Our neurosurgery team is among the most experienced in the nation. We have performed thousands of surgeries and are dedicated to giving the best possible care. The Children’s National Hospital Division of Neurosurgery consistently ranks among the country’s top programs according to U.S. News & World Report.
Patients travel to us from all over the world because we have the resources and expertise necessary to care for their neurological conditions through multidisciplinary programs such as:
The Children’s National Hospital Division of Neurosurgery is among the first in the country to develop new techniques and adopt the latest technologies that make minimally invasive neurosurgery possible by utilizing state of the art equipment and developing new techniques, including:
Children’s National is involved in cutting edge scientific research offering new hope for our patients and new methods of treatment. Our doctors have developed some of the most advanced treatments and clinics for our patients including:
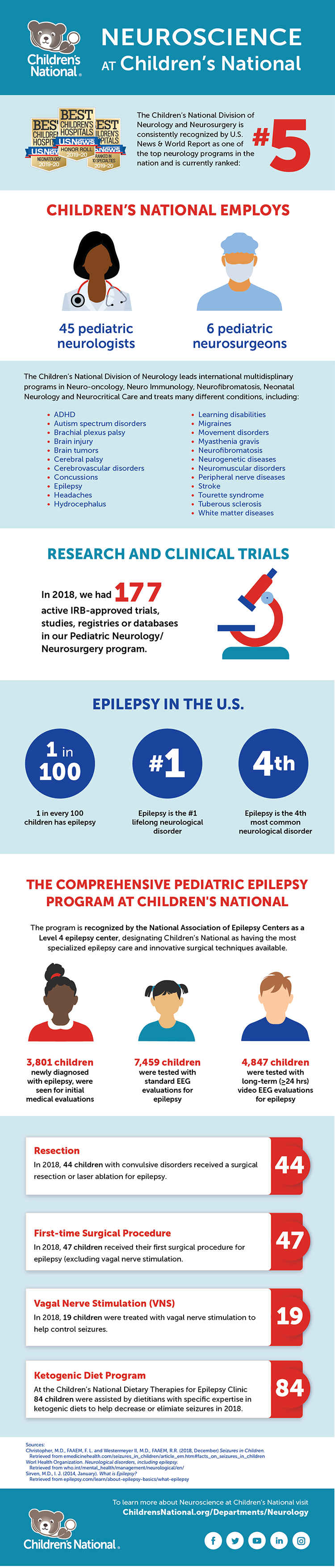
U.S. News & World Report ranks our neurosurgery program number five in the nation, reflecting our commitment to excellence in care for our patients and families.
Children’s National is one of only 12 children’s hospitals in the country to attain Level 1 Surgery Verification from the American College of Surgeons.

Children with rare and medically complex conditions, such as brain tumors, craniofacial disorders, Chiari malformations, vascular disorders and brachial plexus palsy, to name a few, achieve exceptional outcomes at Children’s National. Our patients experience fewer complications, go home sooner and maintain long-term symptom relief.
Our entire team is dedicated to meeting your child’s unique needs. Our Neuro-Intensive Care Unit nurses recognize signs of pain and complications your child may not be able to explain.
Children’s National is at the forefront of new device-based treatments that not only fix neurologic problems, but also restore brain function. We are one of the few pediatric programs in the country offering dedicated pediatric deep brain stimulation, which uses a pacemaker-like device to significantly reduce the burden of movement disorders and difficult-to-control epilepsy, as well as Neuropace implantation to help with seizures in eloquent areas of the brain.
We are proudly training the next generation of pediatric neurosurgeons through residency programs and fellowships in conjunction with several area medical schools.


“The AES, is one of the oldest neurological professional organizations in the country dedicated to the scientific investigation, exchange of clinical information and eradication of epilepsy and associated disorders, and I’m honored to serve as the new president,” Dr. Gaillard said.
In early December 2019, William D. Gaillard, M.D., chief of the Divisions of Child Neurology, Epilepsy and Neurophysiology at Children’s National Hospital, began his term as president of the American Epilepsy Society (AES) at the annual meeting in Baltimore. The AES is a medical and scientific society with over 4,000 members consisting of clinicians, scientists investigating basic and clinical aspects of epilepsy, and other professionals interested in seizure disorders.
“The AES, is one of the oldest neurological professional organizations in the country dedicated to the scientific investigation, exchange of clinical information and eradication of epilepsy and associated disorders, and I’m honored to serve as the new president,” Dr. Gaillard said.
Dr. Gaillard’s clinical research focuses on the use of advanced imaging to investigate the effect of childhood epilepsy on brain structure and function with an emphasis on cognitive systems. His group also develops and implements imaging strategies to improve epilepsy outcomes.
In addition, Dr. Gaillard, an active participant in AES activities, has served as treasurer and as chair of the Clinical Investigator Workshop and Pediatric Content Committees. He also serves as an associate editor for the journal Epilepsy Research, and as a regular reviewer on AES and Epilepsy Foundation study sections.
As division chief of Child Neurology, Epilepsy and Neurophysiology, Dr. Gaillard directs a team of pediatric specialists who see thousands of patients each year. Dr. Gaillard has worked throughout his career to care for children and young adults with epilepsy from the onset of seizures through novel therapeutic interventions, medication trials and, when appropriate, surgery. Treatment options at Children’s National addresses the full range of the condition, including problems of difficult-to-control epilepsy. Additionally, treatment includes the concurrent social, education and emotional issues faced by children with the condition and their families.
His academic appointments include Professor of Pediatrics and Neurology at George Washington University, Professor of Neurology at Georgetown University, and Professor (adjunct), Hearing and Speech, University of Maryland, College Park.
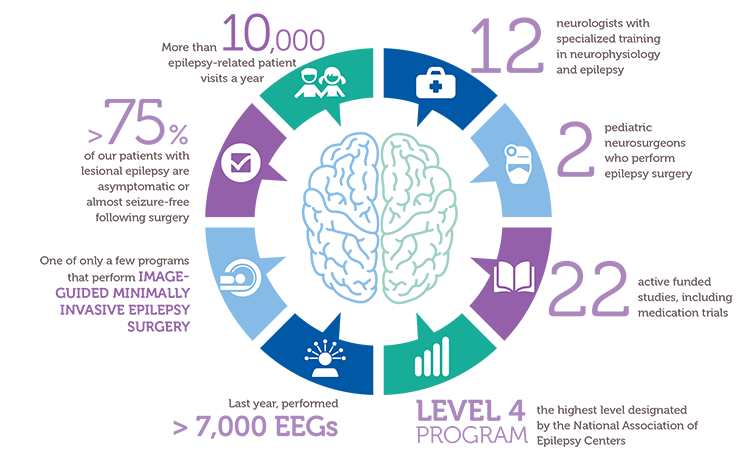
Epilepsy is one of the most common neurological conditions that lasts a lifetime, and, in extreme cases, can lead to death. It affects one out of every 26 people across their lifetime, and 8% of children will have a seizure before leaving childhood. One in 10 children with epilepsy is a candidate for surgery.
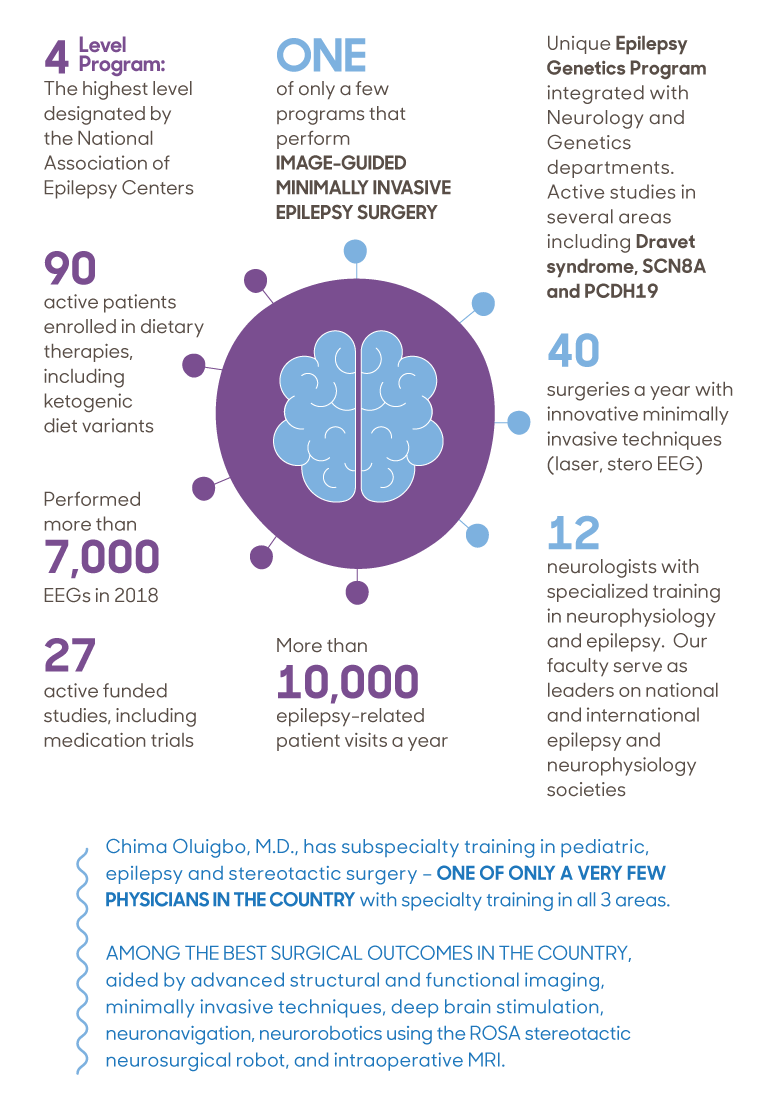
Children’s National has one of the largest and most experienced multidisciplinary epilepsy programs in the country with a range of programs specializing in new onset epilepsy, the ketogenic diet, intractable epilepsy, neuroinflammation, neurogenetics, epilepsy surgery, epileptic encephalopathy and more.
The Children’s National epilepsy program is continuously working to improve care for patients through clinical innovation, growing our team and expanding access in locations throughout the region.
To refer a patient or learn more about our program, call 202-476-3611 or visit ChildrensNational.org/Epilepsy.
The brain comprises only 2% of the body’s volume, but it uses more than 20% of its energy, which makes this organ particularly vulnerable to changes in metabolism.
More than 30 million Americans have diabetes, with the vast majority having Type 2 disease. Characterized by insulin resistance and persistently high blood sugar levels, poorly controlled Type 2 diabetes has a host of well-recognized complications: compared with the general population, a greatly increased risk of kidney disease, vision loss, heart attacks and strokes and lower limb amputations.
But more recently, says Nathan A. Smith, MS, Ph.D., a principal investigator in Children’s National Research Institute’s Center for Neuroscience Research, another consequence has become increasingly apparent. With increasing insulin resistance comes cognitive damage, a factor that contributes significantly to dementia diagnoses as patients age.
The brain comprises only 2% of the body’s volume, but it uses more than 20% of its energy, Smith explains – which makes this organ particularly vulnerable to changes in metabolism. Type 2 diabetes and even prediabetic changes in glucose metabolism inflict damage upon this organ in mechanisms with dangerous synergy, he adds. Insulin resistance itself stresses brain cells, slowly depriving them of fuel. As blood sugar rises, it also increases inflammation and blocks nitric oxide, which together narrow the brain’s blood vessels while also increasing blood viscosity.
When the brain’s neurons slowly starve, they become increasingly inefficient at doing their job, eventually succumbing to this deprivation. These hits don’t just affect individual cells, Smith adds. They also affect connectivity that spans across the brain, neural networks that are a major focus of his research.
While it’s well established that Type 2 diabetes significantly boosts the risk of cognitive decline, Smith says, it’s been unclear whether this process might be halted or even reversed. It’s this question that forms the basis of a collaborative Frontiers grant, $2.5 million from the National Science Foundation split between his laboratory; the lead institution, Stony Brook University; and Massachusetts General Hospital/Harvard Medical School.
Smith and colleagues at the three institutions are testing whether changing the brain’s fuel source from glucose to ketones – byproducts from fat metabolism – could potentially save neurons and neural networks over time. Ketones already have shown promise for decades in treating some types of epilepsy, a disease that sometimes stems from an imbalance in neuronal excitation and inhibition. When some patients start on a ketogenic diet – an extreme version of a popular fat-based diet – many can significantly decrease or even stop their seizures, bringing their misfiring brain cells back to health.
Principal Investigator Smith and his laboratory at the Children’s National Research Institute are using experimental models to test whether ketones could protect the brain against the ravages of insulin resistance. They’re looking specifically at interneurons, the inhibitory cells of the brain and the most energy demanding. The team is using a technique known as patch clamping to determine how either insulin resistance or insulin resistance in the presence of ketones affect these cells’ ability to fire.
They’re also looking at how calcium ions migrate in and out of the cells’ membranes, a necessary prerequisite for neurons’ electrical activity. Finally, they’re evaluating whether these potential changes to the cells’ electrophysiological properties in turn change how different parts of the brain communicate with each other, potentially restructuring the networks that are vital to every action this organ performs.
Colleagues at Athinoula A. Martinos Center for Biomedical Imaging at Massachusetts General Hospital and Harvard Medical School, led by Principal Investigator Eva-Maria Ratai, Ph.D., will perform parallel work in human subjects. They will use imaging to determine how these two fuel types, glucose or ketones, affect how the brain uses energy and produces the communication molecules known as neurotransmitters. They’re also investigating how these factors might affect the stability of neural networks using techniques that investigate the performance of these networks both while study subjects are at rest and performing a task.
Finally, colleagues at the Laufer Center for Physical and Quantitative Biology at Stony Brook University, led by Principal Investigator Lilianne R. Mujica-Parodi, Ph.D., will use results generated at the other two institutions to construct computational models that can accurately predict how the brain will behave under metabolic stress: how it copes when deprived of fuel and whether it might be able to retain healthy function when its cells receive ketones instead of glucose.
Collectively, Smith says, these results could help retain brain function even under glucose restraints. (For this, the research team owes a special thanks to Mujica-Parodi, who assembled the group to answer this important question, thus underscoring the importance of team science, he adds.)
“By supplying an alternate fuel source, we may eventually be able to preserve the brain even in the face of insulin resistance,” Smith says.


At the age of 17, Jake underwent surgery led by neurosurgeon Chima Oluigbo, M.D., where he conducted a temporal lobe resection, also called temporal lobectomy, that works to lower the number of seizures, make them less severe or stop them completely. The surgery ended up being successful and it worked to greatly improve his overall quality of life.
Since 1969, November has been considered Epilepsy Awareness Month to highlight the importance of recognizing a seizure and promoting seizure first aid. At Children’s National Hospital, doctors in the division of neurology are committed to finding treatments for epilepsy and have done just that by helping Jacob Yates, an 18-year-old patient, get his life back.
For many families the holidays are meant for spending time with loved ones and enjoying the seasonal festivities. However, the holidays were not always a joyous occasion for Jake and his family. Since he was a baby, many of his holidays were spent in a bed due to a brain disorder that caused him to have developmental delays and, at times, up to 17 seizures a day.
“The holidays were always a tough time for the family because Jake would get so excited around Christmas that it would overwhelm his system and induce seizures that took him days to recover from,” says his mom, Jennifer.
Jake was born a preemie and hours after he was born, doctors at his local hospital had identified that he was having trouble breathing. By coincidence, the Children’s National transport team was on-site to take another patient to Children’s National, but once they looked at Jake they immediately took him instead by SkyBear Air Transport, the hospital’s rapid helicopter transport service.
During his stay at Children’s National, Jake was in the neonatal intensive care unit (NICU) for 11 days and was supported by breathing machines to help with respiratory distress and other issues stemming from him being born prematurely.
“If it wasn’t for the Children’s National transport team coincidentally being at our local hospital, Jake wouldn’t have survived staying at that location,” said Jennifer.
After he was taken care of at Children’s National, he was discharged 11 days later, but at the age of three months Jake was still experiencing respiratory issues and was taken back to his local hospital in Charles County.
“When he first arrived back at the University of Maryland Charles Regional Medical Center, the doctors thought he may have had cystic fibrosis, but it came back that perhaps he was suffering from reflux and they put him on medication,” Jennifer recalls. Unfortunately, this was not the cause and it would not be the family’s last visit to the hospital.
By the age of six months, Jake had his first seizure and he was flown back to Children’s National. Over the next year he was repeatedly admitted to the hospital as his seizures had caused him to stop breathing.
Between the ages of 4 to 6 years old, Jake became a patient of William D. Gaillard, M.D., division chief of epilepsy and neurophysiology and Roger Packer, M.D., senior vice president at the Center of Neuroscience and Behavioral Health at Children’s National. After his visit, both doctors recommended surgery, but Dr. Packer recommended that Jake receive an electroencephalogram (EEG), magnetic resonance imaging (MRI) and go through a sleep study first to identify the specific causes of his seizures.
Now on a new medication, his seizures were maintained for the most part, but doctors were still recommending that it was time for surgery. When Jake was 15, his parents re-evaluated the surgery and learned that their son had a 76% chance of being seizure and medication free.
At the age of 17, Jake underwent surgery led by Chima Oluigbo, M.D., neurosurgeon at Children’s National, where he conducted a temporal lobe resection, also called temporal lobectomy, that works to lower the number of seizures, make them less severe or stop them completely. The surgery ended up being successful and it worked to greatly improve his overall quality of life.
Before the surgery, Jake didn’t speak much, experienced anxiety and had difficulty expressing his emotions. He had never told his mother that he loved her. After the surgery, Jake looked at his mother and said, “I love you babe.”
According to Jennifer, since the surgery her son is a completely different person and states that he has been seizure free for over a year. Equally, Jake and the family can now all look forward to the holidays.
“We’re so excited to have him share the holidays,” Jennifer says. “He feels better and it shows through his attitude and the way he responds to things. Words can’t express the gratitude we have for the doctors at Children’s National Hospital. They gave my son his life back.”


Andrea L. Gropman, M.D.: We have collected many years of longitudinal clinical data, but with this new funding now we can answer questions about these diseases that are meaningful on a day-to-day basis for patients with urea cycle disorders.
An international research consortium co-led by Andrea L. Gropman, M.D., at Children’s National Hospital has received $5 million in federal funding as part of an overall effort to better understand rare diseases and accelerate potential treatments to patients.
Urea cycle disorder, one such rare disease, is a hiccup in a series of biochemical reactions that transform nitrogen into a non-toxic compound, urea. The six enzymes and two carrier/transport molecules that accomplish this essential task reside primarily in the liver and, to a lesser degree, in other organs.
The majority of patients have the recessive form of the disorder, meaning it has skipped a generation. These kids inherit one copy of an abnormal gene from each parent, while the parents themselves were not affected, says Dr. Gropman, chief of the Division of Neurodevelopmental Pediatrics and Neurogenetics at Children’s National. Another more common version of the disease is carried on the X chromosome and affects boys more seriously that girls, given that boys have only one X chromosome.
Regardless of the type of urea cycle disorder, when the urea cycle breaks down, nitrogen converts into toxic ammonia that builds up in the body (hyperammonemia), particularly in the brain. As a result, the person may feel lethargic; if the ammonia in the bloodstream reaches the brain in high concentrations, the person can experience seizures, behavior changes and lapse into a coma.
Improvements in clinical care and the advent of effective medicines have transformed this once deadly disease into a more manageable chronic ailment.
“It’s gratifying that patients diagnosed with urea cycle disorder now are surviving, growing up, becoming young adults and starting families themselves. Twenty to 30 years ago, this never would have seemed conceivable,” Dr. Gropman says. “We have collected many years of longitudinal clinical data, but with this new funding now we can answer questions about these diseases that are meaningful on a day-to-day basis for patients with urea cycle disorders.”
In early October 2019, the National Institutes of Health (NIH) awarded the Urea Cycle Disorders Consortium for which Dr. Gropman is co-principal investigator a five-year grant. This is the fourth time that the international Consortium of physicians, scientists, neuropsychologists, nurses, genetic counselors and researchers has received NIH funding to study this group of conditions.
Dr. Gropman says the current urea cycle research program builds on a sturdy foundation built by previous principal investigators Mendel Tuchman, M.D., and Mark Batshaw, M.D., also funded by the NIH. While previous rounds of NIH funding powered research about patients’ long-term survival prospects and cognitive dysfunction, this next phase of research will explore patients’ long-term health.
Among the topics they will study:
Long-term organ damage. Magnetic resonance elastrography (MRE) is a state-of-the-art imaging technique that combines the sharp images from MRI with a visual map that shows body tissue stiffness. The research team will use MRE to look for early changes in the liver – before patients show any symptoms – that could be associated with long-term health impacts. Their aim is spot the earliest signs of potential liver dysfunction in order to intervene before the patient develops liver fibrosis.
Academic achievement. The research team will examine gaps in academic achievement for patients who appear to be underperforming to determine what is triggering the discrepancy between their potential and actual scholastics. If they uncover issues such as learning difficulties or mental health concerns like anxiety, there are opportunities to intervene to boost academic achievement.
“And if we find many of the patients meet the criteria for depression or anxiety disorders, there are potential opportunities to intervene. It’s tricky: We need to balance their existing medications with any new ones to ensure that we don’t increase their hyperammonemia risk,” Dr. Gropman explains.
Neurologic complications. The researchers will tap continuous, bedside electroencephalogram, which measures the brain’s electrical activity, to detect silent seizures and otherwise undetectable changes in the brain in an effort to stave off epilepsy, a brain disorder that causes seizures.
“This is really the first time we will examine babies’ brains,” she adds. “Our previous imaging studies looked at kids and adults who were 6 years and older. Now, we’re lowering that age range down to infants. By tracking such images over time, the field has described the trajectory of what normal brain development should look like. We can use that as a background and comparison point.”
In the future, newborns may be screened for urea cycle disorder shortly after birth. Because it is not possible to diagnose it in the womb in cases where there is no family history, the team aims to better counsel families contemplating pregnancy about their possible risks.
Research described in this post was underwritten by the NIH through its Rare Diseases Clinical Research Network.


“The Cute Syndrome Foundation reached out because children with this disorder are dying. They were hoping to find a way to make more people, especially medical professionals, aware of this disorder and treatment recommendations,” said John Schreiber, M.D.
Children’s National Health System is proud to share that they have launched into a 6-month pilot research program to evaluate and improve education and access to care for SCN8A-related epilepsy. Due to advances in genetic testing, more patients with SCN8A mutations and other rare genetic epilepsies are being discovered all the time.
The research for the pilot program is being led by John Schreiber, M.D., assistant professor of neurology and pediatrics and director of the epilepsy genetics program at Children National. Dr. Schreiber will help to develop a more focused effort to provide families and clinicians with the Clinician Information and Reference Guide that was created by The Cute Syndrome Foundation. The goal of the information is to provide families and clinicians with a guide to remove barriers to access expert care.
“The Cute Syndrome Foundation reached out because children with this disorder are dying. They were hoping to find a way to make more people, especially medical professionals, aware of this disorder and treatment recommendations,” said Dr. Schreiber. “We’re at a critical point of collecting information as patients from around the world are looking at Children’s National as a leader to combat this type of disorder.”
As the first study of its kind in a rare genetic epilepsy, the pilot will provide the opportunity for future interventions that will help elevate the profile of SCN8A-related disorders, improve overall patient outcomes and facilitate collaborative partnerships that focus on research and on supporting positive outcomes for patients.
To help uncover barriers to accessing expert advice, the SCN8A survey was given out to over 200 health care professionals at Children’s National 2019 Pediatric Neurology Update meeting. Specifically, the study will help doctors at Children’s National increase provider knowledge of SN8A-related disorders, improve utilization of appropriate anti-seizure therapies and may ultimately end up reducing mortality.
Children’s National received a gift of $15,397 to establish the SCN8A Education and Research Fund, which will support research within the Comprehensive Pediatric Epilepsy Program to evaluate access to and increase awareness of SCN8A epileptic encephalopathy and treatment recommendation from experts in the field. The funds will be used for personnel, technology and material costs associated with the research.


Billie Lou Short, M.D., received the Ninth Annual Mentorship Award in Clinical Science.
People joke that Billie Lou Short, M.D., chief of Children’s Division of Neonatology, invented extracorporeal membrane oxygenation, known as ECMO for short. While Dr. Short did not invent ECMO, under her leadership Children’s National was the first pediatric hospital to use it. And over decades Children’s staff have perfected its use to save the lives of tiny, vulnerable newborns by temporarily taking over for their struggling hearts and lungs. For two consecutive years, Children’s neonatal intensive care unit has been named the nation’s No. 1 for newborns by U.S. News & World Report. “Despite all of these accomplishments, Dr. Short’s best legacy is what she has done as a mentor to countless trainees, nurses and faculty she’s touched during their careers. She touches every type of clinical staff member who has come through our neonatal intensive care unit,” says An Massaro, M.D., director of residency research.
For these achievements, Dr. Short received the Ninth Annual Mentorship Award in Clinical Science.
Anna Penn, M.D., Ph.D., has provided new insights into the central role that the placental hormone allopregnanolone plays in orderly fetal brain development, and her research team has created novel experimental models that mimic some of the brain injuries often seen in very preterm babies – an essential step that informs future neuroprotective strategies. Dr. Penn, a clinical neonatologist and developmental neuroscientist, “has been a primary adviser for 40 mentees throughout their careers and embodies Children’s core values of Compassion, Commitment and Connection,” says Claire-Marie Vacher, Ph.D.
For these achievements, Dr. Penn was selected to receive the Ninth Annual Mentorship Award in Basic and Translational Science.
The mentorship awards for Drs. Short and Penn were among dozens of honors given in conjunction with “Frontiers in Innovation,” the Ninth Annual Research and Education Week (REW) at Children’s National. In addition to seven keynote lectures, more than 350 posters were submitted from researchers – from high-school students to full-time faculty – about basic and translational science, clinical research, community-based research, education, training and quality improvement; five poster presenters were showcased via Facebook Live events hosted by Children’s Hospital Foundation.
Two faculty members won twice: Vicki Freedenberg, Ph.D., APRN, for research about mindfulness-based stress reduction and Adeline (Wei Li) Koay, MBBS, MSc, for research related to HIV. So many women at every stage of their research careers took to the stage to accept honors that Naomi L.C. Luban, M.D., Vice Chair of Academic Affairs, quipped that “this day is power to women.”
Here are the 2019 REW award winners:
2019 Elda Y. Arce Teaching Scholars Award
Barbara Jantausch, M.D.
Lowell Frank, M.D.
Suzanne Feetham, Ph.D., FAA, Nursing Research Support Award
Vicki Freedenberg, Ph.D., APRN, for “Psychosocial and biological effects of mindfulness-based stress reduction intervention in adolescents with CHD/CIEDs: a randomized control trial”
Renee’ Roberts Turner for “Peak and nadir experiences of mid-level nurse leaders”
2019-2020 Global Health Initiative Exploration in Global Health Awards
Nathalie Quion, M.D., for “Latino youth and families need assessment,” conducted in Washington
Sonia Voleti for “Handheld ultrasound machine task shifting,” conducted in Micronesia
Tania Ahluwalia, M.D., for “Simulation curriculum for emergency medicine,” conducted in India
Yvonne Yui for “Designated resuscitation teams in NICUs,” conducted in Ghana
Xiaoyan Song, Ph.D., MBBS, MSc, “Prevention of hospital-onset infections in PICUs,” conducted in China
Ninth Annual Research and Education Week Poster Session Awards
Basic and Translational Science
Faculty: Adeline (Wei Li) Koay, MBBS, MSc, for “Differences in the gut microbiome of HIV-infected versus HIV-exposed, uninfected infants”
Faculty: Hayk Barseghyan, Ph.D., for “Composite de novo Armenian human genome assembly and haplotyping via optical mapping and ultra-long read sequencing”
Staff: Damon K. McCullough, BS, for “Brain slicer: 3D-printed tissue processing tool for pediatric neuroscience research”
Staff: Antonio R. Porras, Ph.D., for “Integrated deep-learning method for genetic syndrome screening using facial photographs”
Post docs/fellows/residents: Lung Lau, M.D., for “A novel, sprayable and bio-absorbable sealant for wound dressings”
Post docs/fellows/residents: Kelsey F. Sugrue, Ph.D., for “HECTD1 is required for growth of the myocardium secondary to placental insufficiency”
Graduate students: Erin R. Bonner, BA, for “Comprehensive mutation profiling of pediatric diffuse midline gliomas using liquid biopsy”
High school/undergraduate students: Ali Sarhan for “Parental somato-gonadal mosaic genetic variants are a source of recurrent risk for de novo disorders and parental health concerns: a systematic review of the literature and meta-analysis”
Clinical Research
Faculty: Amy Hont, M.D., for “Ex vivo expanded multi-tumor antigen specific T-cells for the treatment of solid tumors”
Faculty: Lauren McLaughlin, M.D., for “EBV/LMP-specific T-cells maintain remissions of T- and B-cell EBV lymphomas after allogeneic bone marrow transplantation”
Staff: Iman A. Abdikarim, BA, for “Timing of allergenic food introduction among African American and Caucasian children with food allergy in the FORWARD study”
Staff: Gelina M. Sani, BS, for “Quantifying hematopoietic stem cells towards in utero gene therapy for treatment of sickle cell disease in fetal cord blood”
Post docs/fellows/residents: Amy H. Jones, M.D., for “To trach or not trach: exploration of parental conflict, regret and impacts on quality of life in tracheostomy decision-making”
Graduate students: Alyssa Dewyer, BS, for “Telemedicine support of cardiac care in Northern Uganda: leveraging hand-held echocardiography and task-shifting”
Graduate students: Natalie Pudalov, BA, “Cortical thickness asymmetries in MRI-abnormal pediatric epilepsy patients: a potential metric for surgery outcome”
High school/undergraduate students: Kia Yoshinaga for “Time to rhythm detection during pediatric cardiac arrest in a pediatric emergency department”
Community-Based Research
Faculty: Adeline (Wei Li) Koay, MBBS, MSc, for “Recent trends in the prevention of mother-to-child transmission (PMTCT) of HIV in the Washington, D.C., metropolitan area”
Staff: Gia M. Badolato, MPH, for “STI screening in an urban ED based on chief complaint”
Post docs/fellows/residents: Christina P. Ho, M.D., for “Pediatric urinary tract infection resistance patterns in the Washington, D.C., metropolitan area”
Graduate students: Noushine Sadeghi, BS, “Racial/ethnic disparities in receipt of sexual health services among adolescent females”
Education, Training and Program Development
Faculty: Cara Lichtenstein, M.D., MPH, for “Using a community bus trip to increase knowledge of health disparities”
Staff: Iana Y. Clarence, MPH, for “TEACHing residents to address child poverty: an innovative multimodal curriculum”
Post docs/fellows/residents: Johanna Kaufman, M.D., for “Inpatient consultation in pediatrics: a learning tool to improve communication”
High school/undergraduate students: Brett E. Pearson for “Analysis of unanticipated problems in CNMC human subjects research studies and implications for process improvement”
Quality and Performance Improvement
Faculty: Vicki Freedenberg, Ph.D., APRN, for “Implementing a mindfulness-based stress reduction curriculum in a congenital heart disease program”
Staff: Caleb Griffith, MPH, for “Assessing the sustainability of point-of-care HIV screening of adolescents in pediatric emergency departments”
Post docs/fellows/residents: Rebecca S. Zee, M.D., Ph.D., for “Implementation of the Accelerated Care of Torsion (ACT) pathway: a quality improvement initiative for testicular torsion”
Graduate students: Alysia Wiener, BS, for “Latency period in image-guided needle bone biopsy in children: a single center experience”


William Davis Gaillard, M.D., has begun his term as President-Elect of the American Epilepsy Society (AES), a medical and scientific society with over 4,000 members. Dr. Gaillard’s term started at the end of the society’s annual meeting in New Orleans, La. in December 2018. Dr. Gaillard will become president of the society in 2020.
Dr. Gaillard, an internationally recognized expert in pediatric epilepsy and imaging, is chief of the divisions of Child Neurology, Epilepsy and Neurophysiology, as well as director of the Comprehensive Pediatric Epilepsy Program at the Children’s National Health System in Washington, D.C. He is also the associate director of the DC-IDDC and director of the Intellectual and Developmental Disabilities Research Center (DC-IDDRC) imaging core and associate director of the Center for Neuroscience Research, Children’s Research Institute. His academic appointments include professor of Pediatrics and Neurology at the George Washington University, professor of Neurology at Georgetown University and professor adjunct of Hearing and Speech Sciences University of Maryland, College Park.
As division chief of Child Neurology, Epilepsy and Neurophysiology, Dr. Gaillard directs a team of pediatric specialists who see thousands of patients each year. Dr. Gaillard has worked throughout his career to care for children and young adults with epilepsy from the onset of seizures through novel therapeutic interventions, medication trials and, when appropriate, surgery. Treatment at Children’s National addresses the full range of the condition, including problems of difficult-to-control epilepsy. Additionally, treatment includes the concurrent social, educational and emotional issues faced by children with the condition and their families.
An active member of AES for more than 25 years, Dr. Gaillard has served as treasurer and as chair of the Clinical Investigator Workshop and Pediatric Content Committees. He is an active participant in mentoring activities, including the Junior Investigators Mentoring program and past co-chair of the AES Research and Training Grant Review Study Section. He also serves as an associate editor for the journal Epilepsy Research.
Children’s National Health System’s Comprehensive Pediatric Epilepsy Program is one of the largest and most experienced multidisciplinary epilepsy programs in the country. With a range of programs specializing in new onset epilepsy, the Ketogenic diet, intractable epilepsy, neuroinflammation, neurogenetics, epilepsy surgery and more. The epilepsy program at Children’s National is continuously working to improve care for patients through clinical innovation, active studies and utilizing the most advanced technologies in epilepsy surgery. Children’s National has one of the best surgical outcomes in the county, aided by advanced structural and functional imaging, minimally invasive techniques, deep brain stimulation, neuronavigation, neurorobotics using the ROSA stereotactic neurosurgical robot and intraoperative MRI.
The Children’s National Health System Center for Neuroscience and Behavioral Medicine is proud to host the 29th Annual Pediatric Neurology Update course.
This year’s course will focus on three critical areas in pediatric neuroscience and neurodevelopment: epilepsy with focuses on innovations in epilepsy surgery and new therapeutics; tuberous sclerosis including neurosurgical advances and transition to adulthood; and autism spectrum disorder with emphasis on new understandings and pre-requisites for an “Autism Friendly Hospital.”
We invite you to join us for presentations from renowned experts in the field in this full-day, CME accredited event on April 11, 2019 at the Bethesda North Marriott Hotel & Conference Center in Rockville, MD.
For more information and to register, visit ChildrensNational.org/NeurologyUpdate.


Chima Oluigbo, M.D., and his team are using Visualase to identify and eliminate seizure foci and provide patients with a minimally invasive procedure for treating epilepsy.
About one in 26 people will be diagnosed with epilepsy in their lifetime. That adds up to about 3.4 million people in the U.S., or about 1 percent of the population nationwide. This condition can have huge consequences on quality of life, affecting whether children will learn well in school, eventually drive a car, hold down a job or even survive into adulthood.
For most of those that develop epilepsy, medications can keep seizures in check. However, for about a third of patients, this strategy doesn’t work, says Chima Oluigbo, M.D., an attending neurosurgeon at Children’s National Health System. That’s when he and his team offer a surgical fix.
Epilepsy surgery has come a long way, Dr. Oluigbo explains. When he first began practicing in the early 2000s, most surgeries were open, he says – they involved making a long incision in the scalp that can span half a foot or more. After drilling out a window of skull that can be as long as five inches, surgeons had to dig through healthy brain to find the abnormal tissue and remove it.
Each part of this “maximally invasive” procedure can be traumatic on a patient, Dr. Oluigbo says. That leads to significant pain after the procedure, extended hospital stays of at least a week followed by a long recovery. There are also significant risks for neurological complications including stroke, weakness, paralysis, speech problems and more.
However, open surgery isn’t the only option for epilepsy surgery anymore. Several new minimally invasive alternatives are now available to patients and the most promising, Dr. Oluigbo says, is called Visualase. He and his team are the only surgeons in the region who perform this procedure.
In Visualase surgeries, Dr. Oluigbo and his colleagues start by making a tiny incision, about 5 millimeters, on the scalp. Through this opening, they bore an even tinier hole into the skull and thread a needle inside that’s about 1.6 millimeters wide. “The brain barely notices that it’s there,” he says.
The tip of this wire holds a laser. Once this tip is placed directly at the seizure foci – the cluster of nerve cells responsible for generating a seizure – the patient is placed in an intraoperative magnetic resonance imaging (MRI) device. There, after checking the tip’s precise placement, the surgeons turn the laser on. Heat from the laser eradicates the foci, which the surgeons can see in real time using MRI thermography technology. The margins of the destroyed tissue are well-defined, largely sparing healthy tissue.
After the wire is removed, the incision is closed with a single stitch, and patients go home the next day. The majority of patients are seizure free, with rates as high as 90 percent for some types of epilepsy, Dr. Oluigbo says. Although seizure-free rates are also high for open procedures, he adds, Visualase spares them many of open surgeries’ painful and difficult consequences.
“Having done both open surgeries and Visualase,” Dr. Oluigbo says, “I can tell you the difference is night and day.”
Although open procedures will still be necessary for some patients with particularly large foci that are close to the surface, Dr. Oluigbo says that Visualase is ideal for treating medication-resistant cases in which the foci are buried deep within the brain. A typical example is a condition called hypothalamic hamartoma, in which tumors on the hypothalamus lead to gelastic seizures, an unusual seizure type characterized by uncontrollable laughing. He also uses Visualase for another condition called tuberous sclerosis, in which waxy growths called tubers develop in the brain, and for cancerous and benign brain tumors.
It’s gratifying to be able to help these children become seizure-free for the rest of their lives, says Dr. Oluigbo – even more so with the numerous updates he receives from families telling him how much this procedure has improved their children’s lifestyle.
“Visualase has completely changed the way that we approach these patients,” Dr. Oluigbo says. “It’s extraordinary to see the effects that this one procedure can have on the quality of life for patients here at Children’s National.”
Example of NeuroPace RNS System placement.
If a child’s refractory seizures – seizures that don’t respond to medication – are originating in a part of the brain that is central to function (for example, impacting memory or verbal skills) the standard next step – surgical resection – is not an option for seizure reduction or relief. In most cases, these children are followed, more medications are tried, and other strategies attempted, but few viable options exist to ease their symptoms.
It’s possible that the next generation of implantable neurostimulators, which act as a type of pacemaker for the brain, might make a difference for some children previously left with no answers. Children’s National neurosurgeon Chima Oluigbo, M.D., in collaboration with the Comprehensive Pediatric Epilepsy Program at Children’s National, is looking at how these devices might be used to reduce or eliminate refractory seizures in pediatric patients. One example of this type of device is the RNS System.
“The RNS has been FDA approved for adults since 2013,” says Dr. Oluigbo, who recently implanted a NeuroPace RNS in the first pediatric patient at Children’s National, and one of the first young patients in the country. “The safety and efficacy data in the adult population, now gathered from a cohort of more than 800 adults, is showing positive outcomes so far. That allows pediatric neurosurgeons to consider an off-label use of this device for patients under the approved usage age of 18, when no other treatments exist.”
The RNS operates differently from previous neuro pacemaker-style devices. It is a “closed-loop” system that doesn’t require external activation once a seizure has started. Instead, the precise location of seizure origination is identified via functional magnetic resonance imaging (fMRI). Leads are then placed at the seizure site via surgery, and once activated, the RNS monitors and self-activates when pre-seizure electrical impulses are detected. The device responds by emitting a series of its own electrical impulses to interrupt and reset the brain’s seizure activity. The RNS system’s ability to continuously monitor the patient also allows physicians to get an inside look at the ongoing brain function of these young patients.
“Children’s National is one of the first places to apply the use of this device in children, because we are one of the few locations on the East coast with the multi-disciplinary expertise to implement it safely and effectively,” says Dr. Oluigbo. “Our clinical epilepsy team has been imaging and treating children with epilepsy for almost 30 years. With one of the oldest neurosurgical programs in country and our technological capabilities, Children’s National becomes the perfect location to explore how technology like this can improve the quality of life for our patients, many of whom have previously been told there is nothing more we can do to help.”
De-personalized data from patients who receive the NeuroPace RNS will be shared with the company in the hopes that the data will assist the FDA in assessing the appropriateness of extending the age range of approval from 18 and above to 12 and above.
“Our hope is to contribute to the body of data about this device and determine if it will improve the lives of our younger patients the way it has already been done for adults,” Dr. Oluigbo concludes. “Kids’ brains may respond differently, however, sharing our patients’ experiences and outcomes will help us identify whether or not this is a viable and promising option for more children with refractory epilepsy.”


As part of Research and Education Week 2018, two Presidential awardees were recognized for their research contributions, Catherine “Katie” Forster, M.D., M.S., and Nathan Anthony Smith, Ph.D.
Catherine “Katie” Forster, M.D., M.S., and Nathan Anthony Smith, Ph.D., received the President’s Award for Innovation in Research honoring their respective research efforts to explore an understudied part of the microbiome and to shed light on an underappreciated player in nerve cell communication.
Drs. Forster and Smith received their awards April 19, 2018, the penultimate day of Research and Education Week 2018, an annual celebration of the excellence in research, education, innovation and scholarship that takes place at Children’s National Health System. This year marks the fifth time the President’s Award honor has been bestowed to Children’s faculty.
Dr. Forster’s work focuses on preventing pediatric urinary tract infections (UTIs). Frequently, children diagnosed with illnesses like spina bifida have difficulty urinating on their own, and they often develop UTIs. These repeated infections are frequently treated with antibiotics which, in turn, can lead to the child developing antibiotic-resistant organisms.
“The majority of the time if you culture these children, you’ll grow something. In a healthy child, that culture would indicate a UTI,” Dr. Forster says. “Children with neurogenic bladder, however, may test positive for bacteria that simply look suspect but are not causing infection. Ultimately, we’re looking for better ways to diagnose UTI at the point of care to better personalize antibiotic treatment and limit prescriptions for children who do not truly need them.”
Powered by new sequencing techniques, a research group that includes Dr. Forster discovered that the human bladder hosts a significant microbiome, a diverse bacterial community unique to the bladder. Dr. Forster’s research will continue to characterize that microbiome to determine how that bacterial community evolves over time and whether those changes are predictable enough to intervene and prevent UTIs.
“Which genes are upregulated in Escherichia coli and the epithelium, and which genes are upregulated by both in response to each other? That can help us understand whether genes being upregulated are pathogenic,” she adds. “It’s a novel and exciting research area with significant public health implications.”
Smith’s work focuses on the role of astrocytes, specialized star-shaped glial cells, in modulating synaptic plasticity via norepinephrine. Conventional thinking describes astrocytes as support cells but, according to Smith, astrocytes are turning out to be more instrumental.
Norepinephrine, a neurotransmitter that plays an essential role in attention and focus, is released by a process known as volume transmission, which is a widespread release of a neurotransmitter at once, says Smith, a principal investigator in Children’s Center for Neuroscience Research. Astrocytes, which outnumber neurons in the brain, are strategically and anatomically located to receive this diffuse input and translate it into action to modulate neural networks.
“We hypothesize that astrocytes are integral, functional partners with norepinephrine in modulating cortical networks,” Smith adds. “Since astrocytes and norepinephrine have been implicated in many central nervous system functions, including learning and attention, it is critical to define mechanistically how astrocytes and norepinephrine work together to influence neural networks. This knowledge also will be important for the development of novel therapeutics to treat diseases such as attention deficit hyperactivity disorder and epilepsy.”
William Davis Gaillard, M.D., has been elected second vice president of the American Epilepsy Society (AES), a medical and scientific society with 4,000 members. Dr. Gaillard’s term started at the end of the society’s annual meeting, December 1-5, in Washington, D.C.
“The AES is the largest multidisciplinary professional and scientific society dedicated to the understanding, treatment and eradication of epilepsy and associated disorders, and I am honored to serve as the new Second Vice President.” Dr. Gaillard said.
Dr. Gaillard, an internationally recognized expert in pediatric epilepsy and imaging, is chief of Neurology, Epilepsy and Neurophysiology at Children’s National. He is also the associate director of the DC-IDDC and director of the of the Intellectual and Developmental Disabilities Research Center (DC-IDDRC) imaging core and associate director of the Center for Neuroscience Research, Children’s Research Institute. His academic appointments include professor of Pediatrics and Neurology at George Washington University and professor of Neurology at Georgetown University.
As division chief of Child Neurology, Epilepsy and Neurophysiology, Dr. Gaillard directs a team of pediatric specialists who see thousands of patients each year. Dr. Gaillard has worked throughout his career to care for children and young adults with epilepsy from the onset of seizures through novel therapeutic interventions, medication trials and, when appropriate, surgery. Treatment at Children’s National addresses the full range of the condition, including problems of difficult-to-control epilepsy. Additionally, treatment includes the concurrent social, educational and emotional issues faced by children with the condition and their families.
An active participant in AES activities, Dr. Gaillard has served as treasurer and as chair of the Clinical Investigator Workshop and Pediatric Content Committees. He also serves as an associate editor for the journal Epilepsy Research, and as a regular reviewer on AES and Epilepsy Foundation study sections. Dr. Gaillard will service as first vice president in 2019 and accede to the presidency of AES in 2020.


A study that includes William D. Gaillard, M.D., among its authors indicates that U.S. doctors appear to have reached an unexpected consensus about which anti-seizure medicine to prescribe to their pediatric patients.
The number of available anti-seizure medications has exploded in the past two decades, going from just a handful of medicines available in the 1990s to more than 20 now. Once the Food and Drug Administration (FDA) approves each new medicine based on trials in adults, it’s available for clinicians to prescribe off-label to all age groups. However, says William D. Gaillard, M.D., division chief of Child Neurology and Epilepsy, Neurophysiology and Critical Care Neurology at Children’s National Health System, trials that lead to FDA approval for adults do not provide any information about which medications are best for children.
“With so many medications and so little data,” Dr. Gaillard says, “one might think doctors would choose a wider variety of medicines when they prescribe to children with epilepsy.”
However, the results from a recent study that included Dr. Gaillard and colleagues, published online in Pediatric Neurology on June 27, 2017, show otherwise. The study indicates that doctors in the United States appear to have reached an unexpected consensus about which medication to prescribe for their pediatric patients.
The study is part of a broader effort to collect data on the youngest epilepsy patients – those younger than 3 years old, the age at which epilepsy most often becomes evident. As part of this endeavor, researchers from 17 U.S. pediatric epilepsy centers enrolled in the study 495 children younger than 36 months old who had been newly diagnosed with non-syndromic epilepsy (a condition not linked to any of the commonly recognized genetic epilepsy syndromes).
The researchers mined these patients’ electronic medical records for information about their demographics, disease and treatments. About half of the study participants were younger than 1 year old when they were diagnosed with epilepsy. About half had disease marked by focal features, meaning that their epilepsy appeared to originate from a particular place in the brain. Nearly all were treated with a single medication, as opposed to a cocktail of multiple medicines.
“This study identifies current practices, but whether those practices are correct is a separate question,” explains Dr. Gaillard. “Just because a medication is used commonly doesn’t mean it is the best medication we should be using.”
Of those treated with a single medication, nearly all were treated with one of five medicines: Levetiracetam, oxcarbazepine, phenobarbital, topiramate and zonisamide. However, the data showed a clear prescribing preference. About 63 percent of the patients were prescribed levetiracetam as a first choice. By contrast, oxcarbazepine and phenobarbital, the next most frequently prescribed medicines, were taken by patients as a first choice by a mere 14 percent and 13 percent respectively.
Even more striking, of the children who were not prescribed levetiracetam initially but required a second medication due to inadequate efficacy or unacceptable side effects, 62 percent also received this medication. That made levetiracetam the first or second choice for about 74 percent of all the children in the study, despite the availability of more than 20 anti-seizure medications.
It’s not clear why levetiracetam is such a frequent choice in the United States, says Dr. Gaillard. However, in its favor, the drug is available in a liquid formulation, causes no ill effects medically and can be started intravenously if necessary. Studies have shown that it appears to be effective in controlling seizures in about 40 percent of infants.
Yet, levetiracetam’s market dominance appears to be a North American phenomenon, the study authors write. A recent international survey that Dr. Gaillard also participated in suggests that outside of this continent, carbazepine and oxcarbazepine were the most frequently prescribed medications to treat focal seizures.
What’s really necessary, Dr. Gaillard says, is real data on efficacy for each of the medications commonly prescribed to pediatric epilepsy patients – a marked vacuum in research that prevents doctors from using evidence-based reasoning when making medication choices.
“This study identifies current practices, but whether those practices are correct is a separate question,” he explains. “Just because a medication is used commonly doesn’t mean it is the best medication we should be using.”
To answer that question, he says, researchers will need to perform a head-to-head clinical trial comparing the top available epilepsy medications in children. This study sets the stage for such a trial by identifying which medications should be included.
“Uncontrolled pediatric epilepsy can have serious consequences, from potential problems in development to a higher risk of death,” Dr. Gaillard says. “You want to use the optimal medicine to treat the disease.”


In the spring of 2017, a multidisciplinary team applied an innovative approach to help preserve function in the working right hemisphere of a baby who experienced her first seizure hours after birth.
When orderly early fetal brain development is disturbed in one half of the brain, infants can be born with hemimegalencephaly—a rare occurrence—that results in one of the brain’s two hemispheres being oversized, heavy and malformed. This brain malformation arises early in the fetal period of life, is not inherited and is associated with seizures early in life.
Children with hemimegalencephaly can develop horrible seizures within the first hours or days of life. According to published research, every month these infants experience uncontrolled seizures correlates to a steep decline in IQ.
Because these types of seizures do not respond to multiple anti-seizure medications—medicines which may also cause worrisome side effects of their own in neonates—care teams attempt to schedule surgery as soon as feasible to remove or disconnect the hemisphere triggering the damaging seizures. “The ‘bad’ brain does not sustain any function and it interferes with the ‘good’ brain doing what it needs to do,” says William D. Gaillard, M.D., chief of Children’s division of Epilepsy and Neurophysiology and chief of Neurology.
Hemispherectomy is intricate surgery on an organ that is softer than normal and crisscrossed with a tangle of blood vessels that supply the damaged hemisphere with blood. Because of the risks of life-threatening blood loss in very young infants, the dramatic surgery is usually not performed until babies are at least 3 months old and weigh at least 10 pounds.
The challenge: The vulnerable babies who most need relief, infants who have been seizing since early life, are too young for the operation.
Neurosurgeons have clamped the carotid artery that supplies blood to the brain to minimize blood loss when the hemisphere is surgically removed. Dr. Gaillard says knowledge of that approach led the team to think: What if we use embolization—blocking blood supply to targeted locations in the brain—to achieve the same effect? The plan effectively destroys the malformed brain from within, neutralizing its ability to cause the seizures.
“It was eye-opening for us to think about actually inflicting brain injury as a way of treating something in the brain that was causing seizures. That is really novel in itself: We’re thinking out of the box in applying existing techniques in a different age group. The conventional thinking with newborns is to let them be; their seizures don’t look that bad,” says Taeun Chang, M.D., director of Children’s Neonatal Neurology and Neonatal Neurocritical Care Program.
“We have evidence to suggest this is a safe and effective way of avoiding recurrent seizures and minimizing the need to give these infants potentially toxic medications so early in life. Ultimately, this helps a select group of babies who need the surgery to get to the point of being old enough to have it—all the while, sparing the healthy part of their brain,” Dr. Gaillard adds.

Once the embolization ended Darcy’s most severe seizures, the little girl could make eye contact, started smiling, and then graduated from smiling to full laughs. In weekly physical therapy, the infant works on tummy time, head control and ensuring her eyes track.
In the spring of 2017, the multidisciplinary team applied the innovative approach to help preserve function in the working right hemisphere of a baby named Darcy Murphy. Darcy experienced her first seizure hours after she was born, and when she arrived at Children’s National had been in and out of two different emergency rooms in another state for the first few weeks of her life.
The team explained to the Murphy family that Darcy was on multiple medications, but her seizures continued unabated. The options included inducing a coma, sending Darcy home despite ongoing seizures or minimally invasive embolization.
“We would not have even posed this if we were not confident in our ability to do the procedure and deal with potential complications,” Dr. Chang says.
“Oh my gosh, as a parent you know what you’re doing is permanent,” says Rachel Murphy, 29, Darcy’s mom said of the decisions that she and husband Ryan, 33, faced for the youngest of their three children. “What if it’s not the right decision? What if in a week they come out with a new procedure you could have done? We were horrified all the time. The nice part with this procedure is the reward is apparent very quickly, and it just gets better. You don’t have to wait two years to know you made the right decision. You can see half a brain is better than the whole thing for this specific child.”
Once the embolization ended Darcy’s most severe seizures, the little girl could initiate and maintain eye contact with family members, started smiling and then graduated from smiling to full laughs. In weekly physical therapy, the infant works on tummy time, head control and ensuring her eyes track.
Children’s multidisciplinary care team includes experts in newborn intensive care (neonatologists) to aggressively manage seizures in the traditional fashion as they occur and to monitor vital signs; a neonatal neurologist/neurointensivist at the bedside and in the Angio suite monitoring Darcy’s brain activity; a neonatal epileptologist; a surgical epilepsy team; an interventional neuroradiologist; neurosurgeons to perform the delicate functional hemispherectomy to remove any residual brain tissue from the bad hemisphere; and physical therapists working to help Darcy achieve maximum function after surgery.
“We were just like one unit in the sense of being able to provide coherent, comprehensive care. It’s about blood pressure management, breathing, electrolytes, making sure everything is right for going to the operating room,” Dr. Chang explains. “Darcy’s case highlights the ways in which Children’s National is different and offers personalized care that is superior to other centers.”
The team, which recently published a case report of two previous serial embolizations followed by hemispherectomy, plans follow-up papers describing EEG manifestations during an acute stroke in a newborn, advice to the field on best practices for the embolization and using cooling to control the planned brain injury during embolization hemispherectomy.
Revised Nov. 7, 2017

 A multidisciplinary team led by Chima Oluigbo, M.D., F.R.C.S.C., pioneered a novel technique to preserve newborns’ healthy brain tissue, buying time until the infants became old enough to undergo a hemispherectomy. What’s knownHemimegalencephaly is an extremely rare birth defect in which one side of the brain grows larger than the other. This anomaly typically leads to severe, recurrent seizures that can be difficult to control solely with medications. While the seizures themselves are detrimental to the developing brain, the amount of medications used to reduce seizure frequency often come with significant side effects and have the potential to hamper brain growth. Hemispherectomy, a radical surgery in which one half of the brain is removed, is often the most successful way to treat severe and intractable epilepsy. However, this surgery can be challenging to perform successfully in very young babies. What’s newIn this case report, the Children’s National Health System Epilepsy Team led by Chima Oluigbo, M.D., F.R.C.S.C., a pediatric neurosurgeon; Tammy N. Tsuchida, M.D., PhD., a pediatric surgical epileptologist; Monica Pearl, M.D., a pediatric interventional neuroradiologist; Taeun Chang, M.D., a neonatal neurointensivist; and the neonatal intensive care team explored the possibility of using minimally invasive surgery to cut off the blood supply to the brain hemisphere responsible for generating seizures in newborns with hemimegalencephaly. This procedure, they reasoned, could buy time for babies to mature and become more resilient to withstand the future hemispherectomy while also lessening the damage caused by uncontrolled, recurrent seizures. The case report focused on the first two patients with hemimegalencephaly who had sequential procedures to gradually restrict blood flow to the affected brain hemisphere within their first few weeks of life, followed by hemispherectomies at a few months of age. This novel approach significantly lessened their seizures until hemispherectomy, allowing these children to continue to grow and develop seizure-free. Questions for future researchQ: Which patients are best suited for this surgical procedure? Source: “ ‘Endovascular embolic hemispherectomy’: A strategy for the initial management of catastrophic holohemispheric epilepsy in the neonate.” Oluigbo, C., M.S. Pearl, T.N. Tsuchida, T. Chang, C.-Y. Ho and W. D. Gaillard. Published by Child’s Nervous System October 29, 2016.
|