
Breakthrough device objectively measures pain type, intensity and drug effects

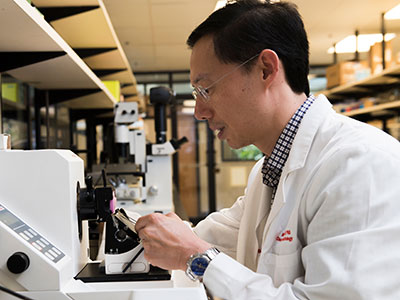
Clinical Research Assistant Kevin Jackson uses AlgometRx Platform Technology on Sarah Taylor’s eyes to measure her degree of pain. Children’s National is testing an experimental device that aims to measure pain according to how pupils react to certain stimuli. (AP Photo/Manuel Balce Ceneta)
Pediatric anesthesiologist Julia C. Finkel, M.D., of Children’s National Health System, gazed into the eyes of a newborn patient determined to find a better way to measure the effectiveness of pain treatment on one so tiny and unable to verbalize. Then she realized the answer was staring back at her.
Armed with the knowledge that pain and analgesic drugs produce an involuntary response from the pupil, Dr. Finkel developed AlgometRx, a first-of-its-kind handheld device that measures a patient’s pupillary response and, using proprietary algorithms, provides a diagnostic measurement of pain intensity, pain type and, after treatment is administered, monitors efficacy. Her initial goal was to improve the care of premature infants. She now has a device that can be used with children of any age and adults.
“Pain is very complex and it is currently the only vital sign that is not objectively measured,” says Dr. Finkel, who has more than 25 years of experience as a pain specialist. “The systematic problem we are facing today is that healthcare providers prescribe pain medicine based on subjective self-reporting, which can often be inaccurate, rather than based on an objective measure of pain type and intensity.” To illustrate her point, Dr. Finkel continues, “A clinician would never prescribe blood pressure medicine without first taking a patient’s blood pressure.”
The current standard of care for measuring pain is the 0-to-10 pain scale, which is based on subjective, observational and self-reporting techniques. Patients indicate their level of pain, with zero being no pain and ten being highest or most severe pain. This subjective system increases the likelihood of inaccuracy, with the problem being most acute with pediatric and non-verbal patients. Moreover, Dr. Finkel points out that subjective pain scores cannot be standardized, heightening the potential for misdiagnosis, over-treatment or under-treatment.
Dr. Finkel, who serves as director of Research and Development for Pain Medicine at the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National, says that a key step in addressing the opioid crisis is providing physicians with objective, real-time data on a patient’s pain level and type, to safely prescribe the right drug and dosage or an alternate treatment.,
She notes that opioids are prescribed for patients who report high pain scores and are sometimes prescribed in cases where they are not appropriate. Dr. Finkel points to the example of sciatica, a neuropathic pain sensation felt in the lower back, legs and buttocks. Sciatica pain is carried by touch fibers that do not have opioid receptors, which makes opioids an inappropriate choice for treating that type of pain.
A pain biomarker could rapidly advance both clinical practice and pain research, Dr. Finkel adds. For clinicians, the power to identify the type and magnitude of a patient’s nociception (detection of pain stimuli) would provide a much-needed scientific foundation for approaching pain treatment. Nociception could be monitored through the course of treatment so that dosing is targeted and personalized to ensure patients receive adequate pain relief while reducing side effects.
“A validated measure to show whether or not an opioid is indicated for a given patient could ease the health care system’s transition from overreliance on opioids to a more comprehensive and less harmful approach to pain management,” says Dr. Finkel.
She also notes that objective pain measurement can provide much needed help in validating complementary approaches to pain management, such as acupuncture, physical therapy, virtual reality and other non-pharmacological interventions.
Dr. Finkel’s technology, called AlgometRx, has been selected by the U.S. Food and Drug Administration (FDA) to participate in its “Innovation Challenge: Devices to Prevent and Treat Opioid Use Disorder.” She is also the recipient of Small Business Innovation Research (SBIR) grant from the National Institute on Drug Abuse.




















 Wilms tumor, also known as nephroblastoma, is the most common pediatric kidney cancer, typically seen in children ages three to four. Compared to patients with unilateral Wilms tumors, children with bilateral Wilms tumors (BWT) have poorer event-free survival (EFS) and are at higher risk for later effects such as renal failure. The treatment of BWT is challenging because it involves surgical removal of the cancer, while preserving as much healthy kidney tissue as possible to avoid the need for an organ transplant.
Wilms tumor, also known as nephroblastoma, is the most common pediatric kidney cancer, typically seen in children ages three to four. Compared to patients with unilateral Wilms tumors, children with bilateral Wilms tumors (BWT) have poorer event-free survival (EFS) and are at higher risk for later effects such as renal failure. The treatment of BWT is challenging because it involves surgical removal of the cancer, while preserving as much healthy kidney tissue as possible to avoid the need for an organ transplant.


 Children’s National is proud to be named #1 in
Children’s National is proud to be named #1 in 



