Mitochondria are the cell’s powerplants and inside them the MTP enzymatic complex catalyzes three steps in beta-oxidation of long-chain fatty acids.
In one family, genetic lightning struck twice. Two sisters were diagnosed with mitochondrial trifunctional protein (MTP) deficiency. This is a rare condition that stops the body from converting fats to energy, which can lead to lactic acidosis, recurrent breakdown of muscle tissue and release into the bloodstream (rhabdomyolysis), enlarged heart (cardiomyopathy) and liver failure.
Mitochondria are the cell’s powerplants and inside them the MTP enzymatic complex catalyzes three steps in beta-oxidation of long-chain fatty acids. MTP deficiency is so rare that fewer than 100 cases have been reported in the literature says Hostensia Beng, M.D., who presented an MTP case study during the American Society of Nephrology’s Kidney Week.
The 7-month-old girl with known MTP deficiency arrived at Children’s National lethargic with poor appetite. Her laboratory results showed a low corrected serum calcium level, elevated CK level and protein in the urine (proteinuria) at a nephrotic range. The infant was treated for primary hypoparathyroidism and rhabdomyolysis.
Even though the rhabdomyolysis got better, the excess protein in the girl’s urine remained at worrisome levels. A renal biopsy showed minimal change disease and foot process fusion. And electron microscopy revealed shrunken, dense mitochondria in visceral epithelial cells and endothelium.
“We gave her tacrolimus, a calcineurin inhibitor that we are well familiar with because we use it after transplants to ensure patient’s bodies don’t reject the donated organ. By eight months after treatment, the girl’s urine protein-to-creatinine (uPCR) ratio was back to normal. At 35 months, that key uPCR measure rose again when tacrolimus was discontinued. When treatment began again, uPCR was restored to normal levels one month later,” Dr. Beng says.
The girl’s older sister also shares the heterozygous deletion in the HADHB gene, which provides instructions for making MTP. That missing section of the genetic how-to guide was predicted to cause truncation and loss of long-chain-3-hydroxyacl CoA dehydrogenase function leading to MTP deficiency.
“Renal involvement has been reported in only one patient with MTP deficiency to date, the older sister of our patient,” Dr. Beng adds.
Podocytes are specialized cells in the kidneys that provide a barrier, preventing plasma proteins from leaking into the urine. Podocytes, however, need energy to function and are rich in mitochondria.
“The proteinuria in these two sisters may be related to their mitochondrial dysfunction. Calcineurin inhibitors like tacrolimus have been reported to reduce proteinuria by stabilizing the podocyte actin cytoskeleton. Tacrolimus was an effective treatment for our patient, who has maintained normal renal function, unlike her sister,” Dr. Beng says.
American Society of Nephrology’s Kidney Week presentation
“Treatment of nephrotic-range proteinuria with tacrolimus in mitochondrial trifunctional protein deficiency
Hostensia Beng, M.D., lead author; Asha Moudgil, M.D., medical director, transplant, and co-author; Sun-Young Ahn, M.D., MS, medical director, nephrology inpatient services, and senior author, all of Children’s National Health System.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/08/mitochondria.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-02-05 09:36:322024-11-08 13:36:20Treating nephrotic-range proteinuria with tacrolimus in MTP
For an elementary school art project, Michael H. Hsieh, M.D., Ph.D., was instructed to fashion a coat of arms out of clay. In addition to panels for truth, justice and Taiwan, in the shield’s M.D. panel, a snake twists around a rod, like the staff for Asclepius, a Greek god associated with healing.
Children’s urologistMichael H. Hsieh, M.D., Ph.D., knew from age 10 that he would become a doctor. Proof is at his parents’ home. For an elementary school art project, students were instructed to fashion a coat of arms out of clay. In addition to panels for truth, justice and Taiwan, in the shield’s M.D. panel, a snake twists around a rod, like the staff for Asclepius, a Greek god associated with healing.
“I liked science. When I can use it to help patients, that is very rewarding,” says Dr. Hsieh, the first doctor in his family.
These days, Dr. Hsieh’s Twitter profile serves as a digital coat of arms, describing him as “tinker, tailor,” #UTI#biologist, epithelial #immunologist, helminthologist and #urologist.
Tinker/tailor is shorthand for the mystery drama, “Tinker Tailor Solider Spy,” he explains, adding that the “tinker” part also refers “to the fact that I am always questioning things, and science is about experimentation, trying to seek answers to questions.”
While still in medical school during a rotation Dr. Hsieh saw a bladder operation on a young child and thought it was “amazing.” That experience in part inspired Dr. Hsieh to become a urologist and bladder scientist. His training in immunology and study of the bladder naturally led him to study urinary tract infections and parasitic worms that affect the urinary tract. In addition, thanks to R01 funding from the National Institutes of Health (NIH), Dr. Hsieh is co-principal investigator with Axel Krieger, University of Maryland, and Jin U. Kang, Johns Hopkins, on a project to develop imaging robots for supervised autonomous surgery on soft tissue.
The $1 million in NIH funding pushes the boundaries on amazing by using multi-spectral imaging technology and improved techniques to reduce surgical complications.
Anastomosis is a technique used by surgeons to join one thing to another, whether it’s a vascular surgeon suturing blood vessels, an orthopedic surgeon joining muscles or a urologist stitching healthy parts of the urinary tract back together. Complications can set in if their stitching is too tight, prompting scar tissue to form, or too loose, letting fluid seep out.
“The human eye can see a narrow spectrum of electromagnetic radiation. These multi-spectral imaging cameras would see across greater set of wavelengths,” he says.
The project has three aims: figuring out the best way to place sutures using multi-spectral imaging, accurately tracking soft tissue as they model suturing and comparing the handicraft of a robot against anastomosis hand-sewn by surgeons.
“I like challenges, and I like new things. I am definitely not interested in doing permutations of other people’s work,” Dr. Hsieh explains. “I would much rather go on a path that hasn’t been tread. It is more difficult in some ways, but on a day-to-day basis, I know I am making a contribution.”
In another innovative research project, Dr. Hsieh leveraged a protein secreted by a parasitic worm, Schistosoma haematobium, that suppresses inflammation in hosts as a new therapeutic approach for chemotherapy-induced hemorrhagic cystitis, a form of inflammation of the bladder.
Watching his first surgery nearly 30 years ago, he had no idea robots might one day vie to take over some part of that complicated procedure, or that parasite proteins could be harnessed as drugs. However, he has a clear idea which innovations could be on the horizon for urology in the next three decades.
“My hope is 30 years from now, we will have a solid UTI vaccine and more non-antibiotic therapies. UTIs are the second-most common bacterial infection in childhood and, in severe cases, can contribute to kidney failure,” he says.
Globally, parasitic worms pose an ongoing challenge, affecting more than 1 billion worldwide – second only to malaria. People persistently infected by schistosome worms fail to reach their growth potential, struggle academically and lack sufficient energy for exercise or work.
“There is a feeling that the infection prevalence might be decreasing globally, but not as quickly as everyone hopes. In 30 years perhaps with more mass drug administration and additional drugs – including a vaccine – we’ll have it close to eliminated globally. It would become more like polio, casting a slim shadow with small pockets of infection here or there, rather than consigning millions to perpetual poverty.”
The Children’s commentators point to the “extremely dangerous” combination of “the small curious hands of a young child” and “the easily accessible and operable, loaded handgun” and suggest that pediatricians who counsel families about safely storing weapons tailor messaging to the weapon type and the family’s reason for owning a firearm.
Paradoxically, as overall firearm ownership decreased in U.S. households with young children from 1976 to 2016, the proportion of these families who owned handguns increased. This shift in firearm preferences over decades from mostly rifles to mostly handguns coincided with increasing firearm-mortality rates in young children, researchers report Jan. 28, 2019, in Pediatrics.
“Almost 5 million children live in homes where at least one firearm is stored loaded and unlocked,” Kavita Parikh, M.D., a pediatric hospitalist at Children’s National Health System, and co-authors write in an invited commentary. “This study is a loud and compelling call to action for all pediatricians to start open discussions around firearm ownership with all families and share data on the significant risks associated with unsafe storage. It is an even louder call to firearm manufacturers to step up and innovate, test and design smart handguns, inoperable by young children, to prevent unintentional injury,” Dr. Parikh and colleagues continue.
The Children’s commentators point to the “extremely dangerous” combination of “the small curious hands of a young child” and “the easily accessible and operable, loaded handgun” and suggest that pediatricians who counsel families about safely storing weapons tailor messaging to the weapon type and the family’s reason for owning a firearm.
They also advocate for childproofing firearms stored in the home – through free or discounted locks, storing weapons separately from ammunition, and using personalized technology that limits the firearm’s potential to be used by children accidentally. According to a retrospective, cross-sectional study led by Children’s researchers, younger children are more likely to be shot by accident.
“The development of effective safety controls on firearms is not only attainable but could be the next big step towards reducing mortality, especially among our youngest. We as a society should be advocating for continued research to ‘childproof’ firearms so that if families choose to have firearms in the home, the safety of their children is not compromised,” Dr. Parikh and co-authors write.
In addition to Dr. Parikh, the senior author, the Pediatrics commentary co-authors include Lead Author Shilpa J. Patel M.D., MPH, emergency medicine specialist; and co-author Monika K. Goyal M.D., MSCE, assistant division chief and director of research in Children’s Division of Emergency Medicine.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/little-boy-looking-at-gun.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-28 10:08:092019-07-19 10:55:16A ‘compelling call’ for pediatricians to discuss firearm safety
Research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that genetic mutations that cause cleft lip and palate also may contribute to neural tube defects, such as spina bifida.
Oral clefts are some of the most common birth defects worldwide, affecting about one in every 700 births. In the U.S., more than 4,000 babies are born each year with cleft lip, with or without cleft palate.
This defect isn’t simply a cosmetic manner: Oral clefts can severely affect feeding, speech and hearing, and they cause about 3,300 deaths annually worldwide.
To better understand these conditions, researchers have isolated a number of genetic mutations that appear to play contributing roles. These include those in a gene known as Interferon Regulatory Factor 6. New research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that these mutations also may contribute to neural tube defects such as spina bifida.
In the first weeks of fetal development, the neural plate curves, creating a neural tube that, once fused shut, becomes the fetal brain and fetal spinal cord. Neural tube defects, which can range from mild to severe, are characterized by incomplete development of the brain, spinal cord or meninges. These defects can potentially result in paralysis or even fetal or neonatal demise. According to the National Institutes of Health, spina bifida, which affects the spinal cord, is the most common neural tube defect in the U.S., affecting up to 2,000 infants each year.
“Despite its high frequency, spina bifida remains among the least understood structural birth defects,” says Brian C. Schutte, an associate professor of Microbiology and Molecular Genetics, Pediatrics and Human Development at Michigan State University and the study’s senior author. “There is strong evidence that genetic factors are a leading cause of such structural birth defects, but in most cases, the cause is unknown. Our team’s study is the first published research to demonstrate that DNA variants in the gene IRF6 can cause spina bifida,” Schutte says.
What’s more, the research team identified a mechanism to explain how altering IRF6 leads to neural tube defects. This mechanism links IRF6 function to two other genes – known as transcription Factor AP2A (TFAP2A) and Grainyhead Like 3 (GRHL3) – that are also known to be required for the development of the neural tube, lip and palate.
“We’re all on the hunt for the reasons when, how and why birth defects happen,” adds Youssef A. Kousa, MS, D.O., Ph.D., a clinical fellow in the Division of Child Neurology at Children’s National Health System and the study’s lead author. “Our main goal is prevention. This paper is a significant development because our team has identified a group of genes that can potentially contribute to very common types of birth defects: craniofacial as well as neural tube defects.”
The scientific odyssey is a wonderful example of serendipity. Kousa, then working in Schutte’s lab, was studying the effects of a new mutant experimental model strain on development of the palate. But one day, he walked into Schutte’s office holding a deformed preclinical embryo and said: “Brian, look at this!”
“Weird things happen in biology,” Schutte replied and counseled him to return if it happened again. Less than two weeks later, Kousa was back with several more of the deformed preclinical embryos, saying: “OK, Brian. It happened again.”
Within hours Kousa had unearthed recently published research that included an image of a similarly affected preclinical embryo. The pair then sketched out possible intersecting genetic pathways, as they brainstormed the myriad ways to end up with that specific phenotype. Initially, they tested their hypotheses in experimental models and eventually corroborated findings through human genetic studies.
The human studies could only be performed by collaborations. Schutte shared their initial observations with human genetics researchers scattered across the country. Those labs then generously agreed to test whether DNA variants in IRF6 were associated with neural tube defects in samples from patients that they had collected over decades of research.
The team found that Tfap2a, Irf6 and Grhl3 are components of a gene regulatory network required for neurulation, a folding process that results in the neural tube bending and then fusing to become the basis of the embryo’s nervous system, from brain to spinal cord.
“Since this network is also required for formation of the lip, palate, limbs and epidermis, which develop at different times and places during embryogenesis, we suggest that the Tfap2a–Irf6–Grhl3 network is a fundamental pathway for multiple morphogenetic processes,” the researchers write.
Interferon Regulatory Factor 6 functions best when there is neither too much expression nor too little. Overexpression of Irf6 suppresses Transcription Factor Activation Protein 2A and Grainyhead Like 3, causing exencephaly, a neural tube defect characterized by the brain being located outside of the skull. Counterintuitively, experimental models that had too little Irf6 also ended up with reduced levels of Tfap2a and Grhl3 that led to a structural birth defect, but at the opposite end of the neural tube.
To test whether the experimental model findings held true in humans, they sequenced samples from people who had spina bifida and anencephaly – the rare birth defect that Kousa spotted in the experimental models – and found IRF6 function was conserved in people. Because of the genetic complexity of these birth defects, and the challenges inherent in collecting samples from cases of severe birth defects, many research teams were invited to participate in the study.
As testament to their collegiality, researchers from Stanford University, University of Texas at Austin, University of Iowa, University of Texas at Houston and Duke University agreed to share precious samples from the California Birth Defects Monitoring Program, from the Hereditary Basis of Neural Tube Defects study and from their own institutional sample collections.
“As we get better at personalized medicine, we could use this information to one day help to counsel families about their own risk and protective factors,” Kousa adds. “If we can identify the genetic pathway, we might also be able to modify it to prevent a birth defect. For example, prenatal supplementation with folic acid has led to a decrease in babies born with neural tube defects, but not all neural tube defects are sensitive to folic acid. This knowledge will help us develop individual-based interventions.”
Financial support for the research covered in this post was provided by the National Institutes of Health under grants DE13513, F31DE022696, DE025060, P01HD067244 and GM072859; startup funding from Michigan State University and the UT-Health School of Dentistry in Houston; and the Centers for Disease Control and Prevention under award number 5U01DD001033.
In addition to Kousa and Schutte, study co-authors include Huiping Zhu, Yunping Lei and Richard H. Finnell, University of Texas at Austin; Walid D. Fakhouri, University of Texas Health Science Center at Houston; Akira Kinoshita, Nagasaki University; Raeuf R. Roushangar, Nicole K. Patel, Tamer Mansour, Arianna L. Smith, and Dhruv B. Sharma, Michigan State University; A.J. Agopian and Laura E. Mitchell, University of Texas School of Public Health; Wei Yang and Gary M. Shaw, Stanford University School of Medicine; Elizabeth J. Leslie, Emory University; Xiao Li, Tamara D. Busch, Alexander G. Bassuk and Brad A. Amendt, University of Iowa; Edward B. Li and Eric C. Liao, Massachusetts General Hospital; Trevor J. Williams, University of Colorado Denver at Anschutz Medical Campus; Yang Chai, University of Southern California; and Simon Gregory and Allison Ashley-Koch, Duke University Medical Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/little-girl-with-spina-bifida.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-25 12:58:112024-12-30 12:46:57Oral clefts may stem from a shared genetic cause as neural tube defects
According to Children’s research presented during the Institute for Healthcare Improvement 2018 Scientific Symposium, standardizing feeding practices – including the timing for fortifying breast milk and formula with essential elements like zinc and protein – improves growth trends for the tiniest preterm infants.
About 1 in 10 infants is born before 37 weeks gestation. These premature babies have a variety of increased health risks, including deadly infections and poor lung function.
Emerging research suggests that getting their length and weight back on track could help. According to Children’s research presented during the Institute for Healthcare Improvement 2018 Scientific Symposium, standardizing feeding practices – including the timing for fortifying breast milk and formula with essential elements like zinc and protein – improves growth trends for the tiniest preterm infants.
The quality-improvement project at Children’s National Health System targeted very low birth weight infants, who weigh less than 3.3 pounds (1,500 grams) at birth. These fragile infants are born well before their internal organs, lungs, brain or their digestive systems have fully developed and are at high risk for ongoing nutritional challenges, health conditions like necrotizing enterocolitis (NEC) and overall poor development.
The research team measured progress by tracking the micro-preemies’ mean delta weight Z-score for weight gain, which measures nutritional status.
“In this cohort, mean delta weight Z-scores improved by 43 percent, rising from -1.8 to the goal of -1.0, when we employed an array of interventions. We saw the greatest improvement, 64 percent, among preterm infants who had been born between 26 to 28 weeks gestation,” says Michelande Ridoré, MS, Children’s NICU quality-improvement program lead who presented the group’s preliminary findings. “It’s very encouraging to see improved growth trends just six months after introducing these targeted interventions and to maintain these improvements for 16 months.”
Within Children’s neonatal intensive care unit (NICU), micro-preemies live in an environment that mimics the womb, with dimmed lighting and warmed incubators covered by blankets to muffle extraneous noise. The multidisciplinary team relied on a number of interventions to improve micro-preemies’ long-term nutritional outcomes, including:
Reducing variations in how individual NICU health care providers approach feeding practices
Fortifying breast milk (and formula when breast milk was not available), which helps these extra lean newborns add muscle and strengthen bones
Early initiation of nutrition that passes through the intestine (enteral feeds)
Re-educating all members of the infants’ care teams about the importance of standardized feeding and
Providing a decision aid about feeding intolerance.
Dietitians were included in the daily rounds, during which the multidisciplinary team discusses each infant’s care plan at their room, and used traffic light colors to describe how micro-preemies were progressing with their nutritional goals. It’s common for these newborns to lose weight in the first few days of life.
Infants in the “green” zone had regained their birth weight by day 14 of life and possible interventions included adjusting how many calories and protein they consumed daily to reflect their new weight.
Infants in the “yellow” zone between day 15 to 18 of life remained lighter than what they weighed at birth and were trending toward lower delta Z-scores. In addition to assessing the infant’s risk factors, the team could increase calories consumed per day and add fortification, among other possible interventions.
Infants in the “red” zone remained below their birth weight after day 19 of life and recorded depressed delta Z-scores. These infants saw the most intensive interventions, which could include conversations with the neonatologist and R.N. to discuss strategies to reverse the infant’s failure to grow.
Future research will explore how the nutritional interventions impact newborns with NEC, a condition characterized by death of tissue in the intestine. These infants face significant challenges gaining length and weight.
Institute for Healthcare Improvement 2018 Scientific Symposium presentation
“Improved growth of very low birthweight infants in the neonatal intensive care unit.”
Caitlin Forsythe, MS, BSN, RNC-NIC, NICU clinical program coordinator, Neonatology, and lead author; Michelande Ridoré, MS, NICU quality-improvement program lead; Victoria Catalano Snelgrove, RDN, LD, CNSC, CLC, pediatric clinical dietitian; Rebecca Vander Veer, RD, LD, CNSC, CLC, pediatric clinical dietitian; Erin Fauer, RDN, LD, CNSC, CLC, pediatric clinical dietitian; Judith Campbell, RNC, IBCLC, NICU lactation consultant; Eresha Bluth, MHA, project administrator; Anna Penn, M.D., Ph.D., neonatologist; Lamia Soghier, M.D., MEd, Medical Unit Director, Neonatal Intensive Care Unit; and Mary Revenis, M.D., NICU medical lead on nutrition and senior author; all of Children’s National Health System.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/10/PreemieImage-e1494013414625.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-23 11:33:392024-02-02 14:39:31Getting micro-preemie growth trends on track
Clinicians suspect that taking probiotics, such as lactobacillus supplements, and making changes to diet may prevent urinary diseases that occur commonly among pediatric patients. A research team led by Children’s faculty is exploring whether changes in the built environment also affect the urinary microbiome.
Emerging evidence suggests that the variety and volume of bacteria that reside in the bladder – the urinary microbiome – significantly impact whether people’s genitourinary systems remain healthy or become susceptible to disease.
Already, clinicians suspect that taking probiotics and making changes to diet may prevent urinary diseases that occur commonly among pediatric patients. A research team led by Children’s faculty is exploring whether changes in the built environment also affect the urinary microbiome.
Using experimental models, they looked at how stable the urinary microbiome was over time. Then, they measured the potential effect of changing the built environment on the urinary microbiome of preclinical models.
They did this by following six C57BL/6 experimental models for five months, starting from when they were nine weeks old. They collected urine specimens when the study began and repeated sample collections each month. The multidisciplinary team isolated microbial DNA from these specimens to determine the makeup of the bacterial community present in their urinary tracts.
All of the experimental models shared a single cage, drank the same water and ate the exact same chow. At four months, however, they moved the preclinical models to a different facility within the same county. Their chow and bedding remained unchanged, but the water source changed since they received tap water at both locations.
“There were no changes in the proportion of specific bacteria in the urinary microbiomes from month zero through month five, which means the urinary microbiomes of healthy experimental models remain stable over time,” says Michael Hsieh, M.D., Ph.D., a urologist at Children’s National Health System and senior author of the work presented during the Pediatric Urology Fall Conference. “However, the convergence of the Shannon Diversity Index, the clustering seen on Principal coordinate analyses and changes in functional analyses taken as a whole suggest that an overall shift of the urinary microbiome occurred due to a change in the physical environment.”
This work suggests that where patients live could influence which bacteria grow in the urinary tracts, including during urinary tract infections.
The Societies for Pediatric Urology’s Pediatric Urology Fall Conference
“Effects of time and the built environment on the stability of the mouse urinary microbiome: implications for clinical utility.”
Catherine S. Forster, M.D., MS, pediatric hospitalist, Children’s National; James Cody, Ph.D., Biomedical Research Institute; Nirad Banskota, MS, Biomedical Research Institute; Crystal Stroud, MS, Children’s National; Ljubica Caldovic, Ph.D., principal investigator, Children’s National; and Michael Hsieh, M.D., Ph.D., urologist, Children’s National.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/Probiotic-Lactobacillis-Bacteria.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-18 11:52:212019-04-22 09:56:13Does ZIP code factor into genitourinary system health?
Patients with spinal cord injuries nearly universally have bacteria present in their urine regardless of whether they have a urinary tract infection.
The fallout from spinal cord injury doesn’t end with loss of mobility: Patients can have a range of other issues resulting from this complex problem, including loss of bladder control that can lead to urine retention. One of the most serious implications is urinary tract infections (UTIs), the most common cause of repeat hospitalization in people with spinal cord injuries, explains Hans G. Pohl, M.D., associate chief in the division of Urology at Children’s National Health System.
Diagnosing UTIs in people with spinal cord injuries is trickier than in people who are otherwise healthy, Dr. Pohl explains. Patients with spinal cord injuries nearly universally have bacteria present in their urine regardless of whether they have a UTI. It’s unclear whether these bacteria are innocent bystanders or precursors to UTIs in patients who don’t yet show symptoms. And although antibiotics can wipe out this bacterial population, these drugs can have undesirable side effects and frequent use can promote development of antibiotic-resistant bacteria.
Although clinical dogma has long promoted the idea that “healthy” urine is sterile, Dr. Pohl and colleagues have shown that a variety of bacteria live in urine, even in people without symptoms. These microorganisms, like the intestinal microbiome, live in harmony with their hosts and may even help promote health. However, it’s unclear what this urinary microbiome might look like for patients with spinal cord injury before, during and after UTIs.
To start investigating this question, Dr. Pohl and co-authors recently reported a case study they published online Sept. 21, 2018, in Spinal Cord Series and Cases. The case report about a 55-year-old man who had injured the thoracic segment of his spinal cord—about the level of the bottom of his shoulder blades—in a skiing accident when he was 19 was selected as “Editor’s Choice” for the journal’s October 2018 issue. The patient had a neurogenic bladder, which doesn’t function normally due to impaired communication with the spinal cord. To compensate for this loss of function, this patient needed to have urine removed every four to six hours by catheterization.
Over eight months Dr. Pohl, the study’s senior author, and colleagues collected 12 urine samples from this patient:
One was collected at a time the patient didn’t show any symptoms of a UTI
Nine were collected when the patient had UTI symptoms, such as bladder spasticity
Two samples were collected when the patient had finished antibiotic treatment for the UTI.
The researchers split each sample in half. One part was put through a standard urinalysis and culture, much like what patients with a suspected UTI would receive at the doctor’s office. The other part was analyzed using a technique that searched for genetic material to identify bacteria that might be present and to estimate their abundance.
The researchers found a variety of different bacteria present in these urine samples. Regardless of the patient’s health status and symptoms, the majority of these bacterial species are known to be pathogenic or potentially pathogenic. By contrast, this patient’s urine microbiome appeared to largely lack bacterial species known to be either neutral or with potentially probiotic properties, such as Lactobacillus.
All of the bacteria that grew in culture also were identified by their genetic material in the samples. However, genetic sequencing also identified a possible novel uropathogenic species called Burkholderia fungorum that didn’t grow in the lab in five of the samples. This bacterium is ubiquitous in the environment and has been identified in soil- and plant-based samples. It also has been discovered in the respiratory secretions of patients with cystic fibrosis, in patients with a heart condition called infectious endocarditis, in the vaginal microbiota of patients with bacterial vaginosis, and in the gut of patients with HIV who have low T-cell counts. Dr. Pohl says it’s unclear whether this species played an infectious role in this patient’s UTI or whether it’s just part of his normal urine flora.
“Consistent with our previous work, this case report demonstrates that rather than healthy urine being sterile, there is a diverse urine bacterial ecosystem during various states of health and disease,” Dr. Pohl says. “Rather than UTIs resulting from the growth or overgrowth of a single organism, it’s more likely that a change in the healthy balance of the urine ecosystem might cause these infections.”
By monitoring the relative abundance of different bacteria types present in the urine of patients with spinal cord injury and combining this information with a patient’s symptoms, Dr. Pohl says doctors may be able to make more accurate UTI diagnoses in this unique population.
In addition to Dr. Pohl, study co-authors include Marcos Pérez-Losada, Ljubica Caldovic, Ph.D., Bruce Sprague and Michael H. Hsieh, M.D., Children’s National; Emma Nally, Suzanne L. Groah and Inger Ljungberg, MedStar National Rehabilitation Hospital; and Neel J. Chandel, Montefiore Medical Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/E-coli-bacteria.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-17 10:58:092024-05-29 09:09:16Urinary bacteria in spinal cord injury cases may tip balance toward UTIs
Over the past several decades, it’s become increasingly recognized that perinatal mood and anxiety disorders (PMADs), including postpartum depression, are more than just “baby blues.” They’re the most common complication of childbirth in the U.S., affecting about 14 percent of women in their lifetimes and up to 50 percent in some specific populations. PMADs can lead to a variety of adverse outcomes for both mothers and their babies, including poor breastfeeding rates, poor maternal-infant bonding, lower infant immunization rates and maternal suicides that account for up to 20 percent of postpartum deaths.
But while it’s obvious that PMADs are a significant problem, finding a way to solve this issue is far from clear. In a policy statement published December 2018 in the journal Pediatrics, the American Academy of Pediatrics recommends that pediatric medical homes coordinate more effectively with prenatal providers to ensure PMAD screening occurs for new mothers at well-child checkups throughout the first several weeks and months of infancy and use community resources and referrals to ensure women suffering with these disorders receive follow-up treatment.
To help solve the huge issue of PMADs requires a more comprehensive approach, suggests Lenore Jarvis, M.D., MEd, an emergency medicine specialist at Children’s National Health System. A poster that Dr. Jarvis and colleagues from Children’s Perinatal Mental Health Taskforce recently presented at the American Academy of Pediatrics 2018 National Convention and Exhibit in Orlando, Florida, details the integrated care to help women with PMADs that originated at Children’s National and is being offered at several levels, including individual, interpersonal, organizational, community and policy. The poster was ranked best in its section for the Council on Early Childhood.
At the base level of care for mothers with possible PMADs, Dr. Jarvis says, are the one-on-one screenings that take place in primary care clinics. Currently, all five of Children’s primary care clinics screen for mental health concerns at annual visits. At the 2-week, 1-, 2-, 4- and 6-month visits, mothers are screened for PMADs using the Edinburgh Postnatal Depression Scale, a validated tool that’s long been used to gauge the risk of postpartum depression. In addition, recent studies at Children’s neonatal intensive care unit (NICU) and emergency department (ED) suggest that performing PMAD screenings in these settings as well could help catch even more women with these disorders: About 45 percent of parents had a positive screen for depression at NICU discharge, and about 27 percent of recent mothers had positive screens for PMADs in the ED.
To further these efforts, Children’s National recently started a Perinatal Mental Health Taskforce to promote multidisciplinary collaboration and open communication with providers among multiple hospital divisions. This taskforce is working together to apply lessons learned from screening in primary care, the NICU and the ED to discuss best practices and develop hospital-wide recommendations. They’re also sharing their experiences with hospitals across the country to help them develop best practices for helping women with PMADs at their own institutions.
Furthering its commitment to PMAD screening, Children’s National leadership set a goal of increasing screening in primary care by 15 percent for fiscal year 2018 – then exceeded it. Children’s National is also helping women with PMADs far outside the hospital’s walls by developing a PMAD screening toolkit for other providers in Washington and across the country and by connecting with community partners through the DC Collaborative for Mental Health in Pediatric Primary Care. In April 2019, the hospital will host a regional perinatal mental health conference that not only will include its own staff but also staff from other local hospitals and other providers who care for new mothers, including midwives, social workers, psychologists, community health workers and doulas.
Finally, on a federal level, Dr. Jarvis and colleagues are part of efforts to obtain additional resources for PMAD screening, referral and treatment. They successfully advocated for Congress to fully fund the Screening and Treatment for Maternal Depression program, part of the 21st Century Cures Act. And locally, they provided testimony to help establish a task force to address PMADs in Washington.
Together, Dr. Jarvis says, these efforts are making a difference for women with PMADs and their families.
“All this work demonstrates that you can take a problem that is very personal, this individual experience with PMADS, and work together with a multidisciplinary team in collaboration to really have an impact and promote change across the board,” she adds.
In addition to Dr. Jarvis, the lead author, Children’s co-authors include Penelope Theodorou, MPH; Sarah Barclay Hoffman, MPP, Program Manager, Child Health Advocacy Institute; Melissa Long, M.D.; Lamia Soghier M.D., MEd, NICU Medical Unit Director; Karen Fratantoni M.D., MPH; and Senior Author Lee Beers, M.D., Medical Director, Municipal and Regional Affairs, Child Health Advocacy Institute.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/new-mom-with-baby.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-16 11:13:402022-11-21 10:14:16Fighting perinatal mood and anxiety disorders on multiple levels
Clinical Research Assistant Kevin Jackson uses AlgometRx Platform Technology on Sarah Taylor’s eyes to measure her degree of pain. Children’s National is testing an experimental device that aims to measure pain according to how pupils react to certain stimuli. (AP Photo/Manuel Balce Ceneta)
Pediatric anesthesiologist Julia C. Finkel, M.D., of Children’s National Health System, gazed into the eyes of a newborn patient determined to find a better way to measure the effectiveness of pain treatment on one so tiny and unable to verbalize. Then she realized the answer was staring back at her.
Armed with the knowledge that pain and analgesic drugs produce an involuntary response from the pupil, Dr. Finkel developed AlgometRx, a first-of-its-kind handheld device that measures a patient’s pupillary response and, using proprietary algorithms, provides a diagnostic measurement of pain intensity, pain type and, after treatment is administered, monitors efficacy. Her initial goal was to improve the care of premature infants. She now has a device that can be used with children of any age and adults.
“Pain is very complex and it is currently the only vital sign that is not objectively measured,” says Dr. Finkel, who has more than 25 years of experience as a pain specialist. “The systematic problem we are facing today is that healthcare providers prescribe pain medicine based on subjective self-reporting, which can often be inaccurate, rather than based on an objective measure of pain type and intensity.” To illustrate her point, Dr. Finkel continues, “A clinician would never prescribe blood pressure medicine without first taking a patient’s blood pressure.”
The current standard of care for measuring pain is the 0-to-10 pain scale, which is based on subjective, observational and self-reporting techniques. Patients indicate their level of pain, with zero being no pain and ten being highest or most severe pain. This subjective system increases the likelihood of inaccuracy, with the problem being most acute with pediatric and non-verbal patients. Moreover, Dr. Finkel points out that subjective pain scores cannot be standardized, heightening the potential for misdiagnosis, over-treatment or under-treatment.
Dr. Finkel, who serves as director of Research and Development for Pain Medicine at the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National, says that a key step in addressing the opioid crisis is providing physicians with objective, real-time data on a patient’s pain level and type, to safely prescribe the right drug and dosage or an alternate treatment.,
She notes that opioids are prescribed for patients who report high pain scores and are sometimes prescribed in cases where they are not appropriate. Dr. Finkel points to the example of sciatica, a neuropathic pain sensation felt in the lower back, legs and buttocks. Sciatica pain is carried by touch fibers that do not have opioid receptors, which makes opioids an inappropriate choice for treating that type of pain.
A pain biomarker could rapidly advance both clinical practice and pain research, Dr. Finkel adds. For clinicians, the power to identify the type and magnitude of a patient’s nociception (detection of pain stimuli) would provide a much-needed scientific foundation for approaching pain treatment. Nociception could be monitored through the course of treatment so that dosing is targeted and personalized to ensure patients receive adequate pain relief while reducing side effects.
“A validated measure to show whether or not an opioid is indicated for a given patient could ease the health care system’s transition from overreliance on opioids to a more comprehensive and less harmful approach to pain management,” says Dr. Finkel.
She also notes that objective pain measurement can provide much needed help in validating complementary approaches to pain management, such as acupuncture, physical therapy, virtual reality and other non-pharmacological interventions.
Dr. Finkel’s technology, called AlgometRx, has been selected by the U.S. Food and Drug Administration (FDA) to participate in its “Innovation Challenge: Devices to Prevent and Treat Opioid Use Disorder.” She is also the recipient of Small Business Innovation Research (SBIR) grant from the National Institute on Drug Abuse.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/AlgometRX.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-10 07:35:322024-09-06 15:28:51Breakthrough device objectively measures pain type, intensity and drug effects
Teens have a biological preference to fall asleep later than younger children and adults, and wake up later, due to a delayed release of hormones that promote sleep. This timing coincides with puberty and makes it harder for middle and high school students to fall asleep early – regardless of 5 a.m. alarms and 7:17 a.m. school start times.
After studying this trend among nearly 1,000 seventh and eighth-grade students in 11 middle schools within a Mid-Atlantic school district, Daniel Lewin, Ph.D., a sleep medicine specialist, pediatric psychologist and associate director of the sleep medicine program at Children’s National Health System, coauthored and published research entitled “Later Start, Longer Sleep: Implications of Middle School Start Times” in the Journal of School Health, which outlines the benefits of delaying school start times.
The research team divided students into two groups: Close to 650 students attended eight late-starting middle schools, where school started at 8 a.m., while nearly 350 students attended early-starting middle schools, where school started at 7:23 a.m.
Students starting school 37 minutes later, despite going to bed 15 minutes later than peers attending an earlier-starting school, got 17 minutes more sleep each night and were more likely to report feeling wide awake during class. The researchers predicted this later-starting school model would translate to students getting an extra 75 minutes of sleep a week – roughly 51 hours of extra sleep each school year. These researchers find that every two minutes in delayed school start times results in one minute of additional sleep each night for children and teens.
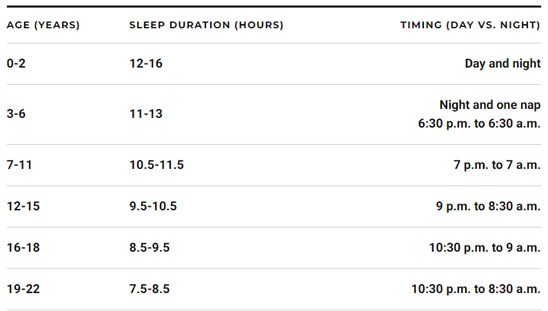
Middle and high school students should get 8.5 to 10.5 hours of sleep each night, ideally between 9 p.m. and 8:30 a.m. for 12- to 15-year-olds and 10:30 p.m. and 9 a.m. for 16- to 18-year-olds.
The American Academy of Pediatrics (AAP) published similar research in their journal, Pediatrics, about the benefits of letting teens catch up on sleep, citing a reduced risk of students being overweight, getting into car accidents or suffering from depression as well as a greater likelihood of having better grades, higher test scores and a better quality of life. AAP recommends schools start at 8:30 a.m. or later to allow students to get 8.5 to 9.5 hours of sleep each night and issued a statement in 2014, entitled “School Start Times for Adolescents.”
Dr. Lewin continues to track these benefits and works with schools to implement the changes. He recently wrote an editorial, entitled “All the Clocks Are Ticking: Sleep Health and Metabolism,” for the Journal of Adolescent Health about the correlation between improved sleep health, mental and physical health and academic performance, explaining how circadian clocks, present on a cellular level, influence behavior and metabolism.
While pushing school start times back requires an immediate investment of rearranging travel routes, bell schedules and after-school activities, several school districts near Washington, D.C., from Virginia Beach to Fairfax County, are adopting this public health model.
An economic analysis conducted by the RAND Corporation finds that after two years, the benefits of reorganizing school start times outweigh the costs.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/General-school-supplies.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-10 07:00:302021-10-25 11:56:40Studying the impact of later school start times
The 2-year-old scampered unexpectedly into a room, startling a family member. Thinking the toddler was an intruder, the family member fired, hitting the child in the chest.
In the emergency department at Children’s National Health System, Lenore Jarvis, M.D. MEd, FAAP, emergency medicine specialist, and colleagues tried to save the boy’s life, inserting tubes, transfusing blood and attempting to restart his dying heart via CPR. The Children’s team was unsuccessful and emerged covered in the blood of a boy whose death was heartbreaking and preventable.
“Firearm violence is a leading cause of childhood traumatic death and injury,” Dr. Jarvis told attendees of a recent congressional news conference intended to prod the incoming Congress to take more concrete action to prevent firearm violence. She provided snapshots of some of the countless lives of local youths cut short by firearms, including an 8-year-old girl killed on a playground in a drive-by shooting, a 13-year-old young man murdered during a fight, a 15-year-old young woman who committed suicide and an entire family who died from firearm injuries.
“I wish it were not so. But these stories are endless. In our emergency department, the effects of gun violence are frequent, life-altering and personal,” Dr. Jarvis said.
The #ThisISOurLane press conference, convened by U.S. Rep. Robin Kelly, (D-Illinois), included haunting stories by clinicians from across the nation about the devastating impact of firearm injuries on children and youth. According to a retrospective, cross-sectional study led by Children’s researchers, younger children are more likely to be shot by accident, and odds are higher that older youths are victims of an assault involving a firearm.
“Gun violence is a public health crisis and should be addressed as such. We need to reduce the numbers of suicides, homicides and accidental gun deaths in children,” added Dr. Jarvis, who also is president-elect of the District of Columbia Chapter of the American Academy of Pediatrics.
During the news conference, U.S. Rep. Frank Pallone Jr., (D-New Jersey), vowed that the House Energy and Commerce Committee he chairs this session will move forward languishing bills, including funding the Centers for Disease Control Prevention to conduct firearms violence research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/Lenore-Jarvis-at-thisisourlane-meeting.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-08 10:33:262019-07-19 10:55:35#thisisourlane: Pediatricians call for safer firearm storage, enhanced research funding
A mutation of the gene PAC1R may be linked to the severity of social deficits experienced by kids with autism spectrum disorder (ASD), finds a study from a multi-institutional research team led by Children’s National faculty. If the pilot findings are corroborated in larger, multi-center studies, the research published online Dec. 17, 2018, in Autism Research represents the first step toward identifying a potential novel biomarker to guide interventions and better predict outcomes for children with autism.
As many as 1 in 40 children are affected by ASD. Symptoms of the disorder – such as not making eye contact, not responding to one’s name when called, an inability to follow a conversation of more than one speaker or incessantly repeating certain words or phrases – usually crop up by the time a child turns 3.
The developmental disorder is believed to be linked, in part, to disrupted circuitry within the amygdala, a brain structure integral for processing social-emotional information. This study reveals that PAC1R is expressed during key periods of brain development when the amygdala – an almond-shaped cluster of neurons – develops and matures. A properly functioning amygdala, along with brain structures like the prefrontal cortex and cerebellum, are crucial to neurotypical social-emotional processing.
“Our study suggests that an individual with autism who is carrying a mutation in PAC1R may have a greater chance of more severe social problems and disrupted functional brain connectivity with the amygdala,” says Joshua G. Corbin, Ph.D., interim director of the Center for Neuroscience Research at Children’s National Health System and the study’s co-senior author. “Our study is one important step along the pathway to developing new biomarkers for autism spectrum disorder and, hopefully, predicting patients’ outcomes.”
The research team’s insights came through investigating multiple lines of evidence:
They looked at gene expression in the brains of an experimental model at days 13.5 and 18.5 of fetal development and day 7 of life, dates that correspond with early, mid and late amygdala development. They confirmed that Pac1r is expressed in the experimental model at a critical time frame for brain development that coincides with the timing for altered brain trajectories with ASD.
They looked at gene expression in the human brain by mining publicly available genome-wide transcriptome data, plotting median PAC1R expression values for key brain regions. They found high levels of PAC1R expression at multiple ages with higher PAC1R expression in male brains during the fetal period and higher PAC1R expression in female brains during childhood and early adulthood.
One hundred twenty-nine patients with ASD aged 6 to 14 were recruited for behavioral assessment. Of the 48 patients who also participated in neuroimaging, 20 were able to stay awake for five minutes without too much movement as the resting state functional magnetic resonance images were captured. Children who were carriers of the high-risk genotype had higher resting-state connectivity between the amygdala and right posterior temporal gyrus. Connectivity alterations in a region of the brain involved in processing visual motion may influence how kids with ASD perceive socially meaningful information, the authors write.
Each child also submitted a saliva sample for DNA genotyping. Previously published research finds that a G to C single nucleotide polymorphism, a single swap in the nucleotides that make up DNA, in PAC1R is associated with higher risk for post traumatic stress disorder in girls. In this behavioral assessment, the research team found children with autism who carried the homozygous CC genotype had higher scores as measured through a validated tool, meaning they had greater social deficits than kids with the heterozygous genotype.
All told, the project is the fruit of six years of painstaking research and data collection, say the researchers. That includes banking patients’ saliva samples collected during clinical visits for future retrospective analyses to determine which genetic mutations were correlated with behavioral and functional brain deficits, Corbin adds.
“Lauren Kenworthy, who directs our Center for Autism Spectrum Disorders, and I have been talking over the years about how we could bring our programs together. We homed in on this project to look at about a dozen genes to assess correlations and brought in experts from genetics and genomics at Children’s National to sequence genes of interest,” he adds. “Linking the bench to bedside is especially difficult in neuroscience. It takes a huge amount of effort and dozens of discussions, and it’s very rare. It’s an exemplar of what we strive for.”
Financial support for the research described in this report was provided by DC-IDDRC under awards HD040677-07 and 1U54HD090257, the Clinical and Translational Science Institute at Children’s National, The Isidore and Bertha Gudelsky Family Foundation and the National Institutes of Health under awards MH083053-01A2 and MH084961.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/DNA.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-08 09:40:512024-09-06 15:24:53PAC1R mutation may be linked to severity of social deficits in autism
Children younger than age 2 need at least 12 hours of sleep each day.
As families and parents renew their interest in health in the new year, pediatricians can take advantage of this momentum by talking about one area absent from common New Year’s resolutions lists: getting enough sleep.
Like diet, exercise and activities that keep your brain sharp, such as reading or learning a new language, healthful sleep patterns play a vital role in supporting physical health and cognitive performance – especially for children and teens.
Here are a few tips parents and pediatricians can use, based on research published by Daniel Lewin, Ph.D., a pediatric psychologist and sleep medicine specialist at Children’s National Health System.
Understand how much sleep each child needs.
The typical range of recommended sleep, such as eight to 10 hours each night, varies for each child. A 16-year-old may do well with 8.5 hours of sleep, while a 6-year-old may need 13 hours of sleep to stay alert. Their body is still rapidly developing. The timing of sleep matters, too, due to a child’s natural circadian rhythm. A chart below details sleep recommendations based on age.
Turn a child’s bedroom into a healthful sleep chamber.
Encouraging children to fall asleep by 7 or 9 p.m. may require planning – outside of maintaining regular sleep schedules. To start, make it easy to promote sound sleep by eliminating distractions, including clocks and electronic devices, which might sit next to a child’s bed and distract him or her from getting a good night’s sleep.
Reserve a designated area for homework and study hours outside of the bedroom, which helps reinforce that the bed is a place for sleep and rest. Avoid doing any complicated routines or activities that might cause excitement right before bed, such as assembling a new toy or playing a high-stakes game.
Follow the same rules for conversations: Don’t have talks that might evoke excitement, like the next Disneyworld vacation, or stress, such as bringing the next day’s spelling test up right before bed. By creating a calm zone, you’ll avoid energizing the biological ‘burst zone,’ a rush of energy that occurs in short bursts before one prepares to rest for the night. Keep conversations and routines simple and soothing. Reading, stretching or practicing mindfulness and yoga are complementary activities children can practice at least 15 minutes before bedtime.
Schedule activities about circadian rhythms.
Understanding when a child sleeps best is just as important as understanding how much sleep is essential to support optimal health. A student in high school is biologically wired to stay up past 9 p.m. due to a later release of hormones that promote sleep. This is one reason some school systems are experimenting with later middle and high school start times, which, according to a review in the Journal of School Health, increases a student’s chance of feeling ‘wide awake’ and alert in the classroom.
If you have control of your student’s schedule, plan around it. For instance, schedule activities for a 17-year-old in the late morning, if possible, while allowing time in the afternoon for a young child to take a nap.
These starter tips serve as ways to strengthen sleep quality. Learn more about Dr. Lewin’s research at PubMed, view a few of his blogs for parents at U.S. News & World Report and learn about the link between sleep and health at the National Institutes of Health. If you experience recurring problems, such as sleep apnea, insomnia, sleep walking, ongoing sleep disruptions or excessive daytime sleepiness, connect with a health care provider.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/smiling-baby-sleeping.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-07 10:43:172024-12-30 12:54:38The science behind optimal sleep health
To help clinicians provide better care to families after children die, Tessie W. October, M.D., MPH, and colleagues recently published an article on this topic in a special supplement to Pediatric Critical Care Medicine on death and dying.
Death and dying are always difficult topics to discuss at hospitals. They’re especially hard conversations when they occur within pediatric intensive care units (PICUs), says Tessie W. October, M.D., MPH, a critical care specialist at Children’s National.
“It’s almost easier to pretend that children don’t die in the ICU. But they do,” Dr. October says.
Tragically, some children do die in ICUs. However, even when pediatric patients die, Dr. October adds, the pediatric care team’s relationship with the bereaved family continues. Knowing how to help vulnerable families during these trying times and ensuring they have needed resources can be critical to lessening the health and social consequences of grief. To help clinicians provide better care to families after children die, Dr. October and colleagues recently published an article on this topic in a special supplement to Pediatric Critical Care Medicine on death and dying.
The multi-institutional research team performed a narrative literature review for this budding field. They pored through more than 75 papers to better understand the health outcomes of parents whose child died within a PICU and the different ways that hospitals help families cope with these tragedies.
The researchers found a range of detrimental health outcomes, from a significantly increased risk of parental death in the aftermath of a child’s death to higher rates of myocardial infarction, cancer and multiple sclerosis. Bereaved parents used more health care resources themselves, took more sick days and had more sleep problems than parents who weren’t bereaved.
Likewise, parents whose child died were at a high risk of experiencing mental health conditions including complicated grief, anxiety, depression and posttraumatic stress disorder. Divorce was eight times higher among bereaved parents compared with the general population, and financial crises were common after voluntary or involuntary unemployment.
Knowing which risks parents could face can help the care team respond better if a child dies, Dr. October explains. Their review highlighted simple ways to support families in the immediate aftermath of a child’s death and beyond, such as:
Giving parents the opportunity to spend time alone with the child’s body
Allowing friends, family and others to visit at the parents’ discretion and
Providing easy access to professional support, such as chaplains, social workers and grief coordinators.
Even simple acts such as closing doors and blinds to provide privacy can be helpful, Dr. October says.
An ongoing relationship with health care providers is also important for helping parents grieve, she adds. Children’s National is among hospitals across the country to set up meetings for parents and other family members within weeks of a child’s death. This gives parents a chance to ask questions about what happened in the confusing blur of the PICU and to gather resources for themselves and surviving siblings. Children’s National also provides ongoing support through periodic calls, sending sympathy cards, attending funeral services and in a special annual memorial during which surviving family members release butterflies.
“Our role doesn’t end when a child dies,” Dr. October says. “To help parents through bereavement, we need to maintain that strong connection.”
Another way to help bereaved families is to make sure they have adequate information, she adds, particularly about the confusing subject of brain death. In a different study recently published in Chest Journal, Dr. October and Children’s colleagues sought to understand which information the public typically accesses about this topic.
The team searched Google and YouTube using “brain dead” and “brain death” as search terms. They evaluated the top 10 results on both sites, assessing the accuracy of information using 2010 guidelines released by the American Academy of Neurology. They also assessed the reading level of websites and evaluated comments about the YouTube videos for content accuracy and tone.
They found that there was inaccurate information on four of the 10 websites, six of the 10 videos and within 80 percent of the YouTube comments. Most of these inaccuracies dealt with using terms like brain death, coma and persistent vegetative state interchangeably. “These conditions are very different and affect how we treat patients,” Dr. October says.
The average reading level of the websites was 12th grade, far too sophisticated for much of the public to comprehend, she adds. And the majority of comments on the YouTube videos were negative, often disparaging clinicians and deriding organ donation.
“It’s really important for providers to recognize that this is an emotionally laden topic, and a lot of times, families come to us with information that’s not always true,” she says. “That’s why it’s especially important for the field to respond with empathy and care.”
In addition to Dr. October, co-authors of the Pediatric Critical Care Medicine study include Karen Dryden-Palmer, R.N., MSN, Ph.D., The Hospital for Sick Children; Beverley Copnell, Ph.D., BAppSc, R.N., Monash University; and Senior Author Kathleen L. Meert, M.D., FCCM, Children’s Hospital of Michigan. Dr. October’s co-authors for the Chest Journal article include Lead Author, Amy H. Jones, M.D., and co-author Zoelle B. Dizon, BA, both of Children’s National.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/PICU-room.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-27 11:51:512020-11-16 09:17:41How to help bereaved families
A small percentage of women said they consumed fewer allergens during pregnancy to stave off food allergies in their newborns, according to preliminary research Karen Robbins, M.D., presented during the American College of Asthma Allergy and Immunology 2018 Annual Scientific Meeting.
Pregnant women routinely swear off alcohol and tobacco to boost their chances of having a healthy baby. What about common food allergens like nuts and milk?
There are scant data that describe how often pregnant women deliberately stop eating a specific food item in order to prevent future food allergies in their newborns. As a first step toward addressing this data gap, a research team led by Karen Robbins, M.D., an allergist at Children’s National Health System, pored through a longitudinal study conducted by the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention.
About 4,900 pregnant women completed the Infant Feeding Practices Study II prenatal questionnaire from May 2005 to June 2007. The study tracked 2,000 pregnant women from the third trimester of pregnancy and their infants through the first year of life. A small percentage of women said they had consumed fewer allergens during pregnancy to stave off food allergies in their newborns, according to a poster Dr. Robbins presented during the American College of Asthma Allergy and Immunology 2018 Annual Scientific Meeting. While their numbers were small, most of these women reported giving up major allergens like nuts, milk or eggs during pregnancy, including:
144 (2.9 percent) reported restricting their diet in some way to prevent future food allergies in their offspring
84 women (1.7 percent) ate fewer nuts
15 women (.3 percent) ate fewer eggs and
2 women (.04 percent) ate/drank consumed less dairy/milk.
“At the time the survey was conducted, few pregnant women in this large data set said they gave up certain foods with the express aim of avoiding a food allergy in their babies,” Dr. Robbins says. “However, mothers who had an older child with a food allergy or who had food allergies themselves had significantly higher odds of trying this food avoidance strategy.”
Despite the diet changes, infants born to these expectant mothers were twice as likely to experience problems with food at age 4 months – though not at age 9 months or 12 months. And these infants were no more likely to be diagnosed with a food allergy.
According to the FDA, millions of Americans suffer a food allergy each year. Reactions can range from mild to life-threatening and can begin soon after eating a problematic food item or an ingredient from that food. Among the most common allergenic foods are milk, eggs, fish, shellfish, tree nuts, peanuts, wheat and soybeans.
“We really need to know more about how often targeted food avoidance occurs among U.S. pregnant women who have a family history of food allergies,” Dr. Robbins adds. “We hope to learn what factors into these women’s decision-making as well as why many of them settled on food avoidance as a potential strategy to try to prevent food allergy in their infants.”
American College of Asthma Allergy and Immunology 2018 Annual Scientific Meeting presentation
“Prenatal food allergen avoidance practices for food allergy prevention.”
Karen Robbins M.D., lead author; Ashley Ramos Ph.D., co-author; Marni Jacobs, Ph.D., co-author; Kate Balas BS, co-author; and Linda Herbert, Ph.D., director of Children’s Division of Allergy and Immunology’s psychosocial clinical program, and senior author.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/pregnant-woman-holding-eggs.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-17 11:16:382024-10-29 15:31:58How does diet during pregnancy impact allergies in offspring?
On December 4, 2018, Children’s National Health System was named a 2018 “Top Children’s Hospital” by The Leapfrog Group, an independent watchdog organization. The highest performing hospitals on the Leapfrog Hospital Survey are recognized annually for this prestigious award. Children’s National is proud to have been recognized 10 times as “Top Children’s Hospital.” Top hospitals are given the designation for having distinct achievements in patient safety and quality, including lower infection rates, decreased length of stay, fewer readmissions and higher survival rates for high-risk procedures.
“We’re particularly proud of this acknowledgment as it recognizes our unwavering commitment to high-quality patient care,” said Kurt Newman, M.D., president and CEO of Children’s National. “It highlights our exceptional clinicians and support teams who work to constantly improve the safety of the care we provide.”
The Top Children’s Hospitals are selected based on The Leapfrog Group’s annual survey of nearly 1,900 hospitals across the country which measures hospitals’ performance in many areas of hospital care, including reduced medication rates and capacity to prevent medication errors.
“Being acknowledged as a Top Children’s Hospital is an incredible feat achieved by less than six percent of eligible hospitals nationwide,” said Leah Binder, president and CEO of The Leapfrog Group. “With this honor, Children’s National has established its commitment to safer and higher quality care. Providing this level of care to patients in Washington, D.C. requires motivation and drive from every team member. I congratulate the board, staff and clinicians, whose efforts made this honor possible.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/top-childrens-hospital-logo-2018.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-14 10:03:512023-07-03 10:49:39The Leapfrog Group names Children’s National Health System a 2018 “Top Children’s Hospital”
“A combination of prenatal MRI and US was able to detect Zika-related brain abnormalities during pregnancy, giving families timely information to prepare for the potential complex care needs of these infants,” says Sarah B. Mulkey, M.D., Ph.D.
Worldwide, thousands of babies have been born to mothers who were infected during pregnancy with Zika, a virus associated with neurological deficits, impaired vision and neurodevelopmental disabilities, among other birth defects. These birth defects are sometimes severe, causing lifelong disability. But they’re also relatively rare compared with the overall rates of infection.
Predicting how many Zika-exposed babies would experience neurological birth defects has been challenging.
However, an international study led by Children’s faculty suggests that ultrasound (US) imaging performed during pregnancy and after childbirth revealed most Zika-related brain abnormalities experienced by infants exposed to the Zika virus during pregnancy, according to a prospective cohort study published online Nov. 26, 2018, in JAMA Pediatrics. Some Zika-exposed infants whose imaging had been normal during pregnancy had mild brain abnormalities detected by US and magnetic resonance imaging (MRI) after they were born.
“A combination of prenatal MRI and US was able to detect Zika-related brain abnormalities during pregnancy, giving families timely information to prepare for the potential complex care needs of these infants,” says Sarah B. Mulkey, M.D., Ph.D., a fetal-neonatal neurologist at Children’s National Health System and the study’s lead author. “In our study, we detected mild brain abnormalities on postnatal neuroimaging for babies whose imaging was normal during pregnancy. Therefore, it is important for clinicians to continue to monitor brain development for Zika-exposed infants after birth.”
As of Nov. 20 2018, nearly 2,500 pregnant women in the U.S. had laboratory confirmed Zika infection, and about 2,400 of them had given birth, according to the Centers for Disease Control and Prevention (CDC). While more than 100 U.S. infants were born with Zika-associated birth defects, the vast majority of Zika-exposed U.S. infants were apparently normal at birth. The sequential neuroimaging study Dr. Mulkey leads seeks to determine the spectrum of brain findings in infants exposed to Zika in the womb using both US and MRI before and after birth.
The international research team enrolled 82 women in the study from June 15, 2016, through June 27, 2017. All of the women had been exposed to Zika during pregnancy; all but one experienced clinical symptoms by a mean gestational age of 8.2 weeks. Eighty of those women lived in or near Barranquilla, Colombia, and were exposed to Zika there. Two U.S. study participants were exposed to the primarily mosquito-borne illness during travel to Zika hot zones.
All women received fetal MRIs and US during the second and/or third trimester of pregnancy. After their infants were born, the children received brain MRI and cranial US. Blood samples from both mothers and babies were tested for Zika using polymerase chain reaction and serology.
Fetal MRI was able to discern Zika-related brain damage as early as 18 weeks gestation and picked up significant fetal brain abnormalities not fully appreciated in US imaging. In one case, the US remained normal while fetal MRI alone detected brain abnormalities. Three fetuses (4 percent) had severe fetal brain abnormalities consistent with Zika infection, including:
Two cases of heterotopias and malformations in cortical development, and
One case of parietal encephalocele, Chiari II malformation and microcephaly.
Seventy-five infants were born at term. One pregnancy was terminated at 23 weeks gestation due to the gravity of the fetal brain abnormalities. One fetus with normal imaging died during pregnancy. One newborn who was born with significant fetal brain abnormalities died at age 3 days.
Cranial US and brain MRI was performed on the majority of infants whose prenatal imaging had been normal. Seven of 53 (13 percent) Zika-exposed infants had mild brain abnormalities detected by MRI after birth. In contrast, postnatal cranial US was better at detecting changes of lenticulostriate vasculopathy, cysts within the brain’s choroid plexus (cells that produce cerebrospinal fluid), germinolytic/subependymal cysts and/or calcifications, which were seen in 21 of 57 (37 percent) infants.
“Sequential neuroimaging revealed that the majority of Zika-exposed fetuses had normal brain development. Tragically, in a small number of pregnancies, Zika-related brain abnormalities were quite severe,” Dr. Mulkey adds. “Our data support the CDC’s recommendation that cranial US be performed after Zika-exposed babies are born. In addition, there is clearly a need to follow these babies over time to gauge whether the brain anomalies we see in imaging affects language, motor and social skills.”
In addition to Dr. Mulkey, study co-authors include Dorothy I. Bulas, M.D., Gilbert Vezina, M.D., Margarita Arroyave-Wessel, MPH, Stephanie Russo, B.S, Youssef A. Kousa, D.O, Ph.D., Roberta L. DeBiasi, M.D., MS, Senior Author Adré J. du Plessis, M.B.Ch.B., MPH, all of Children’s National; Christopher Swisher, BS, Georgetown University and Caitlin Cristante, BS, Loyola University, both of whose contributions included research performed at Children’s National; Yamil Fourzali, M.D., Armando Morales, M.D., both of Sabbag Radiologos; Liliana Encinales, M.D., Allied Research Society; Nelly Pacheco, Bacteriologa, Bio-Nep; Robert S. Lanciotti, Ph.D., Arbovirus Diseases Branch, Centers for Disease Control and Prevention; and Carlos Cure, M.D., BIOMELAB.
Research reported in this news release was supported by the IKARIA fund.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/12/Sarah-B.-Mulkey.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-12-07 12:35:192024-05-29 09:02:15MRI and ultrasound imaging detect the spectrum of Zika’s impact
A Children’s research team found the number of children and adolescents visiting the nation’s emergency departments due to mental health concerns continued to rise at an alarming rate from 2012 through 2016, with mental health diagnoses for non-Latino blacks outpacing such diagnoses among youth of other racial/ethnic groups.
The demand for mental health services continues to be high in the U.S., even among children. The Centers for Disease Control and Prevention (CDC) reports that one in seven U.S. children aged 2 to 8 had a diagnosed mental, behavioral or developmental disorder. In addition, 3 percent of U.S. children aged 3 to 17 had a diagnosis of anxiety, and 2.1 were diagnosed with depression, according to the CDC.
Knowing which children use mental health services can help health care providers improve access and provide more targeted interventions.
Children’s researchers recently investigated this question in the emergency room setting, reporting results from their retrospective cross-sectional study at the American Academy of Pediatrics (AAP) 2018 National Conference & Exhibition. The research team found the number of children and adolescents visiting the nation’s emergency departments due to mental health concerns continued to rise at an alarming rate from 2012 through 2016, with mental health diagnoses for non-Latino blacks outpacing such diagnoses among youth of other racial/ethnic groups.
“Access to mental health services among children can be difficult, and data suggest that it can be even more challenging for minority children compared with non-minority youths,” says Monika K. Goyal, M.D., MSCE, assistant division chief and director of research in the Division of Emergency Medicine at Children’s National Health System and the study’s senior author. “Our findings underscore the importance of improving access to outpatient mental health resources as well as expanding capacity within the nation’s emergency departments to respond to this unmet need.”
An estimated 17.1 million U.S. children are affected by a psychiatric disorder, making mental health disorders among the most common pediatric illnesses. Roughly 2 to 5 percent of all emergency department visits by children are related to mental health concerns. The research team hypothesized that within that group, there might be higher numbers of minority children visiting emergency departments seeking mental health services.
To investigate this hypothesis, they examined Pediatric Health Information System data, which aggregates deidentified information from patient encounters at more than 45 children’s hospitals around the nation. Their analyses showed that in 2012, 50.4 emergency department visits per 100,000 children were for mental health-related concerns. By 2016, that figure had grown to 78.5 emergency department visits per 100,000 children.
During that same five-year time span, there were 242,036 visits by children and adolescents 21 and younger with mental health-related issues*. Within that group:
The mean age was 13.3
Nearly 55 percent were covered by public insurance
78.4 per 100,000 non-Latino black children received mental health-related diagnoses and
51.5 per 100,000 non-Latino white children received mental health-related diagnoses.
“When stratified by race and ethnicity, mental health-related visits to the nation’s emergency departments rose for non-Latino black children and adolescents at almost double the rate seen for non-Latino white children and adolescents,” Dr. Goyal adds. “These children come to our emergency departments in crisis, and across the nation children’s hospitals need to expand mental health resources to better serve these vulnerable patients.”
Because the study did not include reviews of individual charts or interviews with patients or providers, the reason for the disparate demand for mental health resources remains unclear.
*The number of patient visits during the five-year study period was revised on Nov. 1 2018, after updated analyses.
American Academy of Pediatrics National Conference & Exhibition presentation
“Racial disparities in pediatric mental health-related emergency department visits: a five-year, multi-institutional study.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/11/Emergency-signs.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-11-23 10:35:492024-10-29 15:40:23Disparities in who accesses emergency mental health services
According to a retrospective, cross-sectional study led by Children’s researchers, younger kids are more likely to be shot by accident, and odds are higher that older youths are victims of an assault involving a firearm.
An increasing number of children are injured by firearms in the U.S. each year, but the reasons these injuries happen vary. According to a new retrospective, cross-sectional study led by Children’s researchers and presented at the American Academy of Pediatrics (AAP) 2018 National Conference & Exhibition, firearm injuries vary by the intent of the person discharging the weapon. Younger kids are more likely to be shot by accident, and odds are higher that older youths are victims of an assault involving a firearm. Efforts to protect children from firearm-related injuries should factor in these differences in intent as legislation and policies are drafted, the study team suggests.
Researchers led by Shilpa J. Patel, M.D., MPH, Children’s assistant professor of pediatrics and emergency medicine, reviewed data aggregated in the Nationwide Emergency Department Sample from 2009 to 2013 looking for emergency department visits to treat firearm-related injuries suffered by children and adolescents 21 and younger. They excluded emergency department visits for firearm-related injuries attributed to air, pellet, BB or paintball guns.
Firearm-related injuries are a leading cause of injury and death for U.S. children. Some 111,839 children and youth were treated in emergency departments for firearm-related injuries, or 22,367 per year when averaged over the five-year study period. Nearly 63 percent of these youths were injured by accident; 30.4 percent were victims of assault; 1.4 percent used a firearm to injure themselves. Of note:
89.3 percent were male
Their mean age was 18 (67.3 percent 18 to 21; 27.9 percent 13 to 17; 4.8 percent younger than 12)
1 percent were discharged from the emergency department
30 percent had injuries grave enough to trigger hospital admission and
1 percent died from their injuries.
“Children younger than 12 were more likely to be shot by accident. By contrast, we found that the odds of experiencing firearm-related injuries due to assault were higher for youths aged 18 to 21,” Dr. Patel says. “Physicians can play a powerful role in preventing pediatric firearm-related injuries by routinely screening for firearm access and speaking with families about safe firearm storage and violence prevention,” she adds.
Some 52.1 percent of children with firearm-related injuries lived with families whose median household incomes exceeded $56,486.
American Academy of Pediatrics National Conference & Exhibition presentation
“Emergency department visits for pediatric firearm-related injury: by intent of injury.”
Shilpa J. Patel, M.D., MPH, assistant professor of pediatrics and emergency medicine and lead author, Gia M. Badolato, MPH, senior clinical research data manager and study co-author, Kavita Parikh, M.D., MS, associate professor of pediatrics and study co-author, and Monika K. Goyal, M.D., MSCE, assistant division chief and director of Academic Affairs and Research in the Division of Emergency Medicine and study senior author, all of Children’s National Health System; and Sabah F. Iqbal, M.D., medical director, PM Pediatrics, study co-author.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/10/ambulance.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-11-21 10:29:482018-11-26 15:23:45Accident or assault? Pediatric firearm injuries differ by age
Myriad biological and societal factors can impact the occurrence and accelerate progression of chronic kidney disease for children of African descent – including preterm birth, exposure to toxins during gestation and lower socioeconomic status – and can complicate these children’s access to effective treatments.
Myriad biological and societal factors can impact the occurrence and accelerate progression of chronic kidney disease (CKD) for children of African descent – including preterm birth, exposure to toxins during gestation and lower socioeconomic status – and can complicate these children’s access to effective treatments, according to an invited commentary published in the November 2018 edition of American Journal of Kidney Diseases.
Clinicians caring for “these vulnerable children should be mindful of these multiple competing and compounding issues as treatment options are being considered along the continuum from CKD to kidney failure to transplantation,” writes Marva Moxey-Mims, M.D., chief of the Division of Nephrology at Children’s National Health System.
The supplemental article was informed by lessons learned from The Chronic Kidney Disease in Children (CKiD) longitudinal study and conversations that occurred during the Frank M. Norfleet Forum for Advancement of Health, “African Americans and Kidney Disease in the 21st Century.”
African American children represent 23 percent of the overall population of kids with CKD in the CKiD study. While acquired kidney diseases can get their start during childhood when the diseases betray few symptoms, the full impact of illness may not be felt until adulthood. A number of factors can uniquely affect children of African descent, heightening risk for some kids who already are predisposed to suffering more severe symptoms. These include:
Preterm birth. African American children make up 36 percent of patients in CKiD with glomerular disease, which tends to have faster progression to end-stage renal disease. These diseases impair kidney function by weakening glomeruli, which impairs the kidneys’ ability to clean blood. Patients with a high-risk apolipoprotein L1 (APOL1) genotype already are at higher risk for focal segmental glomerulosclerosis (FSGS) and CKD. Researchers hypothesize that preterm birth may represent “a second hit that facilitates the development of glomerular damage resulting from the high-risk genotype.” According to the Centers for Disease Control and Prevention, 1 in 10 U.S. infants in 2016 was born preterm, e.g., prior to 37 weeks gestation.
APOL1 genotype. Compared with children who had a low-risk genotype and FSGS, children with a high-risk genotype had higher rates of uncontrolled hypertension, left ventricular hypertrophy, elevated C-reactive protein levels and obesity.
Human immunodeficiency viral (HIV) status. About 65 percent of U.S. children with HIV-1/AIDS are African American. In a recent nested case-control study of children infected with HIV in the womb, infants with high-risk APOL1 genotypes were 3.5 times more likely to develop CKD with viral infection serving as “a likely second hit.”
Access to kidney transplant. African American adults experience a faster transition to end-stage renal disease and are less likely to receive kidney transplants. African American children with CKD from nonglomerular diseases begin renal replacement therapy 1.6 years earlier than children of other races, after adjusting for socioeconomic status. Their wait for dialysis therapy was 37.5 percent shorter. However, these African American children waited 53.7 percent longer for transplants. Although donor blood types, genetic characteristics and other biological factors each play contributing roles, “these findings may reflect sociocultural and institutional differences not captured by socioeconomic status,” Dr. Moxey-Mims writes.
To alleviate future health care disparities, she suggests that additional research explore the impact of expanding services to pregnant women to lower their chances of giving birth prematurely; early childhood interventions to help boost children’s educational outcomes, future job prospects and income levels; expanded studies about the impact of environmental toxicities on prenatal and postnatal development; and heightened surveillance of preterm infants as they grow older to spot signs of kidney disease earlier to slow or prevent disease progression.
“Clinicians can now begin to take into account genetics, socioeconomic status and the impact of the built environment, rather than blaming people and assuming that their behavior alone brought on kidney disease,” Dr. Moxey-Mims adds. “Smoking, not eating properly and not exercising can certainly make people vulnerable to disease. However, there are so many factors that go into developing a disease that patients cannot control: You don’t control to whom you’re born, where you live or available resources where you live. These research projects will be useful to help us really get to the bottom of which factors we can impact and which things can’t we prevent but can strive to mitigate.”
The article covered in this post is part of a supplement that arose from the Frank M. Norfleet Forum for Advancement of Health: African Americans and Kidney Disease in the 21st Century, held March 24, 2017, in Memphis, Tennessee. The Forum and the publication of this supplement were funded by the Frank M. Norfleet Forum for Advancement of Health, the Community Foundation of Greater Memphis and the University of Tennessee Health Science Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/11/little-girl-in-hospital-corridor.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-11-20 12:29:372024-05-29 09:16:21A growing list of factors that impact CKD severity for kids