Children’s fetal medicine fellow named ‘Outstanding graduate student’

Laura Sanapo, M.D., M.S.H.S., told the graduating class that two guiding themes defined her experience as a GW student: diversity and momentum.
Laura Sanapo, M.D., M.S.H.S., a fetal medicine fellow at Children’s Fetal Medicine Institute, was named “Outstanding graduate student” at The George Washington University School of Medicine & Health Sciences (GWSMHS) and was among two student speakers to address fellow graduates during the ceremony held May 19, 2018.
Dr. Sanapo was selected from a competitive field of top-tier graduate students from an array of academic programs, says Samar A. Nasser, Ph.D., M.P.H., PA-C, director of Clinical and Translational Research and Clinical Health Sciences at GWSMHS, who nominated her for the award. “She is one of the brightest students I have encountered. Because of her exceptional background, I recruited Dr. Sanapo to become an adjunct professor in our Clinical and Translational Research program and I look forward to co-teaching a course with her this fall.”
“I am extremely humbled and honored by this recognition for my ongoing research,” Dr. Sanapo says. “It is a privilege to join the GW faculty and contribute to the growth of an outstanding academic team and diverse group of students. I feel energized by such a collegial and dynamic environment.”
She told the graduating class that two guiding themes defined her experience as a GW student: diversity and momentum. Diversity, she told the group “means the spark that generates new ideas and growth” and momentum is the feeling of being “propelled forward by being part of a university that feels like a lively workshop of ideas.”
Prior to joining Children’s National Health System in 2014, Dr. Sanapo served with distinction at the University of Maryland School of Medicine and Thomas Jefferson University School of Medicine, conducting original research and frequently publishing in peer-reviewed journals.
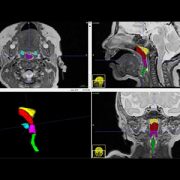
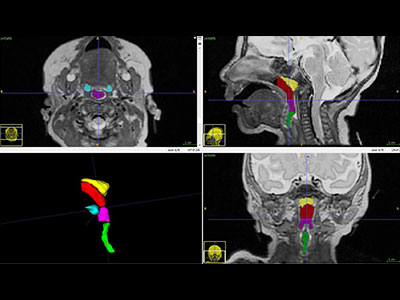
Under the mentorship of Adré J. du Plessis, M.B.Ch.B., M.P.H., chief of Children’s Division of Fetal and Transitional Medicine, Dr. Sanapo investigated the role of advanced ultrasound techniques in assessing fetal vasoreactivity in pregnancies complicated by such conditions as intrauterine growth restriction, Dr. Nasser wrote in the nomination letter. In that study, the research team is trying to better understand how a healthy fetus controls blood flow throughout the body, including to the lungs and brain.
In addition to evaluating and counseling in high-risk pregnancies complicated by complex fetal malformations, Dr. Sanapo performed research and clinical ultrasounds daily. What’s more, Dr. Sanapo often scheduled appointments after-hours for patients unable to complete ultrasounds during normal business hours and was an integral part of the team that counseled women through difficult pregnancies.
“‘These women are especially vulnerable and they deserve 100 percent of my time, knowledge, energy and empathy,’ ” Dr. Nasser recalls Dr. Sanapo explaining. “Laura often goes above and beyond her responsibilities as a fellow to assist these women in need.”
Dr. du Plessis notes that Dr. Sanapo has been a valued clinical leader at Children’s Fetal Medicine Institute, shepherding a multidisciplinary team that includes genetic counselors, specialists in maternal-fetal medicine, radiologists, pediatric neurologists and nurses.
“When Children’s National and Inova announced a three-year, $2.8 million research and education collaboration in maternal, fetal and neonatal medicine last January, Laura’s contributions were pivotal in ensuring the research collaboration’s early success,” Dr. du Plessis adds.