Hear, smell, taste. These senses impact and shape children’s everyday lives. Diego Preciado, MD, PhD, chief of Otolaryngology and Joseph E. Robert, Jr. Professor of Pediatric Otolaryngology, aims to set the gold standard for care of a child’s ear, nose and throat (ENT) — pathways to the senses. “We treat the senses that drive an individual’s personality,” he says. “ENT care has seen wonderful advances in the last 30 years, but there is still more work to do. That’s why I entered the field.”
Dr. Preciado is an innovator. His team, at the Sheikh Zayed Institute for Pediatric Surgical Innovation, helped to advance early detection and treatment of otolaryngology disorders, such as hearing loss, the most common sensory impairment in children. Four in every 1,000 infants are born with it.
In the laboratory, the team uncovered fundamental molecular aspects of chronic ear disease. This led to the development of new medications aimed at reducing the need for surgery. The team and collaborators are developing a drug delivery method, using liposomal nanoparticles — spherical vesicles that are insoluble in water — to carry treatments directly into the ear canal. It could potentially eliminate the need for oral antibiotics and surgery in children with recurrent ear infections. The team also developed an app to guide patients through critical aspects of ENT care. It will help kids with hearing impairments in language development after cochlear implantation.
“At Children’s National,” says Dr. Preciado, “the future is all about helping children get better faster.”
Dr. Preciado’s team works across the hospital and with parent groups in our community to remove barriers to ENT care. “All care is not equal,” he says. “Sadly, families with public or no health insurance typically only receive care at a much later date. This delay often permanently impacts their children’s hearing, speech and social skills.”
Currently in development is a medical and educational intervention model for patients with complex ENT needs. It includes expanding critical wraparound services and creating new care solutions. The focus is precision medicine and personalized therapies. Continuing refinement of our fellowship program to train pediatric otolaryngologists is helping to build a strong workforce for the future.
“Real change can happen only by adopting a team approach to care. An effective leader must be an equal member of the team and lead by example. Children’s National is committed to this approach and ensuring that everyone receives expert care in the same manner.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/Preciado-examnies-Jorge-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-07-02 15:51:172025-07-02 15:52:16Caring for the senses to support children’s development
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/Article_Image_400x300_Bollard-Permar.jpg12501667Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-06-24 10:00:042025-06-24 11:29:49Podcast: Mission Critical: The Importance of Pediatric Research
A new AI tool developed by Children’s National and Howard University analyzes brain immune cells 10,000x faster than manual methods.
A new Machine Learning and Artificial Intelligence tool from researchers at Children’s National Hospital (CNH) and Howard University (HU) accelerates discoveries in brain inflammation. Called StainAI, it rapidly and accurately analyzes microglia, the brain’s immune cells. Scientists currently analyze microglia slowly by hand. StainAI automates this process and speeds it up 10,000-fold. Its use will aid discovery of new treatments for inflammatory brain conditions such as infection, autoimmunity, and aging.
Solving a problem
Traditionally, scientists study microglia one cell at a time. They reconstruct each cell’s shape by hand under a microscope. The shape helps classify microglia as “resting” (normal) or “activated” (inflamed). The manual process is tedious and slow. It limits analyses to a few microglia in small brain areas.
StainAI changes that. It uses deep machine learning and artificial intelligence to overcome and exceed the manual method’s limitations. It correctly classifies millions of microglia from standard microscopic images. StainAI also localizes each microglia to its brain region in 3D. These features enable single-cell analyses of immune activity at a scale not feasible before – the entire brain.
A tool with broad impact
The team applied StainAI to two models of brain injury and inflammation to show its utility. In a rodent model of pediatric cardiac arrest, StainAI identified new brain regions susceptible to injury. In a simian model of viral infection, StainAI localized rod-shaped microglia normally found in white matter to an unexpected brain region – the hippocampus. These findings point towards new treatments and highlight StainAI’s value across diseases and species.
StainAI is fast, accurate and adaptable. It uses common laboratory equipment. Its creators, Michael Shoykhet, MD, PhD, at CNH and Dr. Tsang-Wei Tu at HU, are making StainAI available to other researchers. They hope StainAI will help labs worldwide discover new ways to protect children’s brains from inflammation and injury.
“This project is exciting as it targets more precise surgery with improved safety in terms of decreased radiation,” says Matthew Oetgen, MD, division chief of Orthopaedic Surgery and Sports Medicine at Children’s National.
What if surgeons could fix a child’s hip with pinpoint accuracy – using fewer X-rays and cutting-edge robotics? That’s the promise of a new National Institutes of Health funded project combining 3D imaging and robotic technology to improve the treatment of slipped capital femoral epiphysis (SCFE), a condition that affects the hip joint in growing children.
What’s been the hold-up in the field?
Right now, orthopedic surgeons place screws by hand using 2D X-ray images to guide them. To see the screw from different angles, they have to move the X-ray machine around. “The screw must be placed near the center of the femoral head, but not penetrate it,” says Kevin Cleary, PhD, associate director of engineering at the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). This process takes time and can increase the amount of radiation the patient receives.
Even though better tools like 3D imaging and surgical robots exist, they aren’t used together in current surgical practice. “Individual procedures have nuances that require their own validated workflows,” says Tyler Salvador, a research engineer at Children’s National Hospital. In other words, each type of surgery is different, and doctors need proven steps before using new technology in the operating room.
How does this work move the field forward?
This project brings together low-dose 3D X-rays from nView with a small surgical robot called Micromate™ to help place screws more precisely during SCFE surgeries. “Our research group has been developing robotics, imaging, and related technologies to improve surgical procedures,” says Dr. Cleary. While these tools exist separately, putting them together in one system focused on bone surgery is new. Tyler Salvador adds, “This will provide a complete solution for precision SCFE implant placement and verification.”
“This project is exciting as it targets more precise surgery with improved safety in terms of decreased radiation,” says Matthew Oetgen, MD, division chief of Orthopaedic Surgery and Sports Medicine at Children’s National. “This is a paradigm-shifting effort that will improve outcomes while improving safety which is the holy grail of translational clinical research. It embodies the goal of the SZI — combining technical expertise with surgical leadership to improve outcomes in pediatric surgery.”
Children’s National leads the way
Children’s National is unique because the Sheikh Zayed Institute combines research and clinical care in one place. “Having the labs right inside the hospital helps us work closely with doctors,” says Salvador.
Together, this work is paving the way for safer, faster and more precise surgeries for children with hip problems. By combining advanced imaging and robotics, the team at Children’s National is helping shape the future of pediatric orthopedic care. In addition to this robotic hip pinning project, the Children’s National team is also behind two additional groundbreaking projects including robotic gallbladder removal and a kidney surgery initiative.
This project has been funded in whole with federal funds from the National Institutes of Health under Contract No.R01EB035559.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/Oetgen-hip-pinning-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-06-09 14:36:072025-06-09 14:37:42Transforming pediatric hip surgery with robotics and 3D imaging
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success.
A novel immunotherapy approach that involves training autologous T cells derived from peripheral blood mononuclear cells (PBMCs) has shown early signs of safety and efficacy in a small pre-clinical model. The approach, pioneered by researchers within the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital, may have future implications for the treatment of intractable pediatric solid tumors such as neuroblastoma.
What it means
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success. There is an urgent need for innovative strategies to effectively target these tumors.
This study presents another approach to cell therapy that collects peripheral blood mononuclear cells from the patient and teaches them to target and eliminate solid tumor cells through exposure to similar tumor cells in a controlled laboratory setting. The cells are then primed to find and attack the solid tumor cells when reintroduced, an approach known as adoptive immunotherapy.
What’s new
The authors note that more well-established modalities such as CAR-T and TCR-T therapies have also made significant advances and demonstrate clinical promise at battling cancers such as neuroblastoma. However, the approach presented in the paper offers early promise of an additional potential strategy, especially in a context “where simplicity, speed and safety are priorities.”
By using small molecule treatments, the authors induce an immunogenic response in neuroblastoma tumor cells, making them more recognizable and attackable by immune cells. Ex vivo training of PBMCs with treated neuroblastoma cells exhibited strong tumor-killing activity.
The authors highlight a few key differences of this approach versus existing adoptive cellular therapies. The method “is technically straightforward, requiring only small tumor samples and peripheral blood mononuclear cells (PBMCs), and avoids the need for the complex genetic engineering intrinsic to CAR-T and TCR-T manufacturing,” the authors write. This method leverages ex vivo tumor cell modification, which may mitigate systemic toxicities. “Additionally, because our approach is not limited to a few surface antigens, it may expand the repertoire of actionable tumor-associated targets.”
Children’s National leads the way
Children’s National is a leader in the development of cell therapies for a wide range of pediatric conditions, including pediatric cancer, HIV/AIDS, sickle cell disease and others.
This research is the latest development in a decade-plus of focused research in adoptive immunotherapy within the Center for Cancer and Immunology Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
What’s next
The authors write that there are several critical areas for future research to advance this approach, including a need to understand the specific T cell component and receptors involved in recognizing tumor antigens. They will also need to explore the longevity of the trained T cell response including studies of the memory and persistence of trained PBMCs to ensure lasting anti-tumor effects. Finally, the team will explore the risk of T cell exhaustion, which could reduce the effectiveness of the therapy over time.
Though work remains, the authors note, “Our findings lay the groundwork for developing this approach into a viable therapy for neuroblastoma and possibly other solid tumors as well.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/cancer-cells-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-06-09 10:03:082025-06-09 10:05:08Preliminary study points to efficacy of PBMC-based immunotherapy for neuroblastoma
Using Fitbit data from the the largest long-term study of brain development and child health in the United States, researchers employed machine learning to test whether physiological markers could accurately predict ADHD diagnoses.
A new study published in Frontiers in Child and Adolescent Psychiatry reveals that common wearable devices like Fitbits may hold the key to improving how we identify Attention-Deficit/Hyperactivity Disorder (ADHD) in adolescents. By analyzing patterns in heart rate, activity levels and energy expenditure, researchers were able to predict ADHD diagnoses with striking accuracy, offering a glimpse into a future where objective, real-time data supports earlier and more personalized mental healthcare.
A fresh approach to a common challenge
ADHD affects approximately 1 in 10 children and adolescents in the United States. It is typically diagnosed based on parent and teacher reports, clinical interviews and behavioral observations. While effective, these methods rely heavily on subjective interpretation and can sometimes miss important nuances in how symptoms appear over time. This study, led by Muhammad Mahbubur Rahman, PhD, and colleagues at Children’s National, sought to determine whether wearable health data could help fill that gap.
Turning Fitbit metrics into meaningful insights
The study used data from 450 adolescents who were part of the larger Adolescent Brain Cognitive Development (ABCD) study, the largest long-term study of brain development and child health in the United States. Each participant wore a Fitbit, which captured three key activity and physiological measures:
Resting Heart Rate (RHR) – the number of heart beats per minute while the body is at rest
Sedentary Time – time spent with little or no physical activity
Energy Expenditure – estimated calories burned through physical activity
When the researchers compared these measures between teens with and without ADHD, they found statistically significant differences. Teens with ADHD had consistently higher resting heart rates and showed distinctive patterns in both their movement and stillness.
To go further, the team applied a machine learning model to test whether these physiological markers could accurately predict ADHD diagnoses. The model performed extremely well with 89% accuracy, 88% precision, 90% recall and a 0.95 area under the curve (AUC). These results suggest that the combination of passive, continuous data and predictive modeling could serve as a valuable screening tool, particularly in settings where full clinical evaluations are difficult to access.
A path toward more accessible mental healthcare
The implications are big. If validated in larger and more diverse populations, wearable-derived data could offer a low-cost, low-burden way to flag teens who might benefit from further ADHD evaluation. This could lead to earlier support, fewer misdiagnoses and more tailored treatment strategies.
Importantly, this approach isn’t about replacing clinicians, it’s about giving them better tools. Real-world, real-time data from wearables could act as an additional layer of insight that supports more precise, individualized care. As wearable technology becomes more embedded in daily life, its role in healthcare, especially adolescent mental health, is poised to grow.
Julia Finkel, MD, is a pediatric anesthesiologist and the director of Pain Medicine Research at the Sheikh Zayed Institute for Pediatric Surgical Innovation.
What if doctors could measure pain as precisely as they measure blood pressure? That’s the vision driving Julia Finkel, MD, a pediatric anesthesiologist and director of Pain Medicine Research at the Sheikh Zayed Institute for Pediatric Surgical Innovation. Recently featured in The Washington Post, Dr. Finkel is pioneering the Nociometer, a new device that could transform how we understand and treat pain.
This new innovation uses a painless electrical current on a finger or toe to gently stimulate the body’s three main sensory nerve fibers. It then measures pupil response — linked to the brain’s pain centers — to identify the type and intensity of pain.
Now heading into clinical trials, the Nociometer shows how federal funding fuels innovation for patients. Here, Dr. Finkel shares the inspiration behind her work and the vital role of federal support in pediatric research.
Q: What started you on the path to developing this device?
A: My father is a theoretical physicist. He often talked in lay terms about everything he was thinking. When I was a child, we’d go for walks at night and look at the stars, and he’d explain the universe. My mother was an artist, but she struggled with constant pain from rheumatoid arthritis. There weren’t very good therapeutics at the time. Pain impacted her quality of life.
As an undergraduate, I was a chemistry major and interested in the mechanisms of how things worked. I planned to be a rheumatologist, but switching to anesthesia was transformative.
Q: What did you love about anesthesiology?
A: I love how it profoundly impacts patients. You induce unconsciousness, you induce wakefulness and you eliminate pain. When pain stops for a child, it also lessens the suffering of the parents. Our research is all about gaining a deeper understanding of the mechanisms of pain.
The Nociometer helps identify the mechanism behind the pain symptom so we can treat it appropriately. Research shows us that pain has a recognizable signature in the body. Because we can recognize it, we can treat it better. It’s like having an X-ray to look at before treating a broken leg.
Q: What is it like to work with children experiencing chronic pain? Why is measuring pain this way more effective than the typical scale?
A: Families become desperate. Often, they have seen many doctors before coming to a specialist. But pain is a single word for many different disease states. Not everyone has the right expertise. We often see children with chronic abdominal pain. Perhaps they struggle in school or can’t go at all. They don’t eat well, they have trouble engaging in regular activities. The Nociometer helps us determine the cause of the pain to better treat the problem. The device also gives us a way to validate pain while the pain scale tells us perception. The Nociometer provides objective data, very similar to a blood pressure reading.
Q: How has federal funding, and support from Children’s National, shaped your work?
A: Federal funding has been absolutely critical. Initially, we had grants from multiple agencies within the National Institutes of Health (NIH). This shows how ubiquitous and problematic pain is across the board. It’s the underpinning of many disease states and an upstream driver of the opioid epidemic.
We have grants from the Small Business Innovation Research program within the National Cancer Institute. We have funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases and an award from the Advanced Research Projects Agency for Health. This federal funding comes with scientific rigor and the ecosystem at Children’s National has allowed me to accomplish so much.
Q: What makes Children’s National the right place for this kind of innovation?
A: Children’s National has given me the space to think creatively and pursue unconventional ideas. In 2011, I became a founding member of the Sheikh Zayed Institute for Pediatric Surgical Innovation. With early institutional support, I was able to explore questions that led to the discovery of a physiological biomarker for pain — the basis of the Nociometer.
“Creative” isn’t a word you often hear in medicine, but here, it’s part of the process. I was able to spin out a company, secure funding and build a prototype — steps that wouldn’t have been possible elsewhere. The culture at Children’s National embraces discovery and fuels real impact.
Julia Finkel, MD, is a pediatric anesthesiologist and Director of Pain Medicine Research and Development, The Sheikh Zayed Institute for Pediatric Surgical Innovation and Professor of Anesthesiology, Pediatrics and Critical Care Medicine at The George Washington University.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/Julia-Finkel-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-06-04 16:47:312025-06-05 12:42:51Behind the Nociometer: Q&A with Julia Finkel, MD
The multi-disciplinary team who implanted the first AVEIR leadless pacemakers at Children’s National.
Two new devices being used in adults with heart rhythm disorders — atrial and dual chamber leadless pacemakers and extravascular defibrillators — were successfully implanted in pediatric patients for the first time at Children’s National. These devices represent the latest technology in pacing and defibrillating the heart to maintain its rhythm. Though they are smaller in size, have fewer complications and longer battery life than most of the devices currently available for young patients, they have not been available for use in these younger patients until recently.
“For the first time, we’re bringing these devices that are smaller, smarter, less painful and more flexible to children and teenagers who can really benefit from them,” says Elizabeth Sherwin, MD, a pediatric cardiologist and electrophysiologist at Children’s National who led the teams completing these minimally invasive procedures.
The patient benefit
Offering implantation of these devices gives more children and adults with congenital heart disease access to the latest technologies in implantable heart rhythm devices, which may offer unique benefits for these groups.
Abbott AVEIR dual chamber leadless pacemaker is the newest FDA approved leadless pacemaker. It uses electricity to maintain heart rhythm and can be used to pace both the top and bottom chambers of the heart, which is particularly important for pediatric and adult congenital patients. These devices also:
Are designed to be removed and replaced after battery runs down, which is ideal for children and young adults who will have multiple replacements over a lifetime.
Long battery life, so fewer replacements may be necessary.
Can be placed minimally invasively
Dr. Sherwin says that the minimally invasive procedure and the lack of leads on these devices are particularly key for younger people because these factors remove or reduce the risk of complications commonly experienced with pacemakers in children. There is a reduced risk of bleeding, infection, lead movement or fracture, and long-term problems with the veins. Even better, because they are placed directly in the heart, there are no scars on the chest or visible signs of a pacemaker present.
Medtronic Aurora EV-ICD is an extravascular implantable cardioverter-defibrillator (ICD), which is implanted under the skin (subcutaneous) with a generator on the left chest wall and a lead that goes under the breastbone (sternum). The design includes:
A smaller generator.
No need to go through chest muscle, leading to less painful implantation and more comfort long term.
Emergency heart pacing through the substernal lead – both to try to terminate a fast arrhythmia to avoid need for a shock, and to treat in case the heartbeat is too slow.
Longer battery life (projected 11 years).
Avoids the need to have leads in the blood vessels, with the many potential complications that go along with transvenous leads.
For both of these newer devices, the patient’s size, weight and medical history will help determine if they are a good candidate.
The big picture
The Electrophysiology team is the first and only pediatric and congenital cardiology team trained to implant AVEIR leadless pacemakers and the Aurora EV-ICD for eligible individuals in the mid-Atlantic region. Dr. Sherwin, Charles Berul, MD, and Tom (Nak) Choi, MD, are trained to provide these procedures for people in Washington, DC, Virginia and Maryland. For both devices, Children’s National is among only a handful of children’s hospitals in the U.S. with the training and expertise to offer access to these technologies.
“This is a game-changer for kids with rhythm disorders and adults with congenital heart disease,” Dr. Sherwin says. “We are really excited to be among the first to offer these options for patients who need them.”
A new HIV-specific T cell therapy, tested in six adults living with HIV, used specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
An exciting small clinical trial led by the Center for Cancer and Immunology Research at Children’s National Hospital has shown that a new HIV-specific T cell therapy is safe and may help reduce hidden reservoirs of the virus in the body. This approach, tested in six adults living with HIV, uses specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
The results, published in Nature Communications, represent a step forward in the search for a long-term, drug-free way to control or even cure HIV.
A smarter way to fight HIV
Today, people living with HIV rely on anti-retroviral therapy (ART) to keep the virus under control. These medications are highly effective but must be taken daily and do not eliminate the virus entirely. That is because HIV can hide in a “reservoir” of cells where it remains dormant and invisible to both drugs and the immune system. If ART is stopped, the virus can quickly return.
To change that, scientists at Children’s National and partnering institutions developed a new type of cellular therapy called HST-NEETs — short for “HIV-specific T cells targeting conserved epitopes”. These T cells are trained in the lab to recognize parts of the virus that do not change much, even as HIV mutates. This makes it harder for the virus to escape. The goal is to help the immune system find and destroy the infected cells that are normally hidden.
Safe and promising results
In this phase 1 clinical trial, researchers created personalized HST-NEET therapy from each participant’s own immune cells. After training the cells to recognize HIV, they were infused back into the patients twice over a period of weeks.
The results showed that:
No serious side effects were reported from the infusions.
The treatment was well-tolerated by all six participants.
In two people, the therapy led to stronger HIV-specific immune responses, including more virus-fighting T cells and antibodies.
In two others, researchers saw a drop in the level of HIV hidden in their cells, a sign that the virus reservoir might be shrinking.
In four participants, the infused T cells persisted in the bloodstream for up to 40 weeks, continuing to patrol for signs of HIV.
While not a cure, these findings show early evidence that the therapy may help the body better recognize and fight HIV, even the hidden forms that are hardest to treat.
Building toward a cure
“The fact that we saw HIV-specific T cell responses increase in some participants, even without additional immune-boosting drugs, is very encouraging,” said Catherine Bollard, MBChB, MD, senior author of the study and director of the Center for Cancer and Immunology Research at Children’s National. “It suggests that the immune system can be trained to go after parts of the virus that were previously out of reach.”
Unlike bone marrow transplants, which have led to a cure in a few people with both HIV and cancer but carry high risk, HST-NEET therapy is much safer and more scalable. That is important for the millions of people living with HIV worldwide.
This study also sets the stage for future clinical trials that could combine T cell therapy with other strategies, like latency-reversing drugs that “wake up” hidden HIV, to further shrink the reservoir. It also shows that personalized T cells can be safely made, infused and tracked over time and that they can continue working in the body for many months. Those lessons are valuable not just for HIV but also for developing safer, more targeted cancer immunotherapies in children and adults.
What’s next
The next phase of research will evaluate this therapy in larger groups and under different conditions, including in people undergoing stem cell transplants or with added immune system boosters. Clinical trials are already underway exploring these combinations.
By focusing on preserved parts of the virus, the regions that HIV cannot easily mutate, HST-NEETs could one day become part of a combination approach to eliminate HIV from the body altogether.
“Every step brings us closer to a functional cure,” said Dr. Bollard. “And the lessons we’re learning from HIV may also inform how we treat other chronic viral infections, and even cancer, in the future.”
Authors authors from Children’s National include Danielle K. Sohai, Michael D. Keller, Patrick J. Hanley, Fahmida Hoq, Divyesh Kukadiya, Anushree Datar, Emily Reynolds, Christopher Lazarski, Chase D. McCann, Jay Tanna, Abeer Shibli, Haili Lang, Anqing Zhang, Pamela A. Chansky, Cecilia Motta and Conrad Russell Y. Cruz.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/tube-rack-in-lab-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-05-23 12:34:312025-05-23 12:35:29Personalized T cell therapy for HIV shows safety and early signs of impact
Dr. Tarini has extensively studied policies to optimize the delivery of genetic services for newborns and their families.
Children’s National Hospital named Beth A. Tarini, MD, MS, MBA, as the Richard and Agnes Hudson Endowed Chair in Health Services Research at Children’s National Hospital.
Dr. Tarini, a pediatrician, is the Co-Director of the Center for Translational Research in the Children’s National Research Institute, the hospital’s Director of Resident Research and a professor of pediatrics at George Washington University.
The big picture
Dr. Tarini joins a distinguished group of Children’s National physicians and scientists with an endowed chair. Children’s National is grateful to generous donors who have funded 51 professorships altogether.
Professorships support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and the donor’s commitment to advancing and sustaining knowledge.
Why it matters
Dr. Tarini has extensively studied policies to optimize the delivery of genetic services for newborns and their families. She has obtained $10 million in federal and foundation funding. A national leader in her field, she has served as president of the Society for Pediatric Research and as an appointed member of the Advisory Committee on Heritable Disorders in Newborns and Children. In the latter role, she helped advise the Secretary of the U.S. Department of Health and Human Services on the most appropriate application of universal newborn screening tests, technologies, policies, guidelines and standards.
“It’s an honor to receive the Hudson Chair, which allows me to bridge research and real-world impact,” says Dr. Tarini. “With this support, I will continue working to translate scientific discovery into better genetic services and policy for all newborns and their families.”
The visionary investment from the estate of Richard and Agnes Hudson will ensure that Dr. Tarini and future chairholders can launch bold new initiatives to rapidly advance the field of health services research, elevate the hospital’s academic leadership and improve the health and well-being of children.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/Beth-Tarini-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-05-19 10:54:132025-05-19 10:56:26Honor bestowed on Beth A. Tarini, MD, MS, MBA
“Healthcare is moving very fast. And what often happens in adults, also happens in children. Unfortunately, most of the research is directed initially at adults, and then whittles down to children. At Children’s National, we’re trying to turn that around. We’re trying to do research for children that will expand its way up to adults, turning it on its head.”
Anthony Sandler, MD, senior vice president and surgeon-in-chief, Joseph E. Robert Jr. Center for Surgical Care, and director of the Sheikh Zayed Institute for Pediatric Surgical Innovation highlighted the exciting research and innovation happening at Children’s National – including demonstrating a technology, led by Raj Shekhar, PhD, that uses real-time imaging with augmented reality to project live ultrasound visualization of a patient within the surgeon’s field of view. This enhances surgical precision and ultimately supports positive patient outcomes.
This conversation was a part of Axios’ inaugural Future of Health Summit – an event bringing together the top voices in healthcare, policy and technology to explore the biggest challenges and innovations shaping the future of medicine.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/Sandler-Axios-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-05-15 15:55:332025-05-15 16:13:36In the news: Axios’ Future of Health Summit
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-04-22 10:31:052025-06-10 12:20:52REI Week 2025 empowers the future in pediatric research and innovation
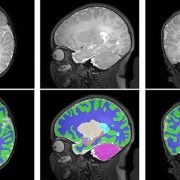
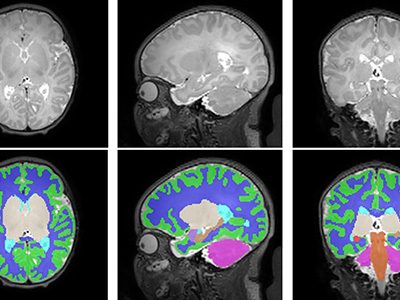
A new study out of the Center for Prenatal, Neonatal & Maternal Health Research, directed by Catherine Limperopoulos, PhD, led by Yao Wu, PhD and Stephanie Merhar, MD, MS, out of Cincinnati Children’s Hospital Medical Center, sought answers to the question: “Do brain volumes differ in opioid-exposed vs. unexposed newborns?” In one of the largest studies of this kind, researchers found that prenatal exposure to opioids is associated with smaller brain volumes in newborns. These findings from the landmark Outcomes of Babies with Opioid Exposure (OBOE) study build on, reinforce smaller studies, and achieve a better understanding of the impacts of prenatal opioid exposure (POE).
Dive Deeper
The Advancing Clinical Trials in Neonatal Opioid Withdrawal (ACT-NOW)’s OBOE study is a multi-site observational study of newborns with prenatal opioid exposure and a control group of unexposed newborns from four different sites in the United States – Case Western Reserve University, Cincinnati Children’s Hospital Medical Center, University of Alabama at Birmingham, and Children’s Hospital of Philadelphia.
In a study involving 173 newborns who were exposed to opioids during pregnancy and 96 newborns not exposed to opioids prenatally showed smaller brain sizes in several key areas. Specifically, these exposed babies had smaller total brain volumes, as shown through MRI, as well as reduced volumes in important parts of the brain, including the cortex (outer layer of the brain), deep gray matter (areas that control movement and emotions), white matter (which helps transmit signals in the brain), cerebellum (responsible for coordination and movement), brainstem (controls basic functions like breathing), and the amygdala (involved in emotions and memory).
Further details showed that newborns exposed to medication for opioid use disorder (MOUD) during pregnancy with methadone, had smaller white matter volumes, while those exposed to MOUD with buprenorphine had smaller volumes specifically in the right amygdala. Additionally, newborns who were exposed to opioids plus additional substances such as THC and gabapentin had smaller volumes in even more brain areas compared to those who were only exposed to opioids.
What’s Next
The OBOE study sets the groundwork for further research into the long-term impact of opioid exposure during pregnancy. Additional work is necessary to expand on these findings and how they relate to functions in childhood – including exploring the way these reduced brain volumes may impact cognitive, behavioral, and motor impairments. The study raises important questions about how current guidelines for MOUD during pregnancy – specifically with methadone and buprenorphine – might evolve considering these findings. This study highlights the need for further research to assess the long-term effects of MOUD regimens on both maternal and infant outcomes.
This significant study underscores the importance of multi-disciplinary collaboration in opioid exposure research, effective regulation, and policy interventions – involving healthcare providers, researchers, policymakers, and affected families – to best mitigate the consequences and improve the health outcomes of children affected by prenatal opioid exposure.
Additional authors from Children’s National include Kushal Kapse, BS, MS, and Josepheen De Asis-Cruz, MD, PhD. Other authors include Carla M. Bann, PhD, Jamie E. Newman, PhD4, Nicole Mack, MS, Sara B. De Mauro, MD, MSCE, Namasivayam Ambalavanan, MD, Jonathan M. Davis, MD, Scott A. Lorch, MD, MSCE5, Deanne Wilson-Costello, MD, Brenda B. Poindexter, MD and Myriam Peralta-Carcelen, MD.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/prenatal-opiod-exposure-CNRI-feature.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-04-15 15:08:582025-04-15 15:08:58New study finds prenatal opioid exposure linked to smaller newborn brain volumes
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/Article_Image_400x300_Linguraru.jpg12501667Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-04-14 11:05:362025-05-09 16:10:59Podcast: Future ready: AI’s role in revolutionizing pediatric care
New technology could revolutionize pain management by offering more accurate diagnoses and treatment.
Measuring pain remains one of the most challenging and imprecise tasks in medicine. However, new groundbreaking research led by Julia Finkel, MD, anesthesiologist, is underway to change that.
Dr. Finkel and scientists are pioneering the development of new tools like the Nociometer to measure pain objectively by analyzing nerve responses. This technology could revolutionize pain management by offering more accurate diagnoses and treatment, especially for those who struggle to express their pain, such as children or those with chronic conditions.
“In order to be most effective, I need to know why; what are the underpinnings of why you feel this way. Different components impact one’s perception of pain. Depression can exacerbate it. Happiness can mitigate it.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/03/nerve-cell-synapse-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-03-28 10:54:302025-03-28 10:54:30In the news: Researchers in the quest for accurate pain measurement
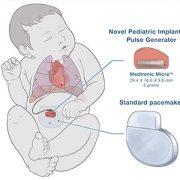
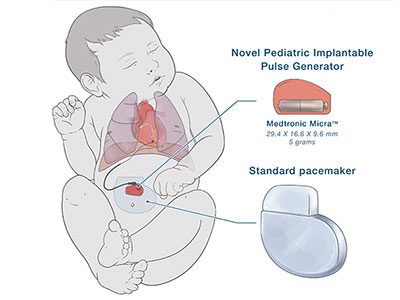
A pacemaker modified in a novel way to work better for the smallest children, including newborns, is safe and effective to stabilize heart rhythms for at least two years, according to a study published in Circulation: Arrhythmia and Electrophysiology, a journal of the American Heart Association.
The study includes the findings from 29 infants who received the novel pediatric pacemaker, which is no bigger than a AAA battery, at multiple institutions in the United States. A majority of them (79%) were born premature, weighing less than five pounds (2.3 kg).
The devices remain stable, with effective pacing, normal electrical parameters and battery longevity aligned with projections for up to two years. This design and application provides a viable alternative to standard-size generators and addresses a vital unmet need for these small patients. In fact, though the study includes data from the first 29 cases, the number of children who have received these devices across the United States today has doubled to nearly 60.
The specially modified pediatric-sized implantable pacemaker includes a Medtronic Micra sub-assembly that connects to an epicardial lead. While this makes the leadless pacemaker into one that uses leads, the resulting device is significantly smaller than any commercially available pacemaker previously on the market in the U.S.
The novel pediatric implantable pulse generator is about a quarter of the size of a traditional pacemaker.
Why it matters
“The need for an urgent permanent pacemaker in newborns is quite rare, but when needed, it is often an emergency,” said lead author Charles Berul, MD, a cardiologist and electrophysiologist at Children’s National Hospital in a press release from the American Heart Association. “Babies who were very small often cannot get a permanent pacemaker and must undergo multiple temporary pacing wires or other techniques in the hopes of getting them big enough to undergo a standard pacemaker placement.”
Dr. Berul also notes that a smaller pacemaker may also help frail elderly patients and be a better choice for some children and adults.
What’s next: Better delivery
Innovating smaller devices is a good start. However, when a newborn or young child needs any pacemaker or defibrillator, they face open chest surgery. Their arteries and veins are just too small for even the smallest size transvenous pacemaker catheter.
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital.
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital. Dr. Rokita is a cancer genomics leader with 20 years of combined research experience in academia, industry and the government. She’s also a technical and analytical expert in genomics research using microarrays and high-throughput sequencing.
“We are very excited that we were able to recruit Dr. Rokita as director of the Bioinformatics Core Facility,” says Muller Fabbri, MD, PhD, associate center director for Cancer and Immunology Research at Children’s National. “Her Bioinformatics Core will play a central role in providing the Brain Tumor Institute community with unique expertise spanning biology/genetics/genomics and bioinformatics and will propel Children’s National forward as a national and worldwide leader in pediatric brain tumor research.”
Dr. Rokita is overseeing the core’s creation, including bringing both bioinformatics staff and computing infrastructure to the program, which will support the data analysis needs of the institute’s investigators. She recently answered questions about the new core and also talked a little bit about the focus of her own research that will continue at Children’s National.
Q: Why is the Brain Tumor Institute establishing a Bioinformatics Core?
A: Growing the institute’s bioinformatics capabilities was one of the things that leadership wanted to make sure was built into the plan for the record-setting $96 million gift that was received in 2023. There was a clear need among the principal investigators for this type of research support which includes organization, analysis and interpretation of large-scale genetic sequencing and other “-omics” data.
Q: How did you decide to join Children’s National?
A: I was leading a pediatric brain tumor focused bioinformatics team at Children’s Hospital of Philadelphia (CHOP). As a part of the Children’s Brain Tumor Network (CBTN), I worked closely with a collaborator from Children’s National, Brian Rood, MD, medical director of the Brain Tumor Institute. He told me about the opportunity and I was very excited to apply.
Q: How did your previous work prepare you for this role?
A: I’ve spent the past 10 years in the pediatric cancer field with the last six focused on brain tumor research. In my various roles at CHOP, I led multiple large-scale genomic analysis efforts, comprehensive data and methods for which we then provided openly to the community. During my postdoctoral fellowship, these efforts included a large neuroblastoma patient-derived cell line “ENCODE” as well as a resource led in collaboration with multiple institutes and the National Cancer Institute funded by Alex’s Lemonade Stand Foundation (ALSF). We further scaled these efforts to build open analytical platforms to empower researchers to build upon our work doing their own cancer genomic analysis. In collaboration with the Childhood Cancer Data Lab at ALSF, we built the platform that ultimately ballooned into the OpenPedCan includes large amounts of harmonized genomic, epigenomic and proteomic data for patients with pediatric cancer. What’s unique is that the data is all processed in the same way and easily accessible through multiple mechanisms. Researchers can use these data to ask questions about the cancer type they study or genes of interest. For example, genes over-expressed, absent and/or mutated in a specific tumor subtype may lead to a better understanding of how a patient’s cancer may respond to a treatment.
We’ll be bringing some of the workflows we created previously here to Children’s National, and that will allow us to join newly generated internal data with the thousands of data points we’ve already harmonized using these workflows.
Q: Can you give us some examples of how data harmonization benefits the field of pediatric brain tumor research?
A: Harmonizing across institutions and databases will help us increase the number of data points available for study. This is really important for rare types of tumors and are major foci of institute collaborator Adriana Fonseca, MD, and her International Rare Brain Tumor Registry program. The Bioinformatics Core will support data organization and analysis for this effort, which aims to sequence the rarest brain tumors — those that make up between only 3% and 5% of all brain tumors. If all the data is analyzed the same way, we can combine multiple studies to increase our total dataset, which in turn may reveal new biomarkers and new subtypes of those tumors. It is critical that we continue to build these data resources in a way that they can be accessed by everyone doing this work. Having dedicated support systems for these functions will push the research farther, faster.
Q: As this work gets underway, what is the core’s main function?
A: As this initiative gets underway, the Bioinformatics Core’s primary goal is to empower investigators by streamlining and centralizing data analyses. We help researchers transfer sequencing data into secure cloud storage, organize newly generated records and prepare those datasets for in-depth study. Our bioinformatics scientists then perform downstream analyses to address the specific questions posed by each investigator. On the backend, we collaborate with information technology at Children’s National to develop a robust infrastructure that supports these activities efficiently. By offering these services in-house, we aim to ensure our investigators have seamless, comprehensive support—ultimately driving innovation and accelerating research progress.
Q: What is “open science” and why is it important in bioinformatics?
A: One of our big focus areas is open science, meaning our goal is to push data and code out into the community so that researchers can easily reproduce and build upon our findings. I’m excited to bring the principles of open science, code sharing and data sharing to the Bioinformatics Core.
Making resources open makes it easier for teams to work together across institutions and research programs. It is also going to benefit patients because people can reuse the code and move towards cures faster. For example, we try to package an entire manuscript’s code when we provide our data so it’s clear how the analyses were done.
Q: What is your particular research passion?
A: I work in several research areas and with many brilliant collaborators. One of our focus areas is understanding how RNA splicing can contribute to pediatric brain tumors to create a change in a protein. We have recently identified tumor-specific splice events in some pediatric brain tumor types and will be partnering with Dalia Haydar, PharmD, PhD, to create therapeutic approaches to targeting these. We are also developing a user-friendly application for mining the large amount of splicing data in pediatric brain tumors.
Another focus of our lab is understanding how the patient’s host genome (alterations inherent in their blood DNA) influences the tumor’s genetics. For example, we’ve just preprinted a study connecting inherited variants to tumor genetics and patient outcomes.
Finally, we are interested in how differences in race, ethnicity and social determinants of health influence survival and treatment outcomes for children with brain tumors.
I am passionate about data sharing, code reproducibility and promoting open science in general.
Q: Is there any specific reason you decided to focus your work around brain tumors and pediatric brain tumors?
A: My cousin passed away from a brain tumor when I was in high school. They didn’t have molecular diagnosis then, but he had a brainstem glioma, likely a diffuse midline glioma. In graduate school, I studied addiction genetics and became fascinated with the brain and towards the end, cancer. As an alumna of Penn State, I was actively involved in philanthropic events raising money for their Dance MaraTHON supporting children with cancer. I was lucky to land a postdoc at CHOP and lean into subsequent roles which allowed my passion for this field to grow.
Q: Last question — What do you do with your time when you are not studying pediatric brain tumor data?
A: I enjoy being with my family, observing my children learn and grow, and listening to music.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/bioinformatics-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-02-26 16:09:002025-03-06 13:18:03Q&A with Dr. Rokita: Building bioinformatics infrastructure at the Brain Tumor Institute
In December of 2024, a team that included experts from Children’s National Hospital traveled to Uganda to continue work on a pilot program applying artificial intelligence (AI) to the diagnosis of rheumatic heart disease (RHD). Ugandan health care providers have been trained and equipped to acquire echocardiograms for their patients but lack expertise in consistently being able to diagnose RHD by detecting leaky heart valves. The team created a tool that uses AI to predict RHD by identifying leaky heart valves on handheld ultrasound devices, then prompts a referral for a full echocardiogram.
The goal is to find ways to help people in Uganda diagnose RHD early, before a patient is in need of surgery, and initiate antibiotics so their heart can return to normal. The team of researchers, including fellow Kelsey Brown, MD, helped to implement additional steps toward this goal in December. According to Dr. Brown, the results were excellent. After four days of seeing patients, over 450 people were screened. The AI tool has an 86% accuracy rating. After returning from Uganda, the research team plans to work on the AI tool and further improve its accuracy rating. Eventually, the vision is that this tool can roll out on a larger scale for more places around the world to access it.
Craig Sable, MD, Marius Linguraru, DPhil, MA, MSc, and Pooneh Roshanitabrizi, PhD, from our Sheikh Zayed Institute, who developed the AI algorithms, worked in partnership with the Rheumatic Heart Disease Research Collaborative (RRCU) in Uganda. This trip was also made possible thanks to a grant funded through the Children’s National Global Health Initiative. Special thank you to our AI partner, US2.AI, who made the deployment of the AI models onto a tablet that provided real-time results, possible.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/RHD-AI-Uganda-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2025-02-26 10:43:202025-05-06 13:49:45Children’s National brings AI into the RHD early diagnosis equation
The course attracts a national audience and brings together neuroscience clinicians and pediatricians in the Washington, D.C. and Mid-Atlantic region.
Guest speakers include Annapurna Poduri, MD, MPH, Deputy Director for NINDS, Emily Freilich, MD, from the FDA and Conor Mallucci, MBBS, Chief of Neurosurgery at Alder Hays, England.
This year’s course highlights 3 major areas:
Updates in Epilepsy
Innovations in Vascular Neurosurgery and Neurointerventional Radiology
Addressing Mental and Behavioral Health in Neurological Conditions
We invite you to join us for presentations from experts in the field during this full-day, CME accredited event on April 10, 2025. This is a hybrid event that will be held virtually or in-person at the Children’s National Research & Innovation Campus.





































 The Divisions of Neurology and Neurosurgery at Children’s National Hospital are proud to host the 35th Annual Pediatric Neurology Update course.
The Divisions of Neurology and Neurosurgery at Children’s National Hospital are proud to host the 35th Annual Pediatric Neurology Update course.