Pioneering NF innovation and treatment: Q&A with Benjamin Siegel, MD
 For more than four decades, Children’s National Hospital has been at the forefront of neurofibromatosis (NF) care, research and treatment. In 2007, Dan and Jennifer Gilbert furthered this mission by establishing the Gilbert Family Neurofibromatosis Institute in honor of their son Nick. The Gilberts have dedicated themselves to eradicating NF and improving the future for those affected. Their partnership with Children’s National has transformed the Institute into a global hub for NF care and innovation.
For more than four decades, Children’s National Hospital has been at the forefront of neurofibromatosis (NF) care, research and treatment. In 2007, Dan and Jennifer Gilbert furthered this mission by establishing the Gilbert Family Neurofibromatosis Institute in honor of their son Nick. The Gilberts have dedicated themselves to eradicating NF and improving the future for those affected. Their partnership with Children’s National has transformed the Institute into a global hub for NF care and innovation.
“Since 1982, we’ve combined compassionate care with cutting-edge innovation to provide the best outcomes for our patients while advancing NF treatment,” says Roger J. Packer, MD, director of the institute.
Dr. Packer leads a team of NF experts, including Benjamin Siegel, MD, clinical co-director of the institute, whose expertise in pediatric neurology and neuro-oncology is critical to the program’s success. In this Q&A, Dr. Siegel shares what sets Children’s National apart, how it benefits patients and the latest NF research advancements.
What makes the Gilbert Family Neurofibromatosis Institute at Children’s National unique from other programs in the country?
The Gilbert Family Neurofibromatosis Institute is the longest-running NF program in the United States, with over 40 years of leadership in advancing the field. We helped establish the initial diagnostic criteria in the 1980s and have been pivotal in chairing the Neurofibromatosis Clinical Trials Consortium. Our involvement in groundbreaking clinical trials led to FDA approval of the first targeted therapies for NF1-associated plexiform neurofibromas. Building upon this strong legacy, we continue to advance the future of care for those affected by NF.
Our multidisciplinary team, led by Sinan Turnacioglu, MD, and myself under Dr. Packer’s direction, integrates diverse expertise. My background in neurology and neuro-oncology, combined with Dr. Turnacioglu’s expertise in neurodevelopmental disabilities, allows us to provide comprehensive, high-quality care. With access to specialized clinical resources, we ensure each patient receives the most informed and well-rounded treatment.
How does the work in this program benefit patients?
Our program’s success lies in its comprehensive, interdisciplinary approach to patient care. NF and schwannomatosis can impact every organ system in the body, making close collaboration among specialists essential to address each patient’s unique needs. Our goal is to act as a “medical home” for individuals with NF, ensuring seamless, coordinated care across neurology, oncology, genetics, orthopedics, neurosurgery, plastic surgery, otolaryngology, endocrinology, cardiology and psychiatry.
Recent expansions include neuropsychology, led by Karin Walsh, PsyD, providing comprehensive clinical neuropsychological testing, and physical medicine and rehabilitation, where Mi Ran Shin, MD, MPH, helps manage musculoskeletal issues and chronic pain. This integrated approach allows us to address the complex concerns of NF patients effectively, improving both their physical function and quality of life.
How is Children’s National leading the way in NF research?
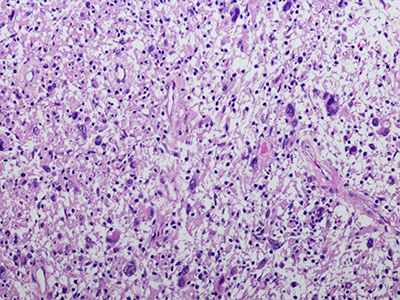
Children’s National is at the forefront of NF research, with groundbreaking translational studies spearheaded by its cutting-edge hospital laboratories. Our team is pioneering the use of organoid models to better understand malignant transformations in NF1-associated low-grade gliomas. With a focus on developing targeted therapies for currently untreatable high-grade gliomas, Children’s National has been selected as a key member of the newly funded Gilbert Family NF1-Assosiated Glioma Consortium, an initiative dedicated to advancing treatment options for NF1-associated gliomas.
As a founding member of the Neurofibromatosis Clinical Trials Consortium (NFCTC), we led pivotal clinical trials on targeted therapies for NF1 and schwannomatosis (NF2) tumors. In 2025, the consortium will launch three new trials focused on NF1-associated plexiform neurofibromas. In development are trials evaluating bone health in NF1, attention deficit disorder in NF1, preventative therapy for NF2-associated schwannomas and new treatments for high-grade gliomas and malignant peripheral nerve sheath tumors (MPNST).
Beyond the NFCTC, Children’s National is a member of the Pediatric Brain Tumor Consortium, contributing to selumetinib research for NF1 gliomas. Additionally, through the leadership of internationally known solid tumor oncologist AeRang Kim, MD, PhD, we’re involved with the Sarcoma Alliance for Research through Collaboration, with a focus on developing treatments for MPNST.
Dr. Walsh’s neuropsychology program has advanced understanding of NF1-related cognitive challenges through studies on MEK inhibitors’ effects on neurocognition and links between sleep disorders and ADHD. It also recently completed a pilot study on the Unstuck and On Target program to improve executive function in NF1.
What else is important for peers to know?
A diagnosis of NF or schwannomatosis can be overwhelming and frightening for families due to the wide range of symptoms and manifestations. This uncertainty can often lead to significant anxiety, as patients and their families may struggle to understand what to expect in terms of medical care, progression and treatment options.
At the Gilbert Family Neurofibromatosis Institute, we aim to ease this uncertainty by providing a comprehensive care approach. We offer not only cutting-edge clinical treatments but also support and guidance through the complexities of the disorder. Our team is committed to addressing concerns, providing updated information about the latest research and connecting families to ongoing clinical trials and support resources. By offering a personalized, multi-disciplinary approach, we help our patients navigate their diagnosis with greater confidence and hope for the future.
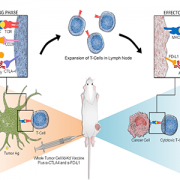
Looking ahead, Children’s National is set to advance NF research and care with a five-year grant from the Gilbert Family Foundation. The hospital will collaborate with global institutions to address NF-1 associated transformed gliomas and launch the first clinical study using molecular targeted therapy and immunotherapy to treat this aggressive tumor, marking a key milestone in its commitment to innovative treatments and improved outcomes for children with NF.