




Catherine Limperopoulos, Ph.D., was drawn to understanding the developing brain, examining how early adverse environments for a mother can impact the baby at birth and extend throughout its entire lifetime. She has widened her lens – and expanded her team – to create the new Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital.
“Despite the obvious connection between mothers and babies, we know that conventional medicine often addresses the two beings separately. We want to change that,” said Dr. Limperopoulos, who also directs the Developing Brain Institute. “Given the current trajectory of medicine toward precision care and advanced imaging, we thought this was the right moment to channel our talent and resources into understanding this delicate and highly dynamic relationship.”
Since its establishment in July 2023, the new research center has gained recognition through high-impact scientific publications, featuring noteworthy studies exploring the early phases of human development.
Dr. Limperopoulos has been at the forefront of groundbreaking research, directing attention to the consequences of maternal stress on the unborn baby and the placenta. In addition, under the guidance of Kevin Cook, Ph.D., investigators published a pivotal study on the correlation between pain experienced by premature infants in the Neonatal Intensive Care Unit and the associated risks of autism and developmental delays.
Another area of research has focused on understanding the impact of congenital heart disease (CHD) on prenatal brain development, given the altered blood flow to the brain caused by these conditions during this period of rapid development. Led by Josepheen De Asis-Cruz, M.D., Ph.D., a research team uncovered variations in the functional connectivity of the brains of infants with CHD. In parallel, Nickie Andescavage, M.D., and her team employed advanced imaging techniques to identify potential biomarkers in infants with CHD, holding promise for guiding improved diagnostics and postnatal care. Separately, she is investigating the impact of COVID-19 on fetal brain development.
In the months ahead, the team plans to concentrate its efforts on these areas and several others, including the impact of infectious disease, social determinants of health and protecting developing brains from the negative impacts of maternal stress, pre-eclampsia and other conditions prevalent among expectant mothers.
Given its robust research plan and opportunities for collaboration, the center pulled together expertise from across the hospital’s faculty and has attracted new talent from across the country, including several prominent faculty members:
The new center brings together award-winning talent. This includes Yao Wu, Ph.D., who recently earned the American Heart Association’s Outstanding Research in Pediatric Cardiology award for her groundbreaking work in CHD, particularly for her research on the role of altered placental function and neurodevelopmental outcomes in toddlers with CHD. Dr. Wu became the third Children’s National faculty member to earn the distinction, joining an honor roll that includes Dr. Limperopoulos and David Wessel, M.D., executive vice president and chief medical officer.
Interim Chief Academic Officer Catherine Bollard, M.D., M.B.Ch.B., said the cross-disciplinary collaboration now underway at the new center has the potential to make a dramatic impact on the field of neonatology and early child development. “This group epitomizes the Team Science approach that we work tirelessly to foster at Children’s National,” Dr. Bollard said. “Given their energetic start, we know these scientists and physicians are poised to tackle some of the toughest questions in maternal-fetal medicine and beyond, which will improve outcomes for our most fragile patients.”

Extensive research has shown that children with congenital heart disease (CHD) who are born blue or who need cardiac surgery in their first year of life are at risk for developmental challenges and/or learning difficulties.
Mary Donofrio, M.D., co-director of the Cardiac Neurodevelopment Outcome (CANDO) program at Children’s National Hospital, says that we started the program — the only one of its kind in the Washington, D.C. region — to identify and manage delays in development and difficulties with learning, no matter when they arise.
“We start paying attention even before birth and then continue to evaluate neurodevelopment at key stages in a kid’s life to assure the best outcome. Our goal is for every kid born with CHD to be able to achieve their full potential, be active, make friends and succeed in school. Most important, we want each of our patients to grow up to be a happy and successful adult,” says Dr. Donofrio.
Learn more about CANDO at Children’s National Hospital and our role in developing best practices for neurodevelopmental and psychosocial services as part of the international multi-specialty Cardiac Neurodevelopmental Outcome Collaborative.


The review summarizes both the known physiological roles of caspases as well as some of the well-characterized neurotoxic effects of anesthetics in pre-clinical models.
A review article in the journal Cell Press: Trends in Neuroscience outlines the wide variety of cellular signaling roles for caspase proteins — a type of cellular enzyme best known for its documented role in the natural process of cell death (apoptosis). The authors, including Nemanja Saric, Ph.D., Kazue Hashimoto-Torii, Ph.D., and Nobuyuki Ishibashi, M.D., all from Children’s National Research Institute, pay particular attention to what the scientific literature shows about caspases’ non-apoptotic roles in the neurons specifically. They also highlight research showing how, when activated during a cardiac surgery with anesthesia and cardiopulmonary bypass, these enzymes may contribute to the degeneration of brain cells seen in young children who undergo heart surgery for critical congenital heart defects (CHDs).
The review summarizes both the known physiological roles of caspases as well as some of the well-characterized neurotoxic effects of anesthetics in pre-clinical models.
The authors propose that these non-apoptotic activities of caspases may be behind some of the adverse effects on the developing brain related to cardiac surgery and anesthesia. Those adverse effects are known to increase risk of behavioral impairments in children with congenital heart disease who underwent cardiac surgery with both anesthesia and cardiopulmonary bypass at a very young age.
This work is the first to propose a possible link between developmental anesthesia neurotoxicity and caspase-dependent cellular responses.
Better understanding of the time and dose-dependent effects of general anesthetics on the developing brain, particularly in children who have genetic predispositions to conditions such as CHDs, will help researchers understand their role (if any) in behavioral problems often encountered by these patients after surgery.
If found to be a contributing factor, perhaps new therapies to mitigate this caspase activity might be explored to alleviate some of these adverse effects on the developing brain.
The authors hope to stimulate more in-depth research into caspase signaling events, particularly related to how these signaling events change when an anesthetic is introduced. Deeper understanding of how anesthetics impact caspase activation in the developing brain will allow for better assessments of the risk for children who need major surgery early in life.
Children’s National Hospital leads studies funded by the U.S. Department of Defense to better understand how these other roles of caspases, which until now have not been well-documented, may contribute to brain cell degeneration when activated by prolonged anesthesia and cardiopulmonary bypass during cardiac surgery for congenital heart disease.
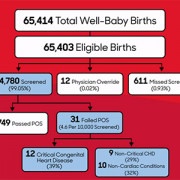
One of the nation’s longest-running newborn screening programs for critical congenital heart disease (CCHD) finds that screening continues to serve as a necessary tool to help identify every child with CCHD — even in states where the majority of babies are diagnosed before birth.
The screening program study findings were published in Pediatrics. The data is some of the first to provide long-term evidence for using pulse oximetry to screen newborns for critical congenital heart disease 24 hours after birth. This screening test was added to the Department of Health and Human Services Recommended Uniform Screening Panel in 2011 and is now required in all 50 states.
“This study reinforces why pulse oximetry screening for CCHD is an important tool in our arsenal to identify and treat critical congenital heart disease, and other conditions that affect the flow of oxygen throughout the body, as soon as possible,” says Bryanna Schwarz, M.D., a cardiology fellow at Children’s National Hospital and lead author. “We know that prompt, early detection and swift intervention is crucial to positive long-term outcomes for these kids.”
The team looked at the data and outcomes for all babies born throughout eight years at Holy Cross Hospital in suburban Maryland, one of the first community birthing hospitals in the country to routinely perform the screening. Over the eight-year period, 64,780 newborns were screened at the site. Of those:
The authors note that the 12 newborns with CCHD identified through pulse oximetry screening are noteworthy because they represent critical congenital heart disease cases that are not found before birth in the state of Maryland, where rates of prenatal diagnosis are relatively high. The finding indicates that screening after birth continues to play a critical role in ensuring every baby with critical congenital heart disease is identified and treated as quickly as possible.
“Holy Cross Health and Children’s National have had a decades-long relationship, as we mutually care for women and infants throughout the region. With Children’s National having the U.S. News & World Report #1 ranking Neonatology service in the nation and Holy Cross Hospital being among the top 10 hospitals for the number of babies delivered each year, we are honored to be leading together the great work that is being done to serve our health care community,” says Ann Burke, M.D., vice president of Medical Affairs at Holy Cross Hospital. “We are committed to continuing to do our part to care for women and infants, as well as contribute to the national landscape for neonatal care. We are delighted in the outcomes we have seen and look forward to continued advancement.”
In this study, infants who did not have critical congenital heart disease were considered “false positives” for CCHD. Still, every one of them was found to have another underlying condition, including non-critical congenital heart disease or non-cardiac conditions (such as sepsis and pneumonia) that would also require monitoring and treatment.
The researchers also ran a projection of recently recommended updates to the screening protocol, which include removing a second re-screen after a newborn fails the initial test, to look at whether removing the second rescreen to verify results would decrease accuracy. While the false positive rate did increase slightly from .03% to .04%, eliminating a second re-screen allowed the newborns who were identified to receive crucial care sooner without having to wait an additional hour for one more test to verify their condition.
“It’s time to stop asking if pulse oximetry is a necessary tool to detect critical heart disease in babies,” says Gerard Martin, M.D., M.A.C.C., senior author of the study and C.R. Beyda Professor of Cardiology at Children’s National Hospital. “Our focus now should be on making evidence-based refinements to the screening protocol based on collected data to ensure the process is simple, can be performed consistently and provides as accurate results as possible.”
While the last decade brought great advances in technologies that improve the care of adult arrhythmias, pediatric patients have been left behind, with only five devices approved for use in children in the same period.
Congenital heart disease (CHD) affects six out of 1,000 babies born in the U.S. each year and is often complicated by arrhythmias, a condition where the heart beats too rapidly, too slowly or irregularly due to a misfiring of the body’s electrical impulses. While the last decade brought great advances in technologies that improve the care of adult arrhythmias, pediatric patients have been left behind, with only five devices approved for use in children in the same period. As a result, pediatric specialists are often using off-label or improvised devices to treat pediatric arrhythmias, including the smallest newborns.
Recognizing this unmet need, the National Capital Consortium for Pediatric Device Innovation (NCC-PDI), in collaboration with MedTech Innovator, is accepting applications through April 12, 2021, for its annual “Make Your Medical Device Pitch for Kids!” competition. This year’s competition focuses on innovations in pediatric devices that treat CHD, with an emphasis on electrophysiology devices such as pacemaker systems, ablation catheters, wearable monitoring devices and related technologies that address arrhythmias in children.
“NCC-PDI was created, with the support of the Food and Drug Administration (FDA), to seek out and address significant unmet needs in pediatric medical devices,” says Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “We have learned from the experts that pediatric-specific technologies for treating arrhythmias would be a game changer in the care of their patients, so we are focusing our competition and grant awards on this opportunity.”

“We have learned from the experts that pediatric-specific technologies for treating arrhythmias would be a game changer in the care of their patients, so we are focusing our competition and grant awards on this opportunity,” says Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI.
Using a virtual format, semi-finalists chosen from all submissions will make their first pitch on May 12, 2021. Up to 10 finalists selected from this event earn participation in a special pediatric-focused track of the MedTech Innovator accelerator program, the largest medtech accelerator in the world, beginning in June 2021. These innovators then participate in the pediatric competition finals in September 2021 where judges will award up to $150,000 in FDA-sponsored grants to the devices selected as most impactful and commercially viable.
How significant is the need for pediatric devices to address arrhythmias? In a recent survey of members conducted by the Pediatric and Congenital Electrophysiology Society (PACES), the vast majority (96%) said they believe there is a deficiency in devices available to serve the needs of pediatric patients. Conducted with the U.S.FDA, the survey also asked respondents to identify the biggest unmet need, which physicians identified as cardiovascular implantable electronic devices that are smaller, have better battery life and have pediatric-specific algorithms. Specifically, a leadless pacemaker designed for pediatric care was consistently on the most-wanted list.
NCC-PDI is one of five members in the FDA’s Pediatric Device Consortia Grant Program created to support the development and commercialization of medical devices for children, which lags significantly behind the advancement of adult medical devices. NCC-PDI is led by the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland with support from partners MedTech Innovator, BioHealth Innovation and design firm Archimedic.
Eskandanian says that enhancing access to resources for pediatric innovators is also one of the aims of the Children’s National Research & Innovation Campus, a first-of-its-kind focused on pediatric health care innovation, with the first phase currently open on the former Walter Reed Army Medical Center campus in Washington, D.C. With its proximity to federal research institutions and agencies, universities, academic research centers, as well as on-site incubator Johnson and Johnson Innovation – JLABS, the campus provides a rich ecosystem of public and private partners which, like the NCC-PDI network, will help bolster pediatric innovation and commercialization.


Every year, nearly 40,000 babies are born with a congenital heart defect (CHD) — the leading cause of birth defect-associated infant illness and death.
Every year, nearly 40,000 babies are born with a congenital heart defect (CHD) — the leading cause of birth defect-associated infant illness and death. An event that may contribute to cyanotic CHD is the lack of oxygen, known as hypoxia, before and after birth, impacting gene expression and cardiac function that delay postnatal cardiac maturation, according to a new pre-clinical model led by researchers at Children’s National Hospital.
Single ventricle, transposition of the great arteries, truncus arteriosus and severe forms of tetralogy of Fallot, such cyanotic congenital heart diseases have lower circulating blood oxygen levels. The lack of oxygen in the blood begins prenatally and continues after birth until definitive repair, suggesting a delay on cardiac maturation.
There is little research on the underpinnings that explain the lack of oxygen’s effects on the developing heart, which could help inform adequate therapies in the pediatric population to promote cardiovascular health across the lifetime. The researchers developed the first pre-clinical model that explores the effects of chronic hypoxia in perinatal and postnatal stages on the developing heart under conditions seen in cyanotic CHD.
“To the best of our knowledge, ours is the first study to perform complete gene expression arrays on animals after perinatal hypoxia,” said Jennifer Romanowicz, senior noninvasive imaging fellow at Boston Children’s Hospital and lead author of the study. “Not only did these studies allow us to determine the effects of hypoxia on heart development, but the detailed results of our study will be available to other researchers to independently address other questions about perinatal hypoxia and heart development.”
The study published in the American Journal of Physiology: Heart and Circulatory Physiology suggests that chronic lack of oxygen alters the electrical properties of heart tissue, called the electrophysiological substrate, and the contractile apparatus, a muscle composed of proteins that control cardiac contraction. Multiple genes involved with the contractile apparatus were expressed differently in the non-human subjects.
“What was remarkable was that most abnormalities normalized after the animals recovered in normal oxygen levels,” said Romanowicz. “This is an optimistic sign that early repair of cyanotic congenital heart disease may allow the heart to finish development.”
The researchers placed pregnant non-human subjects in hypoxic chambers starting on embryonic day 16, mimicking the second trimester in humans. The same subjects gave birth in the hypoxic chambers, and the newborns were kept there until postnatal day eight when the heart muscle maturation is nearly complete. To understand how human infants recover with normalized oxygen levels after surgical repair of cyanotic CHD, the researchers moved hypoxic subjects to normal oxygen conditions for recovery and tested again at postnatal day 30.
“Next steps include using a pre-clinical model of cyanotic congenital heart disease that more accurately represents human neonatal physiology,” said Devon Guerrelli, Ph.D. candidate at Children’s National. We plan to work with the cardiac surgery team at Children’s National to investigate changes in the myocardium due to hypoxia in pediatric patients who are undergoing surgical repair.”
Nikki Posnack, Ph.D., principal investigator at Sheikh Zayed Institute for Pediatric Surgical Innovation and Nobuyuki Ishibashi, M.D., director of Cardiac Surgery Research Laboratory at Children’s National, led and guided the team of researchers involved in the study.


Gerard Martin, M.D., F.A.C.C., has been awarded the 2021 Master of the ACC Award by the American College of Cardiology in honor of contributions to the cardiovascular profession.
Gerard Martin, M.D., F.A.C.C., has been awarded the 2021 Master of the ACC Award by the American College of Cardiology in honor of contributions to the cardiovascular profession. Dr. Martin will be recognized for these achievements along with all 2021 Distinguished Award winners during Convocation at the hybrid 70th Annual Scientific Session & Expo taking place May 15-17, 2021 in Atlanta and virtually.
“Dr. Martin has made lasting contributions to the field of cardiovascular medicine through his dedication to improving cardiovascular health and enhancing patient care,” said ACC President Athena Poppas, MD, F.A.C.C. “It is an honor to be able to recognize Dr. Martin with the Master of the ACC Award and celebrate his tremendous achievements in the cardiovascular field.”
The Master of the ACC (MACC) Award recognizes and honors fellows of the American College of Cardiology who have consistently contributed to the goals and programs of the college and who have provided leadership in important college activities. MACC designees have been members of the college for at least 15 years and have served with distinction and provided leadership on various college programs and committees. Only four distinguished members of the American College of Cardiology are selected for this honor each year.
Dr. Martin is a cardiologist at Children’s National Hospital, where he has been in practice since 1986. He founded the Children’s National Heart Institute in 2004 and was named the C. Richard Beyda Professor of Cardiology in 2007. He has published over 150 peer-reviewed manuscripts, book chapters and invited publications and has presented abstracts at over 125 meetings. Dr. Martin is an invited lecturer who has traveled to over 200 meetings, hospitals and universities within the U.S. and around the world.
Dr. Martin is an advocate for congenital heart disease (CHD) efforts nationally and internationally. He played integral roles in the development and dissemination of critical congenital heart disease screening in using pulse oximetry — a practice that is now standard for all newborns across the United States. He also has volunteered on countless medical missions to developing countries.
Dr. Martin is board-certified in pediatric cardiology, a fellow of the American Academy of Pediatrics and the American College of Cardiology and is also a member of the Society for Pediatric Research and the American Board of Pediatrics.
Nineteen Distinguished Awards will be presented at ACC.21 this year, each recognizing an individual who has made outstanding contributions to the field of cardiovascular medicine. Recipients are nominated by their peers and then selected by the American College of Cardiology Awards Committee.
The American College of Cardiology envisions a world where innovation and knowledge optimize cardiovascular care and outcomes. As the professional home for the entire cardiovascular care team, the mission of the College and its 54,000 members is to transform cardiovascular care and to improve heart health. The ACC bestows credentials upon cardiovascular professionals who meet stringent qualifications and leads in the formation of health policy, standards and guidelines. The College also provides professional medical education, disseminates cardiovascular research through its world-renowned JACC Journals, operates national registries to measure and improve care, and offers cardiovascular accreditation to hospitals and institutions. For more, visit acc.org.
A novel phase 1 trial looking at how best to optimize brain development of babies with congenital heart disease (CHD) is currently underway at Children’s National Hospital.
Children with CHD sometimes demonstrate delay in the development of cognitive and motor skills. This can be a result of multiple factors including altered prenatal oxygen delivery, brain blood flow and genetic factors associated with surgery including exposure to cardiopulmonary bypass, also known as the heart lung machine.
This phase 1 trial is the first to deliver mesenchymal stromal cells from bone marrow manufactured in a lab (BM-MSC) into infants already undergoing cardiac surgery via cardiopulmonary bypass. The hypothesis is that by directly infusing the MSCs into the blood flow to the brain, more MSCs quickly and efficiently reach the subventricular zone and other areas of the brain that are prone to inflammation. The trial is open to eligible patients ages newborn to six months of age.
Learn more in this overview video.
The trial is part of a $2.5 million, three-year grant from the National Institutes of Health (NIH) led by Richard Jonas, M.D., Catherine Bollard, M.B.Ch.B., M.D., and Nobuyuki Ishibashi, M.D.. The project involves collaboration between the Prenatal Cardiology program of Children’s National Heart Institute, the Center for Cancer and Immunology Research, the Center for Neuroscience Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
“NIH supported studies in our laboratory have shown that MSC therapy may be extremely helpful in improving brain development in animal models after cardiac surgery,” says Dr. Ishibashi. “MSC infusion can help reduce inflammation including prolonged microglia activation that can occur during surgery that involves the heart lung machine.”
Staff from the Cellular Therapy Laboratory, led by director Patrick Hanley, Ph.D., manufactured the BM-MSC at the Center for Cancer and Immunology Research, led by Dr. Bollard.
The phase 1 safety study will set the stage for a phase 2 effectiveness trial of this highly innovative MSC treatment aimed at reducing brain damage, minimizing neurodevelopmental disabilities and improving the postoperative course in children with CHD. The resulting improvement in developmental outcome and lessened behavioral impairment will be of enormous benefit to individuals with CHD.
For more information about this new treatment, contact the clinical research team: Gil Wernovsky, M.D., Shriprasad Deshpande, M.D., Maria Fortiz.
The International Consortium for Health Outcomes Measurement (ICHOM) announced the release of a Congenital Heart Disease Standard Set (CHDSS) in late April 2020.
Gerard Martin, M.D., FAAP, FACC, FAHA, cardiologist at Children’s National Hospital, chaired the working group and contributed to the standards’ writing. In ICHOM‘s press release, he noted that, “Having a global set of outcomes that matters most to adult patients and parents of children with congenital heart disease will provide a road map for healthcare professionals and organizations engaged in setting care strategies for this population around the world. I would like to acknowledge the efforts of the Working Group and ICHOM staff for their incredible effort on this project.”
The CHDSS is a minimum core set of standards, comprised of Patient, Parent, and Clinician – Reported Outcome Measures already being collected by most practices in routine clinical care. The CHDSS measures 14 outcomes under the ICHOM framework for comprehensive outcomes measurement. These overarching domains are Overall Health, Social Health, Mental Health, and Physical Health.
Learn more about the CDHSS, the contributors and read the ICHOM press release.

The CHDSS measures 14 outcomes under the ICHOM overarching domains of Overall Health, Social Health, Mental Health, and Physical Health.

Even though mortality from congenital heart disease (CHD) has declined over the last three decades as diagnosis and treatments have advanced, the chances for a child to survive a CHD diagnosis significantly differs based on the country where he or she is born.
This eye-opening finding is drawn from the first comprehensive study of congenital heart disease across 195 countries, prepared using data from the Global Burden of Diseases, Injuries and Risk Factors Study 2017 (GBD), and recently published in The Lancet.
“Previous congenital heart estimates came from few data sources, were geographically narrow and did not evaluate CHD throughout the life course,” write the authors, known collectively as the 2017 GBD Congenital Heart Disease Collaborators. Co-lead author Meghan D. Zimmerman, M.D., worked on the study while completing her pediatric cardiology and American Heart Association Global Health Fellowships at Children’s National Hospital, and two pediatric cardiologists from Children’s National, Cardiology Associate Chief Craig Sable, M.D., and Gerard Martin, M.D., medical director of Global Services, provided leadership and oversight of this paper. The remaining collaborators are from more than 45 institutions around the world, spanning cardiology, public health and schools of medicine on every continent.
This is the first time the GBD study data was used along with all available data sources and previous publications – making it the most comprehensive study on congenital heart disease burden to date. Key differences between this study and prior estimates include:
This more comprehensive data set led to findings that showed lower predicted long-term survival, higher remission, and lower prevalence than previous studies that extrapolated evidence from studies of high-income countries. However, it also means these new estimates are a more accurate representation of the current global state of affairs. Overall, the study found:
“In high income countries like the United States, we diagnose some heart conditions prenatally during the 20-week ultrasound,” says Gerard Martin, M.D., a pediatric cardiologist at Children’s National Hospital who contributed to the study. “We catch others right after birth with a pulse oximetry screening for critical congenital heart disease. We can operate to correct a critical issue within the first week of life. And now our CHD kids are growing and thriving through adulthood and having families of their own.”
“For children born in middle- and low-income countries, these data draw stark attention to what we as cardiologists already knew from our own work in these countries – the lack of diagnostic and treatment tools leads to lower survival rates for children born with CHD,” adds Craig Sable, M.D., associate chief of cardiology at Children’s National, another primary contributor. “This is one of the most significant publications I have been a part of as it highlights the substantial loss of life to CHD in infancy around the globe.”
The authors write, “The UN has prioritized reduction of premature deaths from heart disease, but to meet the target of ‘ending preventable deaths of newborns and children under 5 years of age,’ health policy makers will need to develop specific accountability measures that address barriers and improve access to care and treatment.”
The study also includes a 400-page appendix breaking down each area by type of congenital anomaly, world region and country.


“We were alarmed by the high percentage of pregnant women with a diagnosis of a major fetal heart problem who tested positive for stress, anxiety and depression,” says Catherine Limperopoulos, Ph.D., director of the Center for the Developing Brain at Children’s National and the study’s corresponding author.
When a diagnosis of fetal congenital heart disease causes pregnant moms to test positive for stress, anxiety and depression, powerful imaging can detect impaired development in key fetal brain regions, according to Children’s National Hospital research published online Jan. 13, 2020, in JAMA Pediatrics.
While additional research is needed, the Children’s National study authors say their unprecedented findings underscore the need for universal screening for psychological distress as a routine part of prenatal care and taking other steps to support stressed-out pregnant women and safeguard their newborns’ developing brains.
“We were alarmed by the high percentage of pregnant women with a diagnosis of a major fetal heart problem who tested positive for stress, anxiety and depression,” says Catherine Limperopoulos, Ph.D., director of the Center for the Developing Brain at Children’s National and the study’s corresponding author. “Equally concerning is how prevalent psychological distress is among pregnant women generally. We report for the first time that this challenging prenatal environment impairs regions of the fetal brain that play a major role in learning, memory, coordination, and social and behavioral development, making it all the more important for us to identify these women early during pregnancy to intervene,” Limperopoulos adds.
Congenital heart disease (CHD), structural problems with the heart, is the most common birth defect. Still, it remains unclear how exposure to maternal stress impacts brain development in fetuses with CHD.
The multidisciplinary study team enrolled 48 women whose unborn fetuses had been diagnosed with CHD and 92 healthy women with uncomplicated pregnancies. Using validated screening tools, they found:
All told, they performed 223 fetal magnetic resonance imaging sessions for these 140 fetuses between 21 and 40 weeks of gestation. They measured brain volume in cubic centimeters for the total brain as well as volumetric measurements for key regions such as the cerebrum, cerebellum, brainstem, and left and right hippocampus.
Maternal stress and anxiety in the second trimester were associated with smaller left hippocampi and smaller cerebellums only in pregnancies affected by fetal CHD. What’s more, specific regions — the hippocampus head and body and the left cerebellar lobe – were more susceptible to stunted growth. The hippocampus is key to memory and learning, while the cerebellum controls motor coordination and plays a role in social and behavioral development.
The hippocampus is a brain structure that is known to be very sensitive to stress. The timing of the CHD diagnosis may have occurred at a particularly vulnerable time for the developing fetal cerebellum, which grows faster than any other brain structure in the second half of gestation, particularly in the third trimester.
“None of these women had been screened for prenatal depression or anxiety. None of them were taking medications. And none of them had received mental health interventions. In the group of women contending with fetal CHD, 81% had attended college and 75% had professional educations, so this does not appear to be an issue of insufficient resources,” Limperopoulos adds. “It’s critical that we routinely to do these screenings and provide pregnant women with access to interventions to lower their stress levels. Working with our community partners, Children’s National is doing just that to help reduce toxic prenatal stress for both the health of the mother and for the future newborns. We hope this becomes standard practice elsewhere.”
Adds Yao Wu, Ph.D., a research associate working with Limperopoulos at Children’s National and the study’s lead author: “Our next goal is exploring effective prenatal cognitive behavioral interventions to reduce psychological distress felt by pregnant women and improve neurodevelopment in babies with CHD.”
In addition to Limperopoulos and Wu , Children’s National study co-authors include Kushal Kapse, MS, staff engineer; Marni Jacobs, Ph.D., biostatistician; Nickie Niforatos-Andescavage, M.D., neonatologist; Mary T. Donofrio, M.D., director, Fetal Heart Program; Anita Krishnan, M.D., associate director, echocardiography; Gilbert Vezina, M.D., director, Neuroradiology Program; David Wessel, M.D., Executive Vice President and Chief Medical Officer; and Adré J. du Plessis, M.B.Ch.B., director, Fetal Medicine Institute. Jessica Lynn Quistorff, MPH, Catherine Lopez, MS, and Kathryn Lee Bannantine, BSN, assisted with subject recruitment and study coordination.
Financial support for the research described in this post was provided by the National Institutes of Health under grant No. R01 HL116585-01 and the Thrasher Research Fund under Early Career award No. 14764.
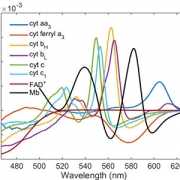
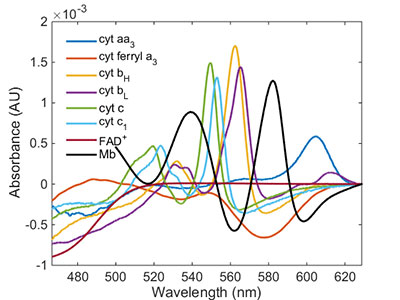
Rafael Jaimes, Ph.D., created an algorithm that is being tested in a pre-clinical model to characterize the light absorbance spectrum from different heart regions using a spectrometer.
After intense cardiac surgery, sometimes a patient’s heart is unable to effectively deliver oxygenated blood and nutrients throughout the recovering body. Known as inadequate or low cardiac output, the condition occurs in about a quarter of patients following surgery with cardiopulmonary bypass, including young children who require complex procedures to correct congenital heart defects at Children’s National Health System.
Researchers at the Sheikh Zayed Institute for Pediatric Surgical Innovation are exploring several facets of this challenge, with the goal of better understanding post-operative recovery trajectories in pediatric patients. Rafael Jaimes, Ph.D., a staff scientist at the institute, leads this work to identify when and how low cardiac output occurs, pinpoint the physical hallmarks of this condition and use that information to prevent long term damage and complications after surgery, including cardiac arrest.
“More research needs to be done to understand the cause of this overarching and multi-faceted syndrome,” says Dr. Jaimes. “I’m interested in understanding how metabolic insufficiency contributes to this condition, and also exploring how we can use current imaging and diagnostic tools to measure, track and treat the insufficiencies that contribute to low cardiac output.”
Tracking inadequate oxygen and nutrient delivery to the parts of the heart that have been repaired is one avenue under exploration. Currently, a cardiac-specific real-time device to measure the oxygen state of the heart, while a patient is in post-operative critical care, is under development.
The heart’s complexity has made using current oxygen measurement devices, such as spectrometers, very difficult. To date no tool exists that effectively screens out artifacts and noise to allow clear visualization. However, during his post-doctoral work, Dr. Jaimes has created a new algorithm that may be the first of its kind to accomplish this feat.
This work on low cardiac output recently received a Congenital Heart Defect Research Award, which is a collaborative program of the Children’s Heart Foundation and the American Heart Association that supports innovative research, seeking to understand and treat congenital heart defects.
A new research study will build on his previous studies by using the algorithm to characterize the absorbance spectrum from different heart regions in a pre-clinical model. The data collected will serve as the baseline for development of a prototype spectrometer software, capable of tracking changes in heart oxygenation before, during and after surgery.
The end goal is to more effectively identify when parts of the heart are deprived of oxygen and nutrients and prevent resulting impacts on cardiac metabolism and output. Doing so will decrease short term mortality and morbidity and may also improve circulation systemically, potentially reducing long term health impacts of reduced oxygenation, such as neurodevelopmental disorders.


Children’s National Health System researchers Richard Jonas, M.D., Catherine Bollard, M.B.Ch.B., M.D., and Nobuyuki Ishibashi, M.D., have been awarded a $2.5 million, three-year grant from the National Institutes of Health (NIH) to conduct a single-center clinical trial at Children’s National. The study will involve collaboration between the Children’s National Heart Institute, the Center for Cancer and Immunology Research, the Center for Neuroscience Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
The goal of the study will be to optimize brain development in babies with congenital heart disease (CHD) who sometimes demonstrate delay in the development of cognitive and motor skills. This can be a result of multiple factors including altered prenatal oxygen delivery, brain blood flow and genetic factors associated with surgery including exposure to the heart lung machine.
The award will be used to complete three specific aims of a Phase 1 safety study as described in the NIH grant:
“NIH supported studies in our laboratory have shown that MSC therapy may be extremely helpful in improving brain development in animal models after cardiac surgery,” says Dr. Ishibashi. “MSC infusion can help reduce inflammation including prolonged microglia activation that can occur during surgery that involves the heart lung machine.”
In addition the researchers’ studies have demonstrated that cell-based intervention can promote white matter regeneration through progenitor cells, restoring the neurogenic potential of the brain’s own stem cells that are highly important in early brain development.
The Phase 1 clinical trial is being implemented in two stages beginning with planning, regulatory documentation, training and product development. During the execution phase, the trial will focus on patient enrollment. Staff from the Cellular Therapy Laboratory, led by director Patrick Hanley, Ph.D., manufactured the BM-MSC at the Center for Cancer and Immunology Research, led by Dr. Bollard. The Advanced Pediatric Brain Imaging Laboratory, led by Catherine Limperopoulos, Ph.D., will perform MR imaging.
The phase 1 safety study will set the stage for a phase 2 effectiveness trial of this highly innovative MSC treatment aimed at reducing brain damage, minimizing neurodevelopmental disabilities and improving the postoperative course in children with CHD. The resulting improvement in developmental outcome and lessened behavioral impairment will be of enormous benefit to individuals with CHD.



During the last few weeks of pregnancy, certain regions of the fetal brain experience exponential growth but also are more vulnerable to injury during that high-growth period.
Yao Wu, Ph.D., a research postdoctoral fellow in the Developing Brain Research Laboratory at Children’s National Health System, has received a Thrasher Research Fund early career award to expand knowledge about regions of the fetal brain that are vulnerable to injury from congenital heart disease (CHD) during pregnancy.
CHD, the most common birth defect, can have lasting effects, including overall health issues; difficulty achieving milestones such as crawling, walking or running; and missed days at daycare or school, according to the Centers for Disease Control and Prevention. Brain injury is a major complication for infants born with CHD. Catherine Limperopoulos, Ph.D., director of Children’s brain imaging lab, was the first to provide in vivo evidence that fetal brain growth and metabolism in the third trimester of pregnancy is impaired within the womb.
“It remains unclear which specific regions of the fetal brain are more vulnerable to these insults in utero,” Limperopoulos says. “We first need to identify early brain abnormalities attributed to CHD and understand their impact on infants’ later behavioral and cognitive development in order to better counsel parents and effectively intervene during the prenatal period to safeguard brain health.”
During the last few weeks of pregnancy, certain regions of the fetal brain experience exponential growth but also are more vulnerable to injury during that high-growth period. The grant, $26,749 over two years, will underwrite “Brain Development in Fetuses With Congenital Heart Disease,” research that enables Wu to utilize quantitative, non-invasive magnetic resonance imaging (MRI) to compare fetal brain development in pregnancies complicated by CHD with brain development in healthy fetuses of the same gestational age.Wu will leverage quantitative, in vivo 3-D volumetric MRI to compare overall fetal and neonatal brain growth as well as growth in key regions including cortical grey matter, white matter, deep grey matter, lateral ventricles, external cerebrospinal fluid, cerebellum, brain stem, amygdala and the hippocampus.
The research is an offshoot of a prospective study funded by the National Institutes of Health that uses advanced imaging techniques to record brain growth in 50 fetuses in pregnancies complicated by CHD who need open heart surgery and 50 healthy fetuses. MRI studies are conducted during the second trimester (24 to 28 weeks gestational age), third trimester (33 to 37 weeks gestational age) and shortly after birth but before surgery. In addition, fetal and neonatal MRI measurements will be correlated with validated scales that measure infants’ and toddlers’ overall development, behavior and social/emotional maturity.
“I am humbled to be selected for this prestigious award,” Wu says. “The findings from our ongoing work could be instrumental in identifying strategies for clinicians and care teams managing high-risk pregnancies to optimize fetal brain development and infants’ overall quality of life.”

In 2017, clinicians and research faculty working at Children’s National Health System published more than 850 research articles about a wide array of topics. A multidisciplinary Children’s Research Institute review group selected the top 10 articles for the calendar year considering, among other factors, work published in high-impact academic journals.
“This year’s honorees showcase how our multidisciplinary institutes serve as vehicles to bring together Children’s specialists in cross-cutting research and clinical collaborations,” says Mark L. Batshaw, M.D., Physician-in-Chief and Chief Academic Officer at Children’s National. “We’re honored that the National Institutes of Health and other funders have provided millions in awards that help to ensure that these important research projects continue.”
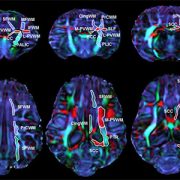
The published papers explain research that includes using imaging to describe the topography of the developing brains of infants with congenital heart disease, how high levels of iron may contribute to neural tube defects and using an incisionless surgery method to successfully treat osteoid osteoma. The top 10 Children’s papers:
Read the complete list.
Dr. Batshaw’s announcement comes on the eve of Research and Education Week 2018 at Children’s National, a weeklong event that begins April 16, 2018. This year’s theme, “Diversity powers innovation,” underscores the cross-cutting nature of Children’s research that aims to transform pediatric care.


“Bone marrow stem cells are used widely for stroke patients, for heart attack patients and for those with developmental diseases,” explains Nobuyuki Ishibashi, M.D. “But they’ve never been used to treat the brains of infants with congenital heart disease. That’s why we are trying to understand how well this system might work for our patient population.”
The National Institutes of Health (NIH) awarded researchers at Children’s National Health System $2.6 million to expand their studies into whether human stem cells could someday treat and even reverse neurological damage in infants born with congenital heart disease (CHD).
Researchers estimate that 1.3 million infants are born each year with CHD, making it the most common major birth defect. Over the past 30 years, advances in medical technology and surgical practices have dramatically decreased the percentage of infants who die from CHD – from a staggering rate of nearly 100 percent just a few decades ago to the current mortality rate of less than 10 percent.
The increased survival rate comes with new challenges: Children with complex CHD are increasingly diagnosed with significant neurodevelopmental delay or impairment. Clinical studies demonstrate that CHD can reduce oxygen delivery to the brain, a condition known as hypoxia, which can severely impair brain development in fetuses and newborns whose brains are developing rapidly.
Nobuyuki Ishibashi, M.D., the study’s lead investigator with the Center for Neuroscience Research and director of the Cardiac Surgery Research Laboratory at Children’s National, proposes transfusing human stem cells in experimental models through the cardio-pulmonary bypass machine used during cardiac surgery.
“These cells can then identify the injury sites,” says Dr. Ishibashi. “Once these cells arrive at the injury site, they communicate with endogenous tissues, taking on the abilities of the damaged neurons or glia cells they are replacing.”
“Bone marrow stem cells are used widely for stroke patients, for heart attack patients and for those with developmental diseases,” adds Dr. Ishibashi. “But they’ve never been used to treat the brains of infants with congenital heart disease. That’s why we are trying to understand how well this system might work for our patient population.”
Dr. Ishibashi says the research team will focus on three areas during their four-year study – whether the stem cells:
At the conclusion of the research study, Dr. Ishibashi says the hope is to develop robust data so that someday an effective treatment will be available and lasting neurological damage in infants with congenital heart disease will become a thing of the past.
Nobuyuki Ishibashi, M.D., and a team of researchers looked the effects of cardiopulmonary bypass surgery on the white matter of an animal model.
Mortality rates for infants born with congenital heart disease (CHD) have dramatically decreased over the past two decades, with more and more children reaching adulthood. However, many survivors are at risk for neurodevelopmental abnormalities associated with cardiopulmonary bypass surgery (CPB), including long-term injuries to the brain’s white matter and neural connectivity impairments that can lead to neurological dysfunction.
“Clinical studies have found a connection between abnormal neurological outcomes and surgery, but we don’t know what’s happening at the cellular level,” explains Nobuyuki Ishibashi, M.D., Director of the Cardiac Surgery Research Laboratory at Children’s National. To help shed light on this matter, Ishibashi and a team of researchers looked at the effects of CPB on the white matter of an animal model.
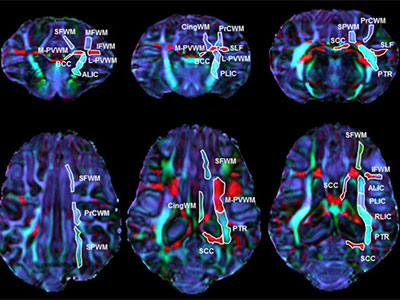
The research team randomly assigned models to receive one of three CPB-induced insults: a sham surgery (control group); full-flow bypass for 60 minutes; and 25°C circulatory arrest for 60 minutes. The team then used fractional anisotropy — a technique that measures the directionality of axon mylenation — to determine white matter organization in the models’ brains. They also used immunohistology techniques to assess the integrity of white matter oligodendrocytes, astrocytes and microglia.
The results, published in the Journal of the American Heart Association, show that white matter experiences region-specific vulnerability to insults associated with CPB, with fibers within the frontal cortex appearing the most susceptible. The team also found that fractional anisotropy changes after CPB were insult dependent and that regions most resilient to CPB-induced fractional anisotropy reduction were those that maintained mature oligodendrocytes.
From these findings, Ishibashi and his co-authors conclude that reducing alterations of oligodendrocyte development in the frontal cortex can be both a metric and a goal to improve neurodevelopmental impairment in the congenital heart disease population. “Because we are seeing cellular damage in these regions, we can target them for future therapies,” explains Ishibashi.
The study also demonstrates the dynamic relationship between fractional anisotropy and cellular events after pediatric cardiac surgery, and indicates that the technique is a clinically relevant biomarker in white matter injury after cardiac surgery.


Children’s National researchers led by Catherine Limperopoulos, Ph.D., demonstrate for the first time that the brains of high-risk infants show signs of functional impairment before they undergo corrective cardiac surgery.
Newborns with congenital heart disease (CHD) requiring open-heart surgery face a higher risk for neurodevelopmental disabilities, yet prior studies had not examined whether functional brain connectivity is altered in these infants before surgery.
Findings from a Children’s National Health System study of this question suggest the presence of brain dysfunction early in the lives of infants with CHD that may be associated with neurodevelopmental impairments years later.
Using a novel imaging technique, Children’s National researchers demonstrated for the first time that the brains of these high-risk infants already show signs of functional impairment even before they undergo corrective open heart surgery. Looking at the newborns’ entire brain topography, the team found intact global organization – efficient and effective small world networks – yet reduced functional connectivity between key brain regions.
“A robust neural network is critical for neurons to travel to their intended destinations and for the body to carry out nerve cells’ instructions. In this study, we found the density of connections among rich club nodes was diminished, and there was reduced connectivity between critical brain hubs,” says Catherine Limperopoulos, Ph.D., director of the Developing Brain Research Laboratory at Children’s National and senior author of the study published online Sept. 28, 2017 in NeuroImage: Clinical. “CHD disrupts how oxygenated blood flows throughout the body, including to the brain. Despite disturbed hemodynamics, infants with CHD still are able to efficiently transfer neural information among neighboring areas of the brain and across distant regions.”
The research team led by Josepheen De Asis-Cruz, M.D., Ph.D., compared whole brain functional connectivity in 82 healthy, full-term newborns and 30 newborns with CHD prior to corrective heart surgery. Conventional imaging had detected no brain injuries in either group. The team used resting state functional connectivity magnetic resonance imaging (rs-fcMRI), a imaging technique that characterizes fluctuating blood oxygen level dependent signals from different regions of the brain, to map the effect of CHD on newborns’ developing brains.
The newborns with CHD had lower birth weights and lower APGAR scores (a gauge of how well brand-new babies fare outside the womb) at one and five minutes after birth. Before the scan, the infants were fed, wrapped snugly in warm blankets, securely positioned using vacuum pillows, and their ears were protected with ear plugs and ear muffs.
While the infants with CHD had intact global network topology, a close examination of specific brain regions revealed functional disturbances in a subnetwork of nodes in newborns with cardiac disease. The subcortical regions were involved in most of those affected connections. The team also found weaker functional connectivity between right and left thalamus (the region that processes and transmits sensory information) and between the right thalamus and the left supplementary motor area (the section of the cerebral cortex that helps to control movement). The regions with reduced functional connectivity depicted by rs-fcMRI match up with regional brain anomalies described in imaging studies powered by conventional MRI and diffusion tensor imaging.
“Global network organization is preserved, despite CHD, and small world brain networks in newborns show a remarkable ability to withstand brain injury early in life,” Limperopoulos adds. “These intact, efficient small world networks bode well for targeting early therapy and rehabilitative interventions to lower the newborns’ risk of developing long-term neurological deficits that can contribute to problems with executive function, motor function, learning and social behavior.”
