
Pandemic stress in pregnant mothers may affect anxiety regions of babies’ brains

The research from Children’s National Hospital provides mounting evidence that children of the pandemic, even those far too young to understand it, need ongoing assessments of developmental or mental health support later in life.
A critical part of the brain linked to risks for anxiety later in life – the left amygdala – was significantly smaller by volume in babies of mothers who reported stress during the COVID-19 pandemic, according to a new manuscript published in JAMA Network Open.
The right hippocampus, which governs spatial, visual and verbal memories, and the white matter were also reduced in children whose mothers reported stress.
The research from Children’s National Hospital provides mounting evidence that children of the pandemic, even those far too young to understand it, need ongoing assessments of developmental or mental health support later in life.
“Looking ahead, we want to use this information – and studies with similar findings – to empower pregnant mothers to request support to mitigate their stress, especially in the event of another global health crisis,” said Nickie Andescavage, M.D., a neonatologist and principal investigator at the Center for Prenatal, Neonatal & Maternal Health Research. “We also want to make sure babies born during COVID-19 get the services that they need in life if they develop anxiety or other mental health disorders.”
The fine print
Researchers at the center used magnetic resonance imaging (MRI) to compare the brains of 103 babies born between 2014 and 2019 prior to the pandemic to 59 born between 2020 and 2022. Mothers who had COVID-19 or other complications in their pregnancies were excluded. The babies underwent MRI imaging while in utero and again soon after delivery.
The mothers were evaluated for stress and anxiety, using the Spielberger State-Train Anxiety Inventory and other evidence-based scoring measures. Pre-pandemic, 21% of mothers reported elevated symptoms of anxiety; in the pandemic cohort, that number jumped to nearly 62%.
Their babies’ brains were also changed, as regions widely understood to control emotion and anxiety displayed smaller volumes on MRI imaging. Given the global impact of the pandemic and universal reports of mental distress worldwide, the potential impact of these findings may impact an entire generation of children born during the pandemic. The team is just beginning to unravel the medical significance.
What’s next
Catherine Limperopoulos, Ph.D., director of the Center for Prenatal, Neonatal & Maternal Health Research, said understanding the impact of stress is vital in supporting the healthy development of young children. Current studies are underway at her center to tease apart the role of stress in prenatal development and examine its long-term impact on development, including cognition, behavior and mental health.
“We all know that being pregnant can be quite stressful, and there are certain times of collective stress that can provide us windows to understand how the body and mind manage it,” Dr. Limperopoulos said. “At our center, we care deeply about the health of mothers and babies, and our researchers plan to continue investigating the role of stress in development to continue building data to show that mental health must be a greater priority.”
This study – “Prenatal maternal psychological distress during the COVID-19 pandemic and newborn brain development” – was supported by the National Institutes of Health, the Intellectual and Developmental Disabilities Research Center, and the A. James & Alice B. Clark Foundation. You can read the full study in JAMA Network Open.





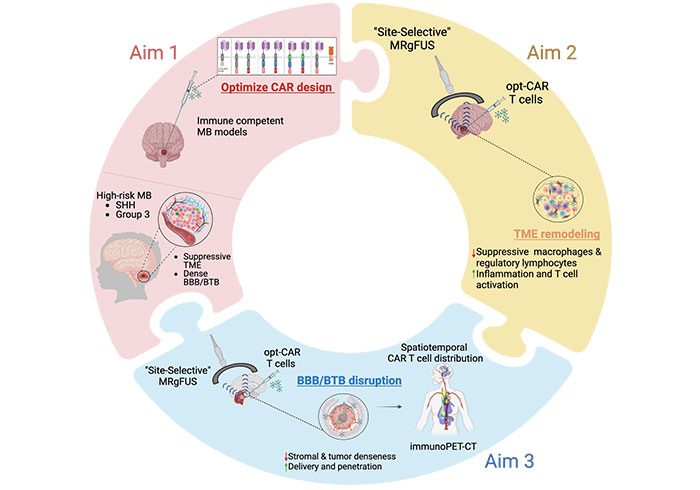 A Children’s National Hospital researcher is embarking on a two-year project that could revolutionize the care of rare pediatric brain tumors, through a Department of Defense (DOD) award to study the efficacy of combining the powers of acoustic therapy and cellular immunotherapy to treat the deadliest forms of medulloblastoma.
A Children’s National Hospital researcher is embarking on a two-year project that could revolutionize the care of rare pediatric brain tumors, through a Department of Defense (DOD) award to study the efficacy of combining the powers of acoustic therapy and cellular immunotherapy to treat the deadliest forms of medulloblastoma.






























 The Children’s National Research Institute released its
The Children’s National Research Institute released its 



