEEG) and subdural evaluation is not mutually exclusive, according to a new
The choice between stereoelectroencephalography (SEEG) and subdural evaluation is not mutually exclusive, according to a new