Dr. Levitt has performed over 10,000 surgeries to address the wide spectrum of problems involving the colon and rectum — more than any other full time practicing pediatric surgeon in the world.
Patients with a previously repaired anorectal malformation (ARM) can suffer from complications which lead to incontinence. Reoperation can improve the anatomic result, but its impact on functional outcomes has previously been unclear.
Marc Levitt, M.D., chief of Colorectal and Pelvic Reconstructive Surgery at Children’s National, and Richard Wood, M.D., chief of Colorectal and Pelvic Reconstruction at Nationwide Children’s Hospital, co-led the study when they worked together in Columbus. They performed a retrospective cohort study, from 2014 to 2019, of patients with a previously repaired ARM who underwent another posterior sagittal anorectoplasty (PSARP) procedure, essentially redoing their first procedure. When results from the initial assessment were compared to 12 months after the redo surgery, they found that patients with fecal incontinence after an ARM repair can, with a reoperation, have their anatomy corrected, restoring continence for many and also improving their quality of life.
The study, published in the Journal of Pediatric Surgery, found that at one-year post-redo operation, 50 percent of the patients were on laxatives only, and 75 percent of those patients were completely continent. Overall, 77 percent of the patients were clean (1 or fewer accident per week) after their redo surgery and complication rates were low. Strictures were the most common complication seen after reoperations, as no dilations were performed, but were easily managed with a minor procedure. Surprisingly, 20 percent of patients with expected poor continence potential became fully continent on a laxative-based regimen after redo surgery. Traditionally, many of these children would not even be offered a redo surgery, given their perceived poor potential for bowel control.
The Division of Colorectal & Pelvic Reconstructive Surgery at Children’s National is the first in the mid-Atlantic region to fully integrate surgery, urology, gynecology and gastroenterology into one cohesive program for children. Dr. Levitt is a world-renowned surgeon who has performed over 10,000 surgeries to address the wide spectrum of problems involving the colon and rectum — more than any other full time practicing pediatric surgeon in the world.
This study shows that redo surgeries are a safe and effective option for patients with fecal incontinence after an anorectal malformation repair. The authors hope that the findings will lead to the ability to help more patients who suffer from complications and/or incontinence after a prior repaired ARM and who can benefit from an improvement in their colorectal anatomy. After a reoperation, patients can expect to have improved quality of life because the outcome gives them more freedom and less worry about soiling accidents.
To access the full article published in the Journal of Pediatric Surgery click here.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/Marc-Levitt-and-patient.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-11-04 14:02:372020-11-12 10:01:03Reoperation of anorectal malformation repair restores continence, improves quality of life
This included a webinar of case discussions on “Decision Making in Pediatric Colorectal Surgery,” led by Marc Levitt, M.D., Colorectal and Pelvic Reconstructive Surgeon at Children’s National Hospital. The international panel included Giulia Brisighelli (Johannesburg, ZA) Martin Lacher (Leipzig, Germany), Paula Midrio (Triviso, Italy), Carlos Reck (Vienna, Austria), Pim Sloots (Rotterdam, Netherlands), Gaia Tamaro (EUPSA Education Office), Alejandra Villanova (Madrid, Spain), and Tomas Wester (Stockholm, Sweden).
Dr. Levitt has since presented follow-up webinars on the following topics:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/DEFINITIVO-EUPSA-2020-Save-the-Date.png400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-10-20 01:33:312020-12-23 15:04:23Decision making in pediatric colorectal surgery webinars
While the way we deliver healthcare is changing rapidly, far too often the tools we use to treat children are stuck in the past.
Over the last decade, pediatric medical device innovation, particularly for the youngest, most fragile children, has made dismal progress. Of the Class 3 (high risk/high benefit) medical devices approved by FDA for pediatrics in the last 10 years, less than 4% are for ages 0-2 years old; and even less for neo-natal patients. Simply put, as medical devices advance, children are not seeing the benefit of innovation.
One of the keynote panelists, and leading voices on this issue, is Children’s National Hospital president and CEO Kurt Newman, M.D. Dr. Newman, a former pediatric surgeon, knows firsthand that every day in our nation’s pediatric hospitals, surgeons are manipulating adult medical devices to create creative solutions for children’s bodies because it’s the only available option.
“Children need and deserve devices that are conceived and designed with their biology and future in mind,” says Dr. Newman. “While children may only make up a small percentage of our population – maybe 20 or 25% – they are 100% of our future.”
“Children need and deserve devices that are conceived and designed with their biology and future in mind,” says Children’s National Hospital president and CEO Kurt Newman, M.D. “While children may only make up a small percentage of our population – maybe 20 or 25% – they are 100% of our future.”
Dr. Newman also addressed the current barriers to pediatric device innovation, which ranges from limited pediatric clinical trials to a market size that’s not financially appealing.
“The truth is, the frontiers of pediatric medicine are really in the innovative treatments, devices, therapies, and cures awaiting us on the other side of research and development.,” says Dr. Newman.
Former CNN correspondent, Jeanne Meserve, moderated the 45-minute keynote panel discussion, asking questions about the challenges to pediatric innovation, what policy changes need to take place to see improvement in the field of pediatric device innovation, and how federal funding can assist in creating change.
Michelle McMurry-Heath, new CEO of DC-based Biotechnology Innovation Organization (BIO), who joined Dr. Newman on this keynote panel, agreed that more needs to be done in the pediatric space. Dr. McMurry-Heath believes the Food and Drug Administration (FDA) is a public health advocate at heart and that the Pediatric Device Consortia (PDC), which Children’s National Hospital is part of, is starting to make new advancements in pediatric innovation by giving FDA clearance to more start-up companies than we’ve seen in the past.
“The FDA is interested in is what improves the health outcomes for the people and innovation is a huge piece. This is an important part of their mission and it is starting to yield benefits,” says Dr. Michelle McMurry-Heath. “Innovation is a team sport – it’s not easy. It takes a village of expertise and collaboration to progress and projects like the Pediatric Device Consortia is an important piece in this puzzle.”
To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, with seven devices having received either their FDA market clearance or CE marking.
Dr. McMurry-Heath also addressed the challenge of diseases that don’t exist in adults and posed the question, “How do you create a device for kids if it doesn’t exist in adults?” She cited the lack of market in pediatrics and the difficulty in bringing a device to market as problems that hinder innovation, which is why advocating for these devices is crucial to children’s healthcare everywhere.
“So much of our innovation comes from our small, innovative companies,” say Dr. McMurry-Heath. “For example, my company is working on a COVID-19 tracker now and 70% of the innovation is coming from our smallest biotech companies. It’s a race against time for these companies to bring their innovation to market in order to keep the lights on and pay their scientists; this dog-eat-dog world isn’t immediately obvious to outsiders.
Beyond advocating, Dr. Newman and Children’s National are developing the first-of-its-kind pediatric research and innovation campus, which is currently under construction at DC’s former Walter Reed Army Medical Center site.
“We secured 12 acres to create something that has never been done before and that’s a campus for innovation dedicated to children,” says Dr. Newman. “Our close proximity to federal research institutions and agencies enables the new Children’s National campus to leverage the rich ecosystem of public and private sectors to help bolster biohealth, medical device, and life science innovation.”
As Children’s National continues to champion ways to accelerate pediatric device development, one focus is the on-site incubator Johnson & Johnson Innovation – JLABS, which will help start-up companies strengthen their ideas by working with coaches, having access to mentors and learning how to interact with the FDA. This partnership also offers an audience for their device which could potentially lead to investments.
The Children’s National Research & Innovation Campus will create an ecosystem that can accelerate breakthroughs in pediatric healthcare discoveries and technologies: The new campus is currently under construction and expected to open in the first quarter of 2021.
Both panelists agreed they’d like to see more flexibility with regulators to work with innovators in order create more incentives for them to present their device, like the NCC-PDI “Make Your Medical Device Pitch for Kids!” Competition, which was recently held in September 2020. The six winners received up to $50,000 in FDA-funded grant awards in order to develop their device, eventually bring it to market in order to improve healthcare for kids.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/Pediatric-device-innovation-panelists.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-10-16 13:31:312024-09-06 15:18:57Accelerating pediatric device innovation through legislative processes and industry changes
The 8th Annual Pediatric Device Innovation Symposium presented by @ChildrensNatl in conjunction with @Devices4kids took place Sept. 28-30.
The 8th Annual Pediatric Device Innovation Symposium presented by Children’s National Hospital in conjunction with the National Capital Consortium for Pediatric Medical Devices (NCC-PDI) kicked off on Monday, Sept. 28, 2020 with a panel featuring three fellow members of the FDA-funded Pediatric Device Consortia (PDC) Grants Program discussing real-world evidence and the vital role that innovation and technology play in advancing healthcare for the pediatric population.
As described by the FDA, real-world evidence (RWE) is the clinical evidence regarding the usage and potential benefits or risks of a medical product, derived from the analysis of patient data. RWE can be generated by different study designs or analyses, including but not limited to, randomized trials, including large simple trials, pragmatic trials and observational studies (prospective and/or retrospective).
The symposium panel, “Pediatric Device Consortia Update on the Use of Real-World Evidence (RWE) for Pediatric Device Innovation” examined real-world evidence (RWE) demonstration projects from Southwest Pediatric Device Consortium, UCSF-Stanford Pediatric Device Consortium and the West Coast Consortium for Technology and Innovation in Pediatrics (CTIP). The panel was moderated by Juan Espinoza, M.D., FAAP, director of CTIP.
“Real-world evidence projects are critical to the advancement of pediatric medical device innovation,” said Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National Hospital, and principal investigator for NCC-PDI. “Bringing together our colleagues in pediatric healthcare through the symposium helps us together identify solutions that will bring medical device innovations to the market faster to benefit the children and families we all serve.”
Here are some of the key discussion points made by panelists regarding current RWE demonstration projects:
Emerging medical and consumer technologies are enabling the diabetes community to take great strides toward truly personalized, real-time, data-driven management.
“Connected” technologies such as smartphone apps, wearable devices and sensors create an ecosystem of data driven-tools that can link patients and care teams for precision management of conditions like diabetes, including predicting a hypoglycemic event.
RWE has an important future in treating rare diseases by using existing data and harnessing that to improve treatment among pediatric patients.
Through the rich data in academic healthcare systems, practitioners are better equipped to provide RWE to address important regulatory and research questions.
The creation of a pediatric device patient database, which provides real-time updates to clinical, device and patient-generated health data, offers several regulatory, safety and research advantages in advancing device innovation.
Kolaleh Eskandanian, PhD, MBA, PMP, vice president and chief innovation officer at Children’s National Hospital, and principal investigator for NCC-PDI.
The FDA currently supports RWE demonstration projects that are focused on understanding data quality, improving RWE tools and evaluating RWE approaches to study design and data analytics. Dr. Espinoza highlighted the importance of ongoing dialogue on the use of RWE as it pertains to innovations that advance pediatric healthcare across the board.
“Thank you to the NCC-PDI team for creating this opportunity for PDCs to talk about the impact of real-world evidence on pediatric medical device development and the projects we have to move that field forward,” said Dr. Espinoza, director of CTIP and principal investigator on the PDC’s RWE Demonstration Project. “These projects are intended to inform the FDA and the industry’s approach to RWE including study design, data standards, fitness for use and regulatory decision making and reproducibility. This is complicated work that involves research, IT infrastructure, clinical care and operations.”
NCC-PDI, which is led by the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland, is one of five members of the FDA’s Pediatric Device Consortia Grant Program. To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, with seven devices having received either their FDA market clearance or CE marking.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/Symposium_Final.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-10-16 10:21:382025-03-10 11:19:22Real-world evidence and the impact on pediatric device innovation
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/NCC-PDI-device-competition.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-10-02 12:53:032025-03-10 11:29:24Medical device competition announces six winners to share in $250K
A collaboration between clinical and basic science researchers including Drs. Ishibashi, Hashimoto-Torii, Jonas, and Deutsch, seeks to to understand how caspase enzyme activation plays a role in the development of fine and gross motor skills in children who underwent cardiac surgery for CHD repair.
The U.S. Department of Defense has awarded $2 million to Children’s National Hospital to study how a family of protease enzymes known as caspases may contribute to brain cell degeneration when activated by prolonged anesthesia and cardiopulmonary bypass during cardiac surgery for congenital heart disease.
This U.S. Army Medical Research Acquisition Activity Award, Anesthesia Neurotoxicity in Congenital Heart Disease, is led by principal investigator Nobuyuki Ishibashi, M.D., with both clinical and basic science co-investigators including Kazue Hashimoto-Torii, Ph.D., (Neuroscience), Richard Jonas, M.D., (Cardiovascular Surgery) and Nina Deutsch, M.D., (Anesthesiology).
While the specific cellular and molecular mechanisms of how anesthesia and cardiac surgery impact cortical development are poorly understood, both seem to impact brain growth and development in young children. The most common neurologic deficit seen in children after CHD surgical repair is the impairment of fine and gross motor skills.
Both anesthetic agents and inflammation like that seen as a result of cardiopulmonary bypass have also been shown to contribute to the activation of a specific group of enzymes that play an essential role in the routine (programmed) death of cells: caspases. However, recent pre-clinical research shows that these enzymes may also contribute to other alterations to cells beyond cell death, including making changes to other cell structures. In pre-clinical models, these changes cause impairments to fine and gross motor skills – the same neurological deficits seen in children with CHD who have undergone procedures requiring prolonged anesthesia and cardiopulmonary bypass.
The research team hypothesizes that caspases are extensively activated as a result of cardiac surgery and while that activation is rarely causing reduced numbers of neurons, the changes that caspase enzymes trigger in neurons are contributing to neurological deficits seen in children with CHD after surgery.
While the study focuses specifically on the impacts of cardiac surgery for correction of a heart defect, the findings could have major implications for any pediatric surgical procedure requiring prolonged anesthesia and/or cardiopulmonary bypass.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/07/doctors-operating.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-07-02 13:47:222024-10-29 15:31:50U.S. DoD awards $2M for study to protect neurological function after cardiac surgery
“Innovation in children’s medical devices consistently lags behind that of adults and we need to change that if we are to confront the challenge to children’s health of COVID-19 and future pandemics,” said Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI.
As medical data increasingly highlights the serious impact of COVID-19 on children’s health, the National Capital Consortium for Pediatric Device Innovation (NCC-PDI) announces a special pitch competition focused on COVID-19-related pediatric medical devices that support home health monitoring and telehealth, and improve sustainability, resiliency and readiness in diagnosing and treating children during a pandemic.
“Despite early reports that COVID-19 posed less of a threat to children, a recent study published by Children’s National shows that considerable numbers of pediatric patients are hospitalized and become critically ill from the disease,” said Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “Innovation in children’s medical devices consistently lags behind that of adults and we need to change that if we are to confront the challenge to children’s health of COVID-19 and future pandemics.”
Funding for the competition is made possible by a grant from the Food and Drug Administration (FDA) and a philanthropic gift from Mei Xu, founder of e-commerce platform Yes She May, a site dedicated to women-owned brands.
Along with grant funding, one company from the competition will be selected by Johnson & Johnson Innovation – JLABS to receive a one-year residency at JLABS @ Washington, DC, which will be located on the new Children’s National Research & Innovation Campus currently under construction. In addition to the 2021 JLABS residency, the awardee will have access to the JLABS community and expert mentoring by the Johnson & Johnson family of companies.
Submissions for the competition are being accepted now through Monday, July 6, 2020z at the NCC-PDI website, Innovate4Kids.org, where complete details can be found.
NCC-PDI is one of five members in the FDA’s Pediatric Device Consortia Grant Program created to support the development and commercialization of medical devices for children, which lags significantly behind the progress of adult medical devices. Along with Children’s National, University of Maryland and Medtech Innovator, NCC-PDI members include accelerator BioHealth Innovation and design firm Archimedic.
To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, with seven devices having received either their FDA market clearance or CE marking. The consortium hosts a major pediatric pitch competition annually that showcases and awards promising pediatric innovations and provides a first-of-its-kind pediatric-focused accelerator program for finalists.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/NCC-PDI-COVID19-Edition-Competition-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-06-17 15:32:282025-03-10 11:14:07NCC-PDI launches special pediatric medical device competition focused on covid-19 innovations
Children’s National Hospital in Washington, D.C., was ranked No. 7 nationally in the U.S. News & World Report 2020-21 Best Children’s Hospitals annual rankings. This marks the fourth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide.
In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fourth year in a row.
For the tenth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“Our number one goal is to provide the best care possible to children. Being recognized by U.S. News as one of the best hospitals reflects the strength that comes from putting children and their families first, and we are truly honored,” says Kurt Newman, M.D., president and CEO of Children’s National Hospital.
“This year, the news is especially meaningful, because our teams — like those at hospitals across the country — faced enormous challenges and worked heroically through a global pandemic to deliver excellent care.”
“Even in the midst of a pandemic, children have healthcare needs ranging from routine vaccinations to life-saving surgery and chemotherapy,” said Ben Harder, managing editor and chief of Health Analysis at U.S. News. “The Best Children’s Hospitals rankings are designed to help parents find quality medical care for a sick child and inform families’ conversations with pediatricians.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/US-News-2020-ID.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-06-16 01:00:292024-12-30 12:50:15Children’s National ranked a top 10 children’s hospital and No. 1 in newborn care nationally by U.S. News
Nobuyuki Ishibashi, M.D., is the principal investigator on a $3.2 million NIH R01 to study white matter growth and repair in utero for fetal brains affected by congenital heart disease.
Many of the neurological deficits seen in children with congenital heart disease (CHD) are related to abnormal white matter development early in life caused by reduced oxygen supply to the brain while in utero. Children with immature white matter at birth also commonly sustain additional white matter injuries following cardiac surgery.
The research, titled “White matter protection in the fetus with congenital heart disease,” looks specifically at whether providing a supplemental amount of the naturally occurring tetrahydrobiopterin (BH4) for pregnant women could rescue white matter development of fetuses with congenital heart disease whose brains aren’t receiving enough oxygen – or suffering from hypoxic-ischemic events.
Previous preclinical studies have shown that this lack of oxygen depletes the brain’s natural BH4 level, and the researchers hypothesize that BH4 levels play a critical role in the growth and development of white matter in the fetal brain by triggering key cellular/molecular processes. Specifically, the study will focus on three aims:
Establish in a preclinical model the optimal protective regiment for women pregnant with a fetus who has CHD to receive BH4.
Determine the appropriate approach to deliver BH4 to this population
Leverage genetic tools and biochemical techniques in the laboratory to better understand where and how BH4 levels play a role in the growth (or lack thereof) of oligodendrocytes—the primary cells of white matter.
This laboratory-based work is the first step to determining if the neurodevelopment of babies born with CHD can be preserved or recovered by addressing key brain development that occurs before the baby is even born. Findings related to congenital heart disease may also translate to other populations where white matter development is affected by hypoxia-ischemia, including premature infants.
The project is led by principal investigator Nobuyuki Ishibashi, M.D., with co-investigators Vittorio Gallo, Ph.D., Joseph Scafidi, D.O., and Mary Donofrio, M.D. as well as colleagues at MedStar Washington Hospital Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/Nobuyuki-Ishibashi.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-06-11 15:34:522023-09-18 11:52:59R01 grant funds white matter protection study for congenital heart disease
The study was co-led by Marc Levitt, M.D., who launched the division of Pediatric Colorectal and Pelvic Reconstructive Surgery at Children’s National Hospital in late 2019.
A prospective randomized controlled trial has given pediatric colorectal specialists the first evidence to reconsider a standard postoperative care practice: Routine anal dilations following a primary posterior sagittal anorectoplasty (PSARP), an operation to reconstruct a child born with imperforate anus. This treatment has been the standard of care following PSARP for more than thirty years and was believed to help prevent strictures after surgery for anorectal malformations (imperforate anus). However, it requires parents and caregivers to perform this uncomfortable procedure on their child daily, which can have a significant psychological impact on the child. Prior to this trial, a quality of life assessment found that postoperative dilations were the most stressful part of these patients’ care for both patient and parents.
“The PSARP procedure, performed for the first time in 1980, improves the lives of children born with imperforate anus by providing a safe and effective reconstruction technique,” says Marc Levitt, M.D., who led the study with co-author Richard Wood, M.D., of Nationwide Children’s Hospital, before joining Children’s National Hospital as chief of the division of Colorectal and Pelvic Reconstructive Surgery. “We are thrilled to have evidence that one of the top postoperative challenges for parents – a twice daily anal dilation for several months after the surgery is completed – can potentially be eliminated for most kids with no impact on their recovery.”
“We also found that if a stricture, or scar, develops, which occurs in only about 10 percent of cases, it can easily be managed with a minor operative procedure done at the same time as colostomy closure, which in most cases they already need. So, if a family had to choose between daily dilations for months or a one in 10 risk of needing a minor surgical procedure, they can now make that choice and avoid routine dilations.”
The prospective single institution randomized controlled trial was conducted between 2017 and 2019 and included 49 patients. The abstract of the results was accepted for presentation at the British Association of Paediatric Surgeons Annual International Congress, 2020, and its manuscript is to be published.
“The clinical benefit of routine dilation had never been studied in a formal way, it had been accepted as surgical dogma. Our cohort, who underwent a randomized controlled trial, gave us the ability to look at this practice in an evidence-based way,” Dr. Levitt says. “Revising this practice could be a real game-changer for parents and kids with anorectal malformations.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/Marc-Levitt-and-patient.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-06-11 15:15:382020-07-27 15:56:17Evidence to eliminate burdensome postop practice after imperforate anus repair
Matthew Oetgen, M.D., MBA, chief of orthopaedics and sports medicine at Children’s National Hospital, presented findings from a study aimed at improving quality and safety for pediatric spinal fusion procedures by reducing surgical site infection rates.
Pediatric orthopaedic surgery as a field is focused on improving quality and value in pediatric spine surgery, especially when it comes to eliminating surgical site infections (SSI). Many studies have documented how and why surgical site infections occur in pediatric spinal fusion patients, however, there is very little data about what approaches are most effective at reducing SSIs for these patients in a sustainable way.
At the Pediatric Orthopaedic Society of North America’s 2020 Annual Meeting, Matthew Oetgen, M.D., MBA, chief of orthopaedic surgery and sports medicine at Children’s National Hospital, presented findings from a long-term single institution study of acute SSI prevention measures.
“These findings give us specific insight into the tactics that are truly preventing, and in our case sometimes even eliminating, SSIs for pediatric scoliosis surgery,” says Dr. Oetgen, who also served on the annual meeting program committee. “By analyzing patient records across more than a decade, we were able to see that some strategies are quite effective, and others, that we thought would move the needle, just don’t.”
The team reviewed medical records and radiographs dating back to 2008 for 1,195 patients who had spinal fusion for scoliosis, including idiopathic scoliosis as well as other forms such as neuromuscular or syndromic scoliosis. Over that period of time, the division of orthopaedics and sports medicine at Children’s National was collaborating with the hospital’s infection control team to achieve several programmatic implementation milestones, including:
January 2012: Standardized infection surveillance program
July 2013: Standardized perioperative infection control protocols including those for pre-operative surgical site wash, surgical site preparation and administration of antibiotics before and after surgery
March 2015: Standardized comprehensive spinal care pathway including protocols for patient temperature control, fluid and blood management, and drain and catheter management
Over the study time period, the team found that SSIs did decrease, but interestingly, the rate did not progressively decrease with each subsequent intervention.
“Instead, we found that the rate went down and was even eliminated for some subgroups when the perioperative infection control protocols were implemented in 2013 and sustained through the study period end,” says Dr. Oetgen. “The other programmatic efforts that started in 2012 and 2015 had no impact on infection rates.”
He also notes that the study’s findings have identified a crucial component in the process for infection control in pediatric spinal surgery—perioperative protocols. “A relatively uncomplicated perioperative infection control protocol did the best job decreasing SSI in spinal fusion. Future efforts to optimize this particular protocol may help improve the rates even further.”
Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
Highlights from the Children’s National Research Institute annual report
In 2018, Children’s National began construction of its new Research & Innovation Campus (CNRIC) on 12 acres of land transferred by the U.S. Army as part of the decommissioning of the former Walter Reed Army Medical Center campus. In 2020, construction on the CNRIC will be complete, and in 2012, the Children’s National Research Institute will begin to transition to the campus.
In late 2019, a team of scientists led by Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, traveled to the Democratic Republic of Congo to collect samples from 60 individuals that will form the basis of a new reference genome data set. The researchers hope their project will generate better reference genome data for diverse populations, starting with those of Central African descent.
A gift of $5.7 million received by the Center for Translational Research’s director, Lisa Guay-Woodford, M.D., will reinforce close collaboration between research and clinical care to improve the care and treatment of children with polycystic kidney disease and other inherited renal disorders.
The Center for Neuroscience Research’s integration into the infrastructure of Children’s National Hospital has created a unique set of opportunities for scientists and clinicians to work together on pressing problems in children’s health.
Children’s National and the National Institute of Allergy and Infectious Diseases are tackling pediatric research across three main areas of mutual interest: primary immune deficiencies, food allergies and post-Lyme disease syndrome. Their shared goal is to conduct clinical and translational research that improves what we know about those conditions and how we care for children who have them.
An immunotherapy trial has allowed a little boy to be a kid again. In the two years since he received cellular immunotherapy, Matthew has shown no signs of a returning tumor — the longest span of time he’s been tumor-free since age 3.
In the past 6 years, the 104 device projects that came through the National Capital Consortium for Pediatric Device Innovation accelerator program raised $148,680,256 in follow-on funding.
Even though he’s watched more than 500 aspiring physicians pass through the Children’s National pediatric residency program, program director Dewesh Agrawal, M.D., still gets teary at every graduation.
Understanding and treating the novel coronavirus (COVID-19)
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, is looking at whether or not the microbiome of bacteria in the human nasal tract acts as a defensive shield against COVID-19.
Catherine Bollard, M.D., MBChB, director of the Center for Cancer and Immunology Research, and her team are seeing if they can “train” T cells to attack the invading coronavirus.
Sarah Mulkey, M.D., Ph.D., an investigator in the Center for Neuroscience Research and the Fetal Medicine Institute, is studying the effects of, and possible interventions for, coronavirus on the developing brain.
You can view the entire Children’s National Research Institute academic annual report online.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/Vittorio-Gallo-and-Marc-Batshaw.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-05-19 14:08:392024-06-28 13:19:46Children’s National Research Institute releases annual report
Patients and staff at the Uganda Heart Institute for RHD-related heart surgeries in Uganda, March 2020. These patients were originally scheduled as part of the cancelled medical mission, but UHI cardiovascular surgeon successfully managed these cases without the support of the mission doctors from the U.S.
In early March as countries around the globe began to wrestle with how best to tackle the spread of COVID-19, a group of doctors, nurses, researchers and other medical staff from Children’s National Hospital were wrestling with a distinct set of challenges: What to do about the 10 Ugandan children and adults who were currently scheduled for lifesaving heart surgery (and the countless others who would benefit from the continued training of the local heart surgery team) to correct complications of rheumatic heart disease (RHD) during an impending medical mission in the country.
Rheumatic heart disease impacts over 39 million people globally and causes nearly 300,000 deaths per year. RHD is the result of frequent, untreated streptococcal throat infections in childhood that ultimately cause the body’s immune system to repeatedly damage heart valves. It is completely preventable, yet the majority of the world’s children still live in impoverished and overcrowded conditions that predispose them to RHD. Most patients present with advanced valvular heart disease. For example, in Uganda, an RHD registry includes over 600 children with clinical RHD, of which nearly 40% die within four years and the median survival time from enrollment in the registry is only nine months. For these patients, heart surgery is the only viable solution for long-term survival and normal quality of life.
Patricia: 9-year-old from Gulu (northern Uganda), had mitral valve replacement and was doing well on a recent follow-up visit at her home.
The scheduled trip from Washington was part of a nearly 20-year partnership** between doctors, nurses, researchers and other medical staff in the United States, including Craig Sable, M.D., associate chief of cardiology, and and Pranava Sinha, M.D.,pediatric cardiovascular surgeon, at Children’s National Hospital in Washington, D.C., and the Uganda Heart Institute in Kampala, Uganda. The partnership aims to tackle RHD head-on. It provides surgical skill transfer, allows for treatment of more complex patients, and increases sustainable surgical capacity for Uganda’s RHD patients over time. As a result, over the last 15 years more than 1,000 children have received lifesaving heart surgery in Uganda, with the Uganda Heart Institute (UHI) performing one to two heart valve surgeries every two weeks over the last few years.
Jackline: 12-year-old from Gulu, had mitral valve repair and aortic valve replacement. Jackline and Patricia were diagnosed through one of our research programs and benefit from our novel telehealth program, which helps connect patients from remote parts of Uganda to specialists at UHI.
COVID-19 was changing the current plan, however. Travel between countries was limited, and the team from the U.S. wouldn’t have been permitted to leave the U.S. and return according to schedule. The trip, and the support teams who were scheduled to arrive to help with the surgeries, were cancelled. The U.S. team members who had already arrived in Uganda were sent home after helping their UHI colleagues set up and prepare for the surgeries as much as possible. Knowing that patients and families were counting on the surgery mission to go forward after waiting for months or years to have surgery for heart valve disease, UHI decided not to cancel the majority of the surgeries. Instead, for the first time, they planned and successfully completed five valve-related cases in a single week – several of them quite complex. The cardiologists and cardiac surgeons from Children’s National who were supposed to be in-country for these procedures were forced to limit their in person assistance to the set-up activities the week prior to surgery and telehealth consult during the procedures.
“It was hard not to be able to stay and work with the UHI team to help these families,” says Dr. Sable. “But we are so proud of the UHI team for meeting this challenge on their own. We knew they had the skills to perform at this volume and complexity. It’s a proud moment to see the team accomplish this major milestone, and to see the patients they cared for thrive.”
The patients are the most important outcome: The five who had successful open-heart surgery are all doing well, either on their way to recovery or already discharged to their communities, where they will, for the first time in memory, be able to play, exercise and go to school or work.
Longer term, this success demonstrates the UHI medical team’s ability to manage greater surgical capacity even when surgical missions from the U.S. resume. The partnership’s goal is to complete at least 1,000 annual operations (both pediatric and adult), with the majority being performed by the local team. Having this capacity available will mean the difference between life and death for many children and adults who have RHD in Uganda and the surrounding countries.
**This work is supported by the Edwards Life Sciences/Thoracic Surgery Foundation, the Emirates Airline Foundation, Samaritan’s Purse Children’s Heart Project and Gift of Life International.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/04/Faces-of-RHD.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-04-29 16:55:222025-02-28 12:23:54Lifesaving heart surgeries for RHD complications in Uganda go on despite COVID-19
Children’s National Hospital announced that world-class surgeon Yves d’Udekem, M.D., Ph.D., will become the next Chief of Cardiac Surgery and Co-Director of the Children’s National Heart Institute this summer.
Dr. d’Udekem is Belgian-born with Canadian and Australian citizenship and received his early training in Belgium and Toronto. As an attending cardiac surgeon in Belgium, he operated on both adults and children with congenital heart disease. Dr. d’Udekem then worked with internationally recognized heart surgeon Marc de Laval, M.D., FRCS, and others in London to train in congenital heart surgery at the Great Ormond Street Hospital for Children.
From there, he was recruited to The Royal Children’s Hospital in Melbourne, Australia, an institution that has been a leader in advancing the field of congenital heart disease. In Melbourne, Dr. d’Udekem built an outstanding reputation for clinical excellence and an exceptional academic career. He has over 300 publications and is highly cited and respected. Dr. d’Udekem obtained more than $7 million in grant funding over the past five years as the creator and leader of the highly touted Fontan Registry.
The Children’s National Cardiology team and hospital leadership have built a framework for Dr. d’Udekem to succeed and advance the legacy that has been so successfully created in cardiac surgery by Richard Jonas, M.D. Dr. Jonas is a world leader in congenital heart surgery who made significant clinical and academic advances in the field and will continue his award-winning research career at Children’s National in the laboratory focusing on neurodevelopmental outcomes for children with heart disease.
Children’s National offers a comprehensive surgical program that includes a team of experienced surgeons performing the full range of procedures available for treatment of pediatric cardiac disease and congenital heart defects. The high volume program serves neonates through adults with congenital heart disease with particular attention to neurodevelopmental outcomes.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/03/Yves-dUdekem.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-03-03 15:35:172024-09-06 15:05:31Yves d’Udekem, M.D., Ph.D., named Chief of Cardiac Surgery and Co-Director of the Children’s National Heart Institute
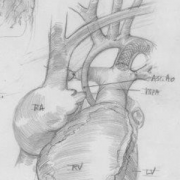
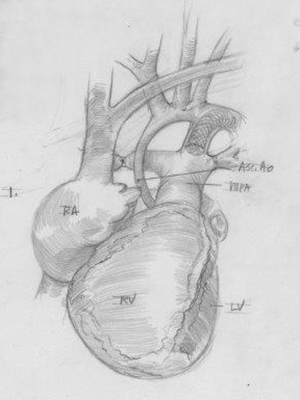
Illustration of a hybrid stage I palliation with bilateral bands on the lung vessels and a stent in the ductus arteriosus for patients with small left heart structures.
A new LinkedIn post from Kurt Newman, M.D., president and CEO of Children’s National Hospital, tells a story about the hospital’s cardiac surgeons and interventional cardiologists working with the U.S. Food and Drug Administration (FDA) to bring a better-sized, less-invasive vascular stent to the U.S. for the first time. The stent holds open a newborn’s ductus arteriosus, a key blood vessel that keeps blood flowing to the body, until the baby is big and strong enough to undergo a serious open-heart procedure for repair of hypoplastic left heart syndrome.
He writes, “Why is this important? At less than 6 lbs., these patients have arteries that are thinner than a toothpick – less than 2mm in diameter. Currently, the stent used in these children is an FDA approved device for adult vascular procedures, adapted and used off-label in children. It is not always well suited for the smallest babies as it is too large for insertion through the artery and often too long as well. The extra length can create immediate and long-term complications including obstructing the vessel it is supposed to keep open.
“While I am proud of the talent and dedication of our Children’s National cardiac surgery and interventional cardiology teams, I tell this story to illustrate a larger point – innovation in children’s medical devices matters. What’s unfortunate is that development and commercialization of pediatric medical devices in the U.S. continues to lag significantly behind adults…We can and must do better.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/02/tiny-stent-illustration-horizontal.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-02-25 15:02:562023-07-03 10:40:59Thinking small for newborns with critical congenital heart disease
Pediatric innovators pitch for up to $250,000 in FDA-funded grant awards.
The National Capital Consortium for Pediatric Device Innovation (NCC-PDI) announced today that the application deadline for its annual “Make Your Medical Device Pitch for Kids!” competition is extended one week to Feb. 22 at midnight EST. Innovators and startup companies with devices in the pediatric cardiovascular, orthopedic and spine, or NICU sectors are invited to apply for a share of up to $250,000 in FDA-funded awards and access to a newly created NCC-PDI pediatric device accelerator program led by MedTech Innovator. Submissions are being accepted now.
Up to 30 companies will be selected for the first round of competition scheduled for March 23, 2020 at the University of Maryland, College Park. Up to 10 finalists chosen from that event will compete for up to $250,000 in grant awards in Toronto, Canada on October 4. Finalists also receive a spot in the MedTech Innovator 2020 Accelerator – Pediatric Track, which provides a customized curriculum and in-depth mentorship. Finalists will be announced in May, 2020.
“This year’s competition focuses on three medical device areas of critical need for pediatric patients, so we want to give innovators as much time as possible to prepare their submissions,” said Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI . “Our goal is to support devices that will improve care for children by helping them advance on the pathway to commercialization. We have seen how this competition can provide significant momentum for pediatric innovations, so we want to encourage as much participation as possible.”
To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, notes Eskandanian, with six devices having received either their FDA market clearance or CE marking. Along with the positive exposure of presenting at this competition, she notes that the success of NCC-PDI’s portfolio companies is attributed to funding, mentorship, support from partners and facilitated interactions between device innovators and potential investors.
Eskandanian notes that enhancing access to resources for pediatric innovators is one aim of the Children’s National Research & Innovation Campus, a first-of-its-kind campus focused on pediatric healthcare innovation, currently under development on the former Walter Reed Army Medical Center campus in Washington, D.C. With its proximity to federal research institutions and agencies, universities, academic research centers, as well as on site accelerator Johnson & Johnson Innovation – JLABS, the campus will create a rich ecosystem of public and private partners which, like the NCC-PDI network, will help bolster pediatric innovation and commercialization. Opening is scheduled for December 2020.
Albert Oh, M.D., Director of the Cleft and Craniofacial Program at Children’s National Hospital.
The American Cleft Palate-Craniofacial Association (ACPA) recognized Albert Oh, M.D., with the 2020 Emerging Leader Award. This award is given to professionals who have been members of ACPA between three to 15 years, and who exhibit exemplary accomplishments and dedication to the issues affecting people with cleft and craniofacial conditions.
The ACPA is an association consisting of professionals who treat and/or perform research on cleft and craniofacial conditions. The nonprofit organization also supports those affected through education and resources through its ACPA Family Services program.
As the director of the Cleft and Craniofacial Program at Children’s National Hospital, Dr. Oh is a leader in the research, surgical treatment and holistic care of cleft and craniofacial patients. He has published over 75 peer-reviewed scientific articles and book chapters. Dr. Oh’s current research interests include the outcomes and safety of cleft and craniofacial procedures, 3-D analysis of craniofacial morphology, Pierre Robin sequence and vascular anomalies.
Dr. Oh says that “It is an honor to be recognized by the ACPA and to share their mission of advancing research and improving outcomes for all those affected by cleft and craniofacial conditions.”
Dr. Oh will be presented with his award during the ACPA’s 77th Annual Meeting in Portland, Or.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/01/Albert-Oh.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2020-01-28 16:17:542020-04-30 16:43:07Albert Oh, M.D., receives 2020 Emerging Leader Award from the ACPA
The competition focuses on pediatric devices in three areas of critical need: cardiovascular, orthopedic and spine, and neonatal intensive care (NICU) and is now accepting applications. Contestants will pitch for a share of up to $250K in grant awards and the opportunity to participate in the MedTech Innovator 2020 Accelerator – Pediatric Track.
The first stage of competition will be held on March 23 at the University of Maryland and will include up to 30 companies selected from all submissions received. Up to 10 finalists selected from that event will move on to the “Make Your Medical Device Pitch for Kids!” finals on October 4, 2020 in Toronto, Canada. Finalists from the March qualifying round will be notified in May, 2020.
“While there is a great need for pediatric devices in many specialty areas, the development and commercialization process is very challenging because of the small market size and dynamic characteristics of the patient population,” says Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “To provide pediatric innovators with greater support in meeting these unique challenges, we must go beyond grant funding, which is why we are collaborating with MedTech Innovator to offer an accelerator program with a pediatric track.”
To date, NCC-PDI has mentored over 100 medical device sponsors to help advance their pediatric innovations, notes Eskandanian, with six devices having received either their FDA market clearance or CE marking. She says the success of NCC-PDI’s portfolio companies is attributed to funding, mentorship, support from partners, facilitated interactions between device innovators and potential investors, and being discovered during their presentations at the signature “Make Your Medical Device Pitch for Kids!” competitions.
While advancements have been made in some pediatric specialties, there is still a critical need for novel devices in cardiovascular, orthopedic and spine, and NICU areas. On average over the past decade, only 24 percent of life-saving medical devices approved by FDA – those that go through PMA and HDE regulatory pathways – have an indication for pediatric use. Of those, most are designated for children age 12 or older. “Devices designed specifically for the younger pediatric population are vitally needed and, at this early stage of the intervention, can significantly improve developmental outcomes for a child,” Eskandanian said.
Enhancing access to resources for pediatric innovators is also one of the aims of the Children’s National Research and Innovation Campus, a first-of-its-kind focused on pediatric healthcare innovation, currently under development on the former Walter Reed Army Medical Center campus in Washington, D.C. and opening in December, 2020. With its proximity to federal research institutions and agencies, universities, academic research centers, as well as on site accelerator Johnson and Johnson Innovation – JLABS, the campus will create a rich ecosystem of public and private partners which, like the NCC-PDI network, will help bolster pediatric innovation and commercialization.
Recently, Kurt Newman, M.D., president and CEO of Children’s National Hospital, authored an opinion piece for the popular political website, The Hill. In the article, he called upon stakeholders from across the landscape to address the significant innovation gap in children’s healthcare versus adults.
As Chair of the Board of Trustees of the Children’s Hospital Association, Dr. Newman knows the importance of raising awareness among policy makers at the federal and state level about the healthcare needs of children. Dr. Newman believes that children’s health should be a national priority that is addressed comprehensively. With years of experience as a pediatric surgeon, he is concerned by the major inequities in the advancements of children’s medical devices and technologies versus those for adults. That’s why Children’s National is working to create collaborations, influence policies and facilitate changes that will accelerate the pace of pediatric healthcare innovation for the benefit of children everywhere. One way that the hospital is tackling this challenge is by developing the Children’s National Research & Innovation Campus, which will be the nation’s first innovation campus focused on pediatric research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/02/Kurt-Newman-capitol-building.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2019-12-11 15:41:002023-07-10 10:07:22Making healthcare innovation for children a priority