In a new study published in JAMA Network Open, experts at Children’s National and allied institutions created and validated the first dataset to depict hemorrhage control for machine learning applications, the simulated outcomes following carotid artery laceration (SOCAL) video dataset.
Computer algorithms, such as machine learning and computer vision, are increasingly able to discover patterns in visual data, powering exciting new technologies worldwide. At Children’s National Hospital, physician-scientists develop and apply these advanced algorithms to make surgery safer by studying surgical video.
In a new study published in JAMA Network Open, experts at Children’s National and allied institutions created and validated the first dataset to depict hemorrhage control for machine learning applications, the simulated outcomes following carotid artery laceration (SOCAL) video dataset.
The authors designed SOCAL to serve as a benchmark for data-science applications, including object detection, performance metric development and outcome prediction. Hemorrhage control is a high-stakes adverse event that can pose unique challenges for video analysis. With SOCAL, the authors aim to solve a valuable use case with algorithms.
“As neurosurgeons, we are often called to perform high-risk and high-impact procedures. No one is more passionate about making surgery safer,” said Daniel Donoho, M.D., neurosurgeon at Children’s National Hospital and senior author of the study. “Our team at Children’s National and the Sheikh Zayed Institute is poised to lead this exciting new field of surgical data science.”
These algorithms require raw data for their development, but the field lacks datasets that depict surgeons managing complications.
By creating automated insights from surgical video, these tools may one day improve patient care by detecting complications before patients are harmed, facilitating surgeon development.
“Until very recently, surgeons have not known what may be possible with large quantities of surgical video captured each day in the operating room,” said Gabriel Zada, M.D., M.S., F.A.A.N.S., F.A.C.S., director of the Brain Tumor Center at the University of Southern California (USC) and co-author of the study. “Our team’s research led by Dr. Donoho shows the feasibility and the potential of computer vision analysis in surgical skill assessment, virtual coaching and simulation training of surgeons.”
The lack of videos of adverse events creates a dataset bias which hampers surgical data science. SOCAL was designed to meet this need. After creating a cadaveric simulator of internal carotid artery injury and training hundreds of surgeons on the model at nationwide courses, the authors then developed computational models to measure and improve performance.
“We are currently comparing our algorithms to experts, including those developed using the SOCAL dataset,” Dr. Donoho said. “Human versus machine, and our patients are ultimately the winners in the competition.”
The authors are also building a nationwide collective of surgeons and data scientists to share data and improve algorithm performance through exciting partnerships with USC, California Institute of Technology and other institutions.
You can read the full study “Utility of the Simulated Outcomes Following Carotid Artery Laceration Video Data Set for Machine Learning Applications” in JAMA Network Open.
In a pre-clinical model, researchers from Children’s National Hospital found that the Mueller polarimetric imaging, a novel technique that improves image contrast, may help identify nerves from other surrounding tissues during neck and head surgical procedures, avoiding accidental nerve damage.
“This technology holds great promise for the possibility of a truly noninvasive imaging approach and may help improve surgical outcomes by potentially reducing inadvertent, ill effects of nerve injuries in head and neck surgery,” said Bo Ning, Ph.D., R&D engineer at Children’s National and lead author of the study.
This pre-clinical study presents the first application of a full-field polarimetric imaging technique in vivo during head and neck surgery to highlight the vagus nerve (VN) and a branch that supplies all the intrinsic muscles to the larynx, known as recurrent laryngeal nerve (RLN).
“Unlike conventional nerve identification devices, this technique is noninvasive and less interruptive to intact tissues without disrupting surgical workflows,” said Ning et al. “Since the technique has an easy mechanism and promising performance in our study, this novel method holds great potential for real-time, noninvasive, and convenient nerve visualization.”
While some promising methods use polarimetric imaging for tissue characterizations, the current literature is still limited to ex vivo conditions due to the system complications and prolonged acquisition speeds.
“Recently, the industry released a new polarimetric camera, which is compact and allows fast and high-definition polarimetric imaging through simple snapshots. Enlightened by this technical advance, we have developed a practical polarimetric imaging method,” said Ning, who also develops compact and practical imaging systems for surgical innovation, including 3D, fluorescent, laser speckle and hyperspectral techniques. “It allows fast polarimetric analysis and can acquire birefringence maps over the whole field of view within 100 milliseconds, which provides an appropriate speed for directly surgical use.”
The new approach proofs that the concept is feasible to set up in live subjects during head and neck surgery, which can also be easily adapted for other surgeries. Among the seven subjects, the VNs and RLNs were successfully differentiated from arteries and other surrounding tissues.
Additional co-authors from Children’s National include Itai Katz, Ph.D., M.S., R&D staff engineer III; Anthony D. Sandler, M.D., Senior Vice President and Surgeon-in-Chief; Richard Jaepyeong Cha, Ph.D., research faculty assistant professor.
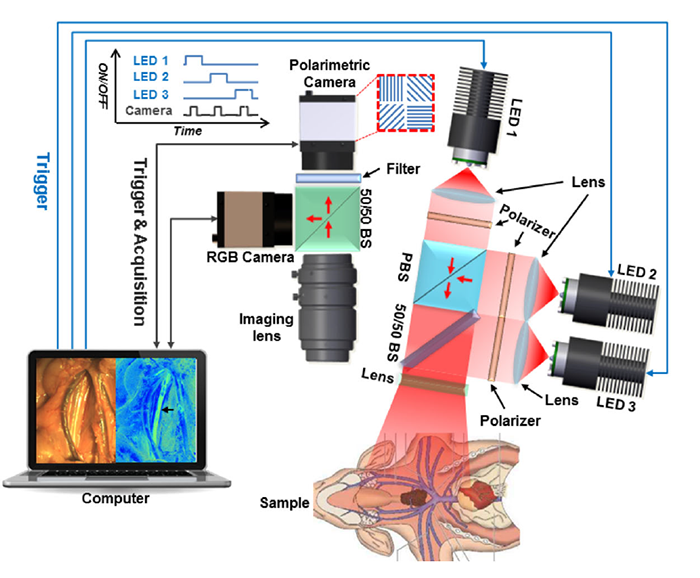
Researchers at Children’s National used a novel technique that improves image contrast, which may help improve surgical outcomes.

Researchers found that patients with localized pediatric renal cell carcinoma have excellent short-term outcomes without adjuvant therapy.
Although renal cell carcinoma (RCC) is the second most common kidney cancer diagnosed in children and adolescents, guidance regarding its clinical management has been confined to retrospective case series, which were limited by reporting bias, varied treatment approaches and a lack of central pathology review to confirm the diagnosis.
Research conducted by the Children’s Oncology Group (COG) and led by Jeffrey Dome, M.D., Ph.D., vice president of the Center for Cancer and Blood Disorders at Children’s National Hospital, found that patients with localized pediatric RCC have excellent short-term outcomes without adjuvant therapy with 4-year overall survival estimates of 96% for patients with stage I disease, 100% for patients with stage II disease and 88% for patients with stage III disease.
“The results of this study provide important practical insights into the management of pediatric RCC,” said Dr. Dome. “Oncologists now have validation that a surgery-only approach is appropriate management for the majority of children and adolescents with RCC.”
“The results of this study provide important practical insights into the management of pediatric RCC,” said Jeffrey Dome, M.D., Ph.D.
The excellent survival in patients with stage III disease held up even in those with tumor involvement of regional lymph nodes, a finding that differs from adult RCC. However, patients with metastatic disease (stage IV), had a 4-year overall survival estimate of only 29%, demonstrating the need to find active treatments for this group. Outcomes varied according to tumor histological subtype. Nearly all recurrences occurred in patients with the translocation histology and renal medullary carcinoma; recurrences were rare in other subtypes.
A follow-up study called AREN1721 is now open in the Children’s Oncology Group and adult cancer cooperative groups that participate in the National Clinical Trials Network. This study involves a comparison of two treatment regimens for metastatic or unresectable “translocation” renal cell carcinoma, the most common subtype of renal cell carcinoma in children, adolescents and young adults. The treatment regimens will include nivolumab, a PD1 immune checkpoint inhibitor, with or without axitinib, a tyrosine kinase inhibitor that targets vascular endothelial growth factor receptor (VEGFR).


Due to the global COVID-19 pandemic, the 1st Joint Congress of European Pediatric Surgeons’ Association (EUPSA), International Pediatric Endosurgery Group (IPEG), and European Society of Paediatric Endoscopic Surgeons (ESPES) in Vienna, Austria, was canceled. Despite this, EUPSA’s Education Office continued to foster collaboration and further educational opportunities among members in order to maintain and improve high standards of surgical care for pediatric surgical patients around the globe.
This included a webinar of case discussions on “Decision Making in Pediatric Colorectal Surgery,” led by Marc Levitt, M.D., Colorectal and Pelvic Reconstructive Surgeon at Children’s National Hospital. The international panel included Giulia Brisighelli (Johannesburg, ZA) Martin Lacher (Leipzig, Germany), Paula Midrio (Triviso, Italy), Carlos Reck (Vienna, Austria), Pim Sloots (Rotterdam, Netherlands), Gaia Tamaro (EUPSA Education Office), Alejandra Villanova (Madrid, Spain), and Tomas Wester (Stockholm, Sweden).
Dr. Levitt has since presented follow-up webinars on the following topics:
You can view the full webinars below:
The cover of the new Pediatric Colorectal and Pelvic Reconstructive Surgery textbook, edited by Marc A. Levitt, M.D., and Alejandra Vilanova-Sánchez, M.D.
The first edition of the Pediatric Colorectal and Pelvic Reconstructive Surgery textbook, edited by Marc A. Levitt, M.D., and Alejandra Vilanova-Sánchez, M.D., is now available.
The textbook provides comprehensive coverage of the anatomical and physiological aspects of complex colorectal and pelvic malformations presented in a practical and clinically focused way. Some of the topics explored include surgical protocols, the benefits of high-level collaboration between surgical services when treating these anomalies, treatment algorithms and care of complications.
The book also includes content on:
The Pediatric Colorectal and Pelvic Reconstructive Surgery, 1st edition textbook can be purchased here, and will benefit colorectal teams worldwide.

Marc Levitt, M.D., leads the colorectal program at Children’s National Hospital and is editor of the new Pediatric Colorectal and Pelvic Reconstructive Surgery textbook.
Marc Levitt, M.D., currently leads the colorectal program at Children’s National Hospital, the first in the mid-Atlantic region to fully integrate surgery, urology, gynecology and gastroenterology into one cohesive program for children. He has been the driving force around the world in enhancing the care of children with colorectal and pelvic reconstructive needs through the development of specialized, integrated and collaborative surgical centers. He is internationally recognized as specializing in conditions affecting the newborn, pediatric and adolescent population affected with anorectal malformations (imperforate anus), cloacal malformations, Hirschsprung disease, as well as a variety of conditions leading to fecal incontinence, such as spinal conditions and functional constipation. Dr. Levitt has written three textbooks, and has authored over 200 scientific articles on these subjects.
Dr. Levitt is the founder of the Colorectal Team Overseas (CTO), which is a group of international providers that travel to the developing world to provide care and teaching for patients with colorectal needs. He co-founded the creation of the Pediatric Colorectal and Pelvic Learning Consortium (PCPLC), which is an organization of collaborating colorectal centers across the globe.
Alejandra Vilanova-Sánchez, M.D., is a pediatric surgeon in the urogenital and colorectal unit at the University Hospital La Paz, Madrid. After finishing her training, she completed a fellowship in Pelvic Reconstruction Surgery at the Center for Colorectal and Pelvic Reconstruction at Nationwide Children’s Hospital. Her focus was on complex colorectal and pelvic surgery involving the gynecological and urological systems. Dr. Vilanova-Sánchez is a member of the Spanish Association of Pediatric Surgeons, European Pediatric Surgical Association (EUPSA) and ARM-net. She is a frequent speaker in international meetings and she has organized several national and international meetings on the topic of pediatric colorectal care. She participates annually in surgical brigades collaborating with nonprofit organizations, Colorectal Team Overseas and Helping Hands for Anorectal Malformations International, where she helps patients with colorectal conditions around the world.



Children’s National Hospital announced that world-class surgeon Yves d’Udekem, M.D., Ph.D., will become the next Chief of Cardiac Surgery and Co-Director of the Children’s National Heart Institute this summer.
Dr. d’Udekem is Belgian-born with Canadian and Australian citizenship and received his early training in Belgium and Toronto. As an attending cardiac surgeon in Belgium, he operated on both adults and children with congenital heart disease. Dr. d’Udekem then worked with internationally recognized heart surgeon Marc de Laval, M.D., FRCS, and others in London to train in congenital heart surgery at the Great Ormond Street Hospital for Children.
From there, he was recruited to The Royal Children’s Hospital in Melbourne, Australia, an institution that has been a leader in advancing the field of congenital heart disease. In Melbourne, Dr. d’Udekem built an outstanding reputation for clinical excellence and an exceptional academic career. He has over 300 publications and is highly cited and respected. Dr. d’Udekem obtained more than $7 million in grant funding over the past five years as the creator and leader of the highly touted Fontan Registry.
The Children’s National Cardiology team and hospital leadership have built a framework for Dr. d’Udekem to succeed and advance the legacy that has been so successfully created in cardiac surgery by Richard Jonas, M.D. Dr. Jonas is a world leader in congenital heart surgery who made significant clinical and academic advances in the field and will continue his award-winning research career at Children’s National in the laboratory focusing on neurodevelopmental outcomes for children with heart disease.
Children’s National offers a comprehensive surgical program that includes a team of experienced surgeons performing the full range of procedures available for treatment of pediatric cardiac disease and congenital heart defects. The high volume program serves neonates through adults with congenital heart disease with particular attention to neurodevelopmental outcomes.
Researchers at Children’s National Hospital are using quantitative imaging and machine intelligence to enhance care for children with a common kidney disease, and their initial results are very promising. Their technique provides an accurate way to predict earlier which children with hydronephrosis will need surgical intervention, simplifying and enhancing their care.
We live in a time of great uncertainty yet great promise, particularly when it comes to harnessing technology to improve lives. Researchers at Children’s National Hospital are using quantitative imaging and machine intelligence to enhance care for children with a common kidney disease, and their initial results are very promising. Their technique provides an accurate way to predict earlier which children with hydronephrosis will need surgical intervention, simplifying and enhancing their care.
Hydronephrosis means “water in the kidney” and is a condition in which a kidney doesn’t empty normally. One of the most frequently detected abnormalities on prenatal ultrasound, hydronephrosis affects up to 4.5% of all pregnancies and is often discovered prenatally or just after birth.
Although hydronephrosis in children sometimes resolves by itself, identifying which kidneys are obstructed and more likely to need intervention isn’t particularly easy. But it is critical. “Children with severe hydronephrosis over long periods of time can start losing kidney function to the point of losing a kidney,” says Marius George Linguraru, DPhil, MA, MSc, principal investigator of the project; director of Precision Medical Imaging Group at the Sheikh Zayed Institute for Pediatric Surgical Innovation; and professor of radiology, pediatrics and biomedical engineering at George Washington University.
Children with hydronephrosis face three levels of examination and intervention: ultrasound, nuclear imaging testing called diuresis renogram and surgery for the critical cases. “What we want to do with this project is stratify kids as early as possible,” Dr. Linguraru says. “The earlier we can predict, the better we can plan the clinical care for these kids.”
Ultrasound is used to see whether there is a blockage and try to determine hydronephrosis severity. “Ultrasound is non-invasive, non-radiating, and does not expose the child to any risk prenatally or postnatally,” Dr. Linguraru says. Ultrasound evaluations require a trained radiologist, but there’s a lot of variability. Radiologists have a grading system based on the ultrasound appearance of the kidney to determine whether the hydronephrosis is mild, moderate or severe, but studies show this isn’t predictive of longer term outcomes.
Children whose ultrasounds show concern will be referred to diuresis renogram. Costly, complex, invasive and irradiating, it tests how well the kidney empties. Although appropriate for good clinical indications, doctors try to minimize its use. “Management of hydronephrosis is complex,” Dr. Linguraru says. “We want to use ultrasound as much as possible and much less diuresis renogram.”
For those patients whose kidney is obstructed and eventually need surgical intervention, the sooner that decision can be made the better. “The more you wait for a kidney that is severely obstructed, the more function may be lost. If intervention is required, it’s preferable to do it early,” Dr. Linguraru says. Of course for the child whose hydronephrosis will likely resolve itself, intervention is not the best option.
“With our technique we are measuring physiological and anatomical changes in the ultrasound image of the kidney,” says Marius George Linguraru, DPhil, MA, MSc. “The human eye may find it difficult to put all this together, but the machine can do it. We use quantitative imaging to do deep phenotyping of the kidney and machine learning to interpret the data.”
Dr. Linguraru and the multidisciplinary team at Children’s National Hospital, including radiology and urology clinicians, are putting the power of computers to work interpreting subtleties in the ultrasound data that humans just can’t see. In their pilot study they found that 60% of the nuclear imaging tests could have been safely avoided without missing any of the critical cases of hydronephrosis. “With our technique we are measuring physiological and anatomical changes in the ultrasound image of the kidney,” Dr. Linguraru says. “The human eye may find it difficult to put all this together, but the machine can do it. We use quantitative imaging to do deep phenotyping of the kidney and machine learning to interpret the data.”
Results of the initial study indicate that kids who have a mild condition can be safely discharged earlier and the model can predict all those kids with obstructions and accelerate their diagnosis by sending them earlier to get further investigation. Dr. Linguraru says. “There are only benefits: some kids will get earlier diagnosis, some earlier discharges.”
The team also has a way to improve the interpretation of diuresis renograms. “We analyze the dynamics of the kidney’s drainage curve in quantifiable way. Using machine learning to interpret those results, we showed we can potentially discharge some kids earlier and accelerate intervention for the most severe cases instead of waiting and repeating the invasive tests,” he says. The framework has 93% accuracy, including 91% sensitivity and 96% specificity, to predict surgical cases, a significant improvement over clinical metrics’ accuracy.
The next step is a study connecting all the protocols. “Right now we have a study on ultrasound, a study on nuclear imaging, but we need to connect them so a child with hydronephrosis immediately benefits,” says Dr. Linguraru. Future work will focus on streamlining and accelerating diagnosis and intervention for kids who need it, both in prospective studies and hopefully clinically as well.
Hydronephrosis is an area in which machine learning can be applied to pediatric health in meaningful ways because of the sheer volume of cases.
“Machine learning algorithms work best when they are trained well on a lot of data,” Dr. Linguraru says. “Often in pediatric conditions, data are sparse because conditions are rare. Hydronephrosis is one of those areas that can really benefit from this new technological development because there is a big volume of patients. We are collecting more data, and we’re becoming smarter with these kinds of algorithms.”
Learn more about the Precision Medical Imaging Laboratory and its work to enhance clinical information in medical images to improve children’s health.


Our neurosurgery team is among the most experienced in the nation. We have performed thousands of surgeries and are dedicated to giving the best possible care. The Children’s National Hospital Division of Neurosurgery consistently ranks among the country’s top programs according to U.S. News & World Report.
Patients travel to us from all over the world because we have the resources and expertise necessary to care for their neurological conditions through multidisciplinary programs such as:
The Children’s National Hospital Division of Neurosurgery is among the first in the country to develop new techniques and adopt the latest technologies that make minimally invasive neurosurgery possible by utilizing state of the art equipment and developing new techniques, including:
Children’s National is involved in cutting edge scientific research offering new hope for our patients and new methods of treatment. Our doctors have developed some of the most advanced treatments and clinics for our patients including:
U.S. News & World Report ranks our neurosurgery program number five in the nation, reflecting our commitment to excellence in care for our patients and families.
Children’s National is one of only 12 children’s hospitals in the country to attain Level 1 Surgery Verification from the American College of Surgeons.

Children with rare and medically complex conditions, such as brain tumors, craniofacial disorders, Chiari malformations, vascular disorders and brachial plexus palsy, to name a few, achieve exceptional outcomes at Children’s National. Our patients experience fewer complications, go home sooner and maintain long-term symptom relief.
Our entire team is dedicated to meeting your child’s unique needs. Our Neuro-Intensive Care Unit nurses recognize signs of pain and complications your child may not be able to explain.
Children’s National is at the forefront of new device-based treatments that not only fix neurologic problems, but also restore brain function. We are one of the few pediatric programs in the country offering dedicated pediatric deep brain stimulation, which uses a pacemaker-like device to significantly reduce the burden of movement disorders and difficult-to-control epilepsy, as well as Neuropace implantation to help with seizures in eloquent areas of the brain.
We are proudly training the next generation of pediatric neurosurgeons through residency programs and fellowships in conjunction with several area medical schools.


The cerebral palsy program at Children’s National Hospital takes a comprehensive approach to meet children’s needs from infancy through young adulthood.
Though children with cerebral palsy (CP) often require significant rehabilitative and surgical support, most often each service is provided in the individual specialty itself. Patients and their families frequently experience a great deal of stress coordinating care, getting to appointments, keeping track of medications and managing treatments on their own.
However, the CP program at Children’s National Hospital, co-led by an orthopaedic surgeon, Sean Tabaie, M.D., and a pediatric rehabilitation specialist, Olga Morozova, M.D., working together and in collaboration with Shannon Kelly, M.D., (Orthopaedics) and Jeff Rabin, D.O., (Physical Medicine and Rehabilitation) has evolved into a truly comprehensive approach. The program is designed to meet the needs of these children from infancy through young adulthood with the goal of improving function and preventing musculoskeletal deformities and complications.
Providing children and their families with a single point of care coordination allows the care team to track and anticipate a multitude of potential challenges for each child as early as possible and intervene in smaller ways before they bring pain and long-term complications or require major surgical interventions. Key highlights of this collaborative program include:
The doctors point out that offering these services in one cohesive location and combining treatments into the same appointment or procedure date is something that many patients with CP and their families truly appreciate.
“I think families of children with CP will travel great distances if the care they receive is comprehensive and eliminates some of the back and forth travel they do now,” says Dr. Tabaie.
Today, the team sees close to 100 patients with CP per month and hopes to expand to reach as many families in the region and beyond who need them.
Dr. Tabaie says, “Our goal is to identify patients early and start managing them to help their quality of life today, prepare them to grow as healthily and in as little pain as possible and set them up to be as healthy as they can possibly be as adults, too.”
“With the broad range of expertise at Children’s National, including the nation’s best NICU, I’m confident that colorectal patients will get better, integrated care faster and more effectively here than anywhere else in the world,” says Marc Levitt, M.D.
World-renowned surgeon opens first program for care and treatment of colorectal conditions in the mid-Atlantic.
A new, highly-specialized surgical program at Children’s National Hospital is expected to draw patients from around the world. The colorectal surgery program is the first in the mid-Atlantic region to fully integrate surgery, urology, gynecology and gastroenterology into one cohesive program for children. The program is led by Marc Levitt, M.D., an internationally recognized expert in the surgical care and treatment of pediatric colorectal disorders who has performed over 10,000 surgeries to address a wide spectrum of problems involving the colon and rectum – more than any other full time practicing pediatric surgeon in the world.
“In the 25 years that I’ve been passionate about helping children with colorectal and pelvic conditions, I’ve learned that collaborative and integrated programs are the best way to care for them,” says Dr. Levitt. “With the broad range of expertise at Children’s National, including the nation’s best NICU, I’m confident that colorectal patients will get better, integrated care faster and more effectively here than anywhere else in the world.”
The program provides diagnosis and treatment for every type of colorectal disorder occurring in infants, children and adolescents, from the most common to the most complex. Every necessary specialty is integrated into the program in one convenient location to provide seamless care for all colon and rectum conditions, with particular expertise in:
“Every child receives a customized treatment plan to address his or her unique needs,” Dr. Levitt says about the program. “Additionally, our surgeons often combine complex procedures across specialties to reduce the number of surgeries a child requires. It isn’t unusual for us to include urology, gynecology, and gastroenterology teams in the operating room alongside the colorectal surgeons so multiple issues can be addressed in a single procedure – we know that when possible, fewer surgeries is always better for the child.”
Dr. Levitt has cared for children from 50 states and 76 countries. He is the founder of Colorectal Team Overseas (CTO), a group of international providers who travel to the developing world to provide care for patients and teaching of their physicians and nurses. He co-founded the Pediatric Colorectal and Pelvic Learning Consortium (PCPLC), an organization of collaborating colorectal centers across the globe.
“We’re absolutely thrilled to welcome Marc Levitt and launch the comprehensive colorectal program under his expert leadership,” adds Anthony Sandler, M.D., surgeon-in-chief and vice president of the Joseph E. Robert, Jr., Center for Surgical Care at Children’s National. “There are few in the world who can provide the expertise and leadership in colorectal diagnoses and treatment that Marc brings with him to Children’s. Many children and families from the region and from around the world will benefit from his expertise and from the program in general.”
Albert Oh, M.D., Director of the Cleft and Craniofacial Program at Children’s National Hospital.
The American Cleft Palate-Craniofacial Association (ACPA) recognized Albert Oh, M.D., with the 2020 Emerging Leader Award. This award is given to professionals who have been members of ACPA between three to 15 years, and who exhibit exemplary accomplishments and dedication to the issues affecting people with cleft and craniofacial conditions.
The ACPA is an association consisting of professionals who treat and/or perform research on cleft and craniofacial conditions. The nonprofit organization also supports those affected through education and resources through its ACPA Family Services program.
As the director of the Cleft and Craniofacial Program at Children’s National Hospital, Dr. Oh is a leader in the research, surgical treatment and holistic care of cleft and craniofacial patients. He has published over 75 peer-reviewed scientific articles and book chapters. Dr. Oh’s current research interests include the outcomes and safety of cleft and craniofacial procedures, 3-D analysis of craniofacial morphology, Pierre Robin sequence and vascular anomalies.
Dr. Oh says that “It is an honor to be recognized by the ACPA and to share their mission of advancing research and improving outcomes for all those affected by cleft and craniofacial conditions.”
Dr. Oh will be presented with his award during the ACPA’s 77th Annual Meeting in Portland, Or.


Fewer than half of California pharmacies provided correct prescription drug disposal details, a percentage that dropped if “secret shoppers” made their call on a weekend, according to a brief research report published online Dec. 31, 2019, in Annals of Internal Medicine.
The callers pretended to be well-meaning parents who were trying to safely dispose of unneeded antibiotics and opioid-based prescription painkillers after their child’s surgery. Fewer than half of the California pharmacies they called provided correct prescription drug disposal details, a percentage that dropped sharply if the “secret shoppers” made their call on a weekend, according to a brief research report published online Dec. 31, 2019, in Annals of Internal Medicine.
“The Food and Drug Administration advises consumers about how to safely dispose of unneeded medicines and, because pharmacists can play an integral role in this conversation, the American Pharmacists Association says prescription medication disposal should follow FDA guidelines,” says Rachel E. Selekman, M.D., MAS, a pediatric urologist at Children’s National Hospital and the study’s first author. “We found very few California pharmacies permitted take-back of unneeded medications. There was also a striking difference in the accuracy and completeness of drug disposal information depending on whether they answered the call on a weekday or a weekend. That suggests room for improvement,” Dr. Selekman says.
The multi-institutional research team, led by Primary Investigator and senior author Hillary L. Copp, M.D., MS, at University of California, San Francisco, identified licensed pharmacies located in urban and rural settings in California. That state that accounts for 10% of all U.S. pharmacies. They wrote a script that guided four male and two female “secret shoppers” to ask about what to do about leftover antibiotics (sulfamethoxazole-trimethoprim tablets) and a liquid opioid-based painkiller (hydrocodone-acetaminophen). From late-February to late-April 2018, they called 898 pharmacies from 8 a.m. to 8 p.m., asking about the correct way to dispose of these medicines.
According to the FDA, consumers should mix most unused medicines with an unappealing substance, like kitty litter, place it in a sealed container and toss the container in the trash. Medicines that can be harmful to others, like opioids, should be flushed down the sink or toilet. Many pharmacies have programs or kiosks to handle unused prescription medicines.
Of the pharmacies surveyed in California:
Asked specifically about drug take-back programs, just 11% said their pharmacy had one that could be used to dispose of antibiotics or opioids.
“Unused prescription medications can be misused by others and can result in accidental childhood poisonings,” Dr. Selekman adds. “The bottom line is that we often talk about how to address the problem of too many unused medications lingering in homes. There are many reasons this is a problem, but part of the problem is nobody knows what to do if they have too many prescription medicines. Because of this research, we have discovered that pharmacies don’t uniformly provide accurate information to our patients. Patients, families and health care professionals who advise families should work together to help improve and expand safe disposal options for these powerful medications.”
In addition to Drs. Selekman and Copp, the research team includes co-authors Thomas W. Gaither, M.D., MAS, Zachary Kornberg, BA, and Aron Liaw, M.D., all of whom were at the University of California, San Francisco, School of Medicine, Division of Pediatric Urology at the time the study was performed.


Earlier this year Michael Tsifansky, M.D., F.A.A.P., joined Children’s National Hospital as an attending physician in the Cardiac Intensive Care Unit and in the Division of Pulmonology and Sleep Medicine. He brings to Children’s National a unique mix of expertise in critical care and pulmonary medicine. That passion for these two subspecialties has also made him one of the country’s leading experts in lung transplant procedures and the recovery from them.
Dr. Tsifansky shared more information about caring for patients with complex lung diseases, especially those with end-stage lung disease. He outlines the patient population for pediatric lung transplants and the arduous process patients endure while waiting for a transplant, undergoing this major procedure, and then recovering from it.
What types of patients undergo lung transplant surgeries?
Lung transplantation in children is indicated when the following criteria are met:
Could you describe the surgery process?
Pediatric lung transplantation may be performed on cardiopulmonary bypass, on extracorporeal membrane oxygenation (ECMO) or off extracorporeal cardiopulmonary support (ECS). The donor’s lungs are kept chilled prior to transplantation and should be transplanted within six to eight hours after removal from the donor. The donor’s main-stem bronchi and pulmonary arteries are connected to those of the recipient, and the donor’s pulmonary venous drainage is connected to the recipient’s left atrium using the donor’s left atrial roof tissue. This procedure typically takes six to eight hours.
Could you describe the recovery process?
Typically, pediatric lung transplant recipients are extubated and encouraged to sit up four to six hours after the transplant procedure and walk soon afterward. It is important that they be out of bed and moving as soon as possible, and our colleague from Rehabilitation Services (physical and occupational therapists and rehabilitation physicians) will be working with the children toward these goals. After transplantation, pediatric patients will be given discharge instructions with individualized guidelines for a healthy lifestyle. Patients should return to near-normal life approximately three to six months after transplantation.
How long does the recovery process take?
The patient will remain hospitalized for 11-14 days following surgery for acute rehab, titration of antirejection meds and initial healing.
You’ve mentioned that it’s important for transplant patients to get moving as part of recovery. When can a patient begin walking again?
Lung recipients will be assisted into a chair soon after the transplant. Within the first 24-36 hours, the patient is encouraged to take short walks, increasing the distance each day. A physical therapist will work with the patient during their hospitalization to meet their goals. We also encourage patients to exercise on the treadmill regularly while hospitalized. By the time the patient is ready to go home, he or she will be able to easily move around by themselves and do most of their care without assistance. They feel so much better than before transplant and have so much energy that we almost always have to gently limit their activity for a short while to allow their chest incision to heal properly.
What do you see as the next step in pulmonary care for end stage lung disease at Children’s National Hospital?
The development of a pediatric-specific lung transplant and respiratory failure program is the natural extension of the hospital’s cystic fibrosis program, heart transplant program and programs in pulmonary hypertension, bronchopulmonary dysplasia and extracorporeal membrane oxygenation for respiratory failure.
At present, there is no local option for a pediatric-specific program that can perform the transplant and provide the necessary comprehensive wrap-around services for patients in infancy up to age 18. As a top children’s hospital, Children’s National is uniquely positioned to provide the highest level of pediatric-specific care to this patient population and allow patients and their families to spend more time at home while undergoing this and other lifesaving treatments.
Dr. Tsifansky hopes to launch a comprehensive pediatric lung transplant and respiratory failure program at Children’s National in the very near future. Stay tuned for future developments from this area.


Born to young parents, no prenatal testing had suggested any problems with Bella’s brain. But just a few hours after birth, Bella suffered her first seizure – one of many that would follow in the ensuing days. After brain imaging, her doctors in Iowa diagnosed her with hemimegalencephaly.
Strokes are neurologically devastating events, cutting off life-sustaining oxygen to regions of the brain. If these brain tissues are deprived of oxygen long enough, they die, leading to critical loss of function – and sometimes loss of life.
“As physicians, we’re taught to prevent or treat stroke. We’re never taught to inflict it,” says Taeun Chang, M.D., director of the Neonatal Neurology and Neonatal Neurocritical Care Program at Children’s National Hospital.
That’s why a treatment developed at Children’s National for a rare brain condition called hemimegalencephaly is so surprising, Dr. Chang explains. By inflicting controlled, targeted strokes, Children’s National physician-researchers have treated five newborns born with intractable seizures due to hemimegalencephaly before they’re eligible for epilepsy surgery, the standard of care. In the four surviving infants, the procedures drastically reduced or completely relieved the infants of hemimegalencephaly’s characteristic, uncontrollable seizures.
The most recent patient to receive this life-changing procedure is Bella, a 13-month-old from Iowa whose treatment at Children’s National began within her second week of life. Born to young parents, no prenatal testing had suggested any problems with Bella’s brain. But just a few hours after birth, Bella suffered her first seizure – one of many that would follow in the ensuing days. After brain imaging, her doctors in Iowa diagnosed her with hemimegalencephaly.
A congenital condition occurring in just a handful of children born worldwide each year, hemimegalencephaly is marked by one brain hemisphere growing strikingly larger and dysplastic than the other, Dr. Chang explains. This abnormal half of the brain is highly vascularized, rippled with blood vessels needed to support the seizing brain. The most conspicuous symptoms of hemimegalencephaly are the numerous seizures that it causes, sometimes several in the course of an hour, which also may prevent the normal half of the brain from developing and learning.
Prior studies suggest early surgery achieves better developmental outcomes with one study reporting as much as a drop of 10-20 IQ points with every month delay in epilepsy surgery.
The standard treatment for unilateral megalencephaly is a dramatic procedure called a hemispherectomy, in which surgeons remove and disconnect the affected half of the brain, allowing the remaining half to take over its neurological duties. However, Dr. Chang says, implementing this procedure in infants younger than 3 months of age is highly dangerous. Excessive, potentially fatal blood loss is likely in infants younger than 3 months who have a highly vascularized brain in the setting of an immature coagulation system. That leaves their doctors with no choice but to wait until these infants are at least 3 months old, when they are more likely to survive the surgery.
However, five years ago, Dr. Chang and her colleagues came up with a different idea when a newborn continued to have several seizures per hour despite multiple IV seizure medications: Because strokes cause irreversible tissue death, it might be possible to effectively incapacitate the enlarged hemisphere from within by inflicting a stroke on purpose. At the very least, this “functional embolization” might buy time for a traditional hemispherectomy, and slow or halt ongoing brain damage until the infants are able to withstand surgery. Ideally, this procedure may be all some children need, knocking out the offending hemisphere completely so they’d never need a hemispherectomy, which has late complications, such as hydrocephalus.
A pediatrician friend of Bella’s paternal grandparents read a story on Children’s National website about Darcy, another baby who’d received functional embolization a year earlier and was doing well. She contacted Dr. Chang to see if the procedure would be appropriate for Bella.
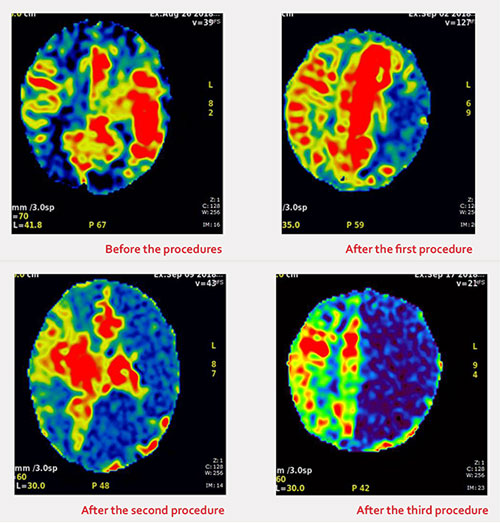
Within days, Bella and her family headed to Washington, D.C., to prepare for functional embolization herself. Within the first weeks of life, Bella underwent three separate procedures, each three to four hours long. Under real-time fluoroscopic and angiographic guidance, interventional neuroradiologist Monica Pearl, M.D., threaded a micro-catheter up from the baby’s femoral artery through the complex network of blood vessels all the way to her brain. There, in targeted branches of her cerebral arteries, Dr. Pearl strategically placed liquid embolic agent to obstruct blood flow to the abnormal half of Bella’s brain.
Immediately after the first procedure, the team had to contend with the same consequences that come after any stroke: brain swelling that can cause bleeding and herniation, complicated further by the already enlarged hemisphere of Bella’s brain. Using neuroprotective strategies learned from treating hundreds of brain-injured newborns, the neonatal neurocritical care team and the neonatal intensive care unit (NICU) minimized the brain swelling and protected the normal half of the brain by tightly controlling the brain temperature, her sugar and electrolyte levels, her blood pressure and coagulation system.
As the brain tissue in the oversized hemisphere died, so did the seizures that had plagued Bella since birth. She has not had a seizure since she left Children’s National more than one year ago. Her adoptive parents report that Bella is hitting many of the typical developmental milestones for her age: She’s getting ready to walk, blowing kisses and saying a few words. Physical, speech and occupational therapy will keep her moving in the right direction, Dr. Chang says.
“We believe that Children’s National is the only place in the world that’s treating newborns in this way to preserve their futures,” Dr. Chang says. “We’re privileged to be able to care for Bella and other kids with this rare condition.”
Bella’s transfer and successful procedures required the support and collective efforts of many within the hospital organization including William D. Gaillard, M.D., and his surgical epilepsy team; interventional neuroradiology with Dr. Monica Pearl; Neurosurgery; Neonatology and the NICU; social work; and even approval from Robin Steinhorn, M.D., senior vice president of the Center for Hospital-Based Specialties, and David Wessel, M.D., executive vice president and Chief Medical Officer.
“While obvious credit goes to the medical team who saved Bella’s future and the neonatal intensive care nurses who provided exceptional, intensive, one-on-one care, Bella’s team of supporters extend to all levels within our hospital,” Dr. Chang adds.
Also read:
|
Bella was born with a rare condition (hemimegalencephaly) in which one half of the brain developed abnormally, causing seizures. The textbook approach is to let babies grow big enough for a dramatic surgery. But Bella’s left hemisphere was triggering so many seizures each hour that waiting would mean her life would be defined by severe disability. Children’s National Hospital is believed to be the only center in the world that calms these seizures through controlled strokes. Procedure one occurred five days after Bella came to Children’s National Hospital from Iowa, when she was 13 days old. The team first optimized control of her seizures and obtained special magnetic resonance images to plan their approach. They glued up the branches of the left posterior cerebral artery and branches of the left middle cerebral artery. Bella had a tiny bleed that was controlled immediately in the angio suite and afterwards in the Children’s National neonatal intensive care unit. Procedure two occurred 10 days later when Bella was 23 days old. The team waited until brain swelling had subsided and brain tissue loss had occurred from the first procedure. This time, they glued up the remaining branches of the left posterior cerebral artery and some branches of the left anterior cerebral artery. The third and final procedure was done nine days later when Bella was 29 days old. This time the team glued and coiled, placing little wire coils where it was unsafe to use glue, getting at the remaining small and numerous branches that remained of the left anterior cerebral artery. Also read: |


Children’s National in Washington, D.C., is the nation’s No. 6 children’s hospital and, for the third year in a row, its neonatology program is No.1 among all children’s hospitals providing newborn intensive care, according to the U.S. News Best Children’s Hospitals annual rankings for 2019-20.
This is also the third year in a row that Children’s National has been in the top 10 of these national rankings. It is the ninth straight year it has ranked in all 10 specialty services, with five specialty service areas ranked among the top 10.
“I’m proud that our rankings continue to cement our standing as among the best children’s hospitals in the nation,” says Kurt Newman, M.D., President and CEO for Children’s National. “In addition to these service lines, today’s recognition honors countless specialists and support staff who provide unparalleled, multidisciplinary patient care. Quality care is a function of every team member performing their role well, so I credit every member of the Children’s National team for this continued high performance.”
The annual rankings recognize the nation’s top 50 pediatric facilities based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
“The top 10 pediatric centers on this year’s Best Children’s Hospitals Honor Roll deliver outstanding care across a range of specialties and deserve to be nationally recognized,” says Ben Harder, chief of health analysis at U.S. News. “According to our analysis, these Honor Roll hospitals provide state-of-the-art medical expertise to children with rare or complex conditions. Their rankings reflect U.S. News’ assessment of their commitment to providing high-quality, compassionate care to young patients and their families day in and day out.”
The bulk of the score for each specialty is based on quality and outcomes data. The process also includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with challenging conditions.
Below are links to the five specialty services that U.S. News ranked in the top 10 nationally:
The other five specialties ranked among the top 50 were cardiology and heart surgery, diabetes and endocrinology, gastroenterology and gastro-intestinal surgery, orthopedics, and urology.


Nichole Jefferson and Patrick O. Gee
African Americans who either donated a kidney, received a kidney donation, are on dialysis awaiting a kidney transplant or have a close relative in one of those categories are helping to perfect a new study that aims to improve outcomes after kidney transplantation.
The study is called APOLLO, short for APOL1 Long-Term Kidney Transplantation Outcomes Network. Soon, the observational study will begin to enroll people who access transplant centers around the nation to genotype deceased and living African American kidney donors and transplant recipients to assess whether they carry a high-risk APOL1 gene variant.
The study’s Community Advisory Council – African American stakeholders who know the ins and outs of kidney donation, transplantation and dialysis because they’ve either given or received an organ or are awaiting transplant – are opening the eyes of researchers about the unique views of patients and families.
Already, they’ve sensitized researchers that patients may not be at the same academic level as their clinicians, underscoring the importance of informed consent language that is understandable, approachable and respectful so people aren’t overwhelmed. They have encouraged the use of images and color to explain the apolipoprotein L1 (APOL1) gene. The APOL1 gene is found almost exclusively in people of recent African descent, however only 13 percent of these people carry the high-risk APOL1 variant that might cause kidney problems.
One issue arose early, during one of the group’s first monthly meetings, as they discussed when to tell patients and living donors about the APOLLO study. Someone suggested the day of the transplant.
“The Community Advisory Council told them that would not be appropriate. These conversations should occur well before the day of the transplant,” recalls Nichole Jefferson.
“The person is all ready to give a kidney. If you’re told the day of transplant ‘we’re going to include you in this study,’ that could possibly stop them from giving the organ,” Jefferson says. “We still remember the Tuskegee experiments. We still remember Henrietta Lacks. That is what we are trying to avoid.”
Patrick O. Gee, Ph.D., JLC, another Community Advisory Council member, adds that it’s important to consider “the mental state of the patient and the donor. As a patient, you know you are able to endure a five- to eight-hour surgery. The donor is the recipient’s hero. As the donor, you want to do what is right. But if you get this information; it’s going to cause doubt.”
Gee received his kidney transplant on April 21, 2017, and spent 33 days in the hospital undergoing four surgeries. His new kidney took 47 days to wake up, which he describes as a “very interesting journey.” Jefferson received her first transplant on June 12, 2008. Because that kidney is in failure, she is on the wait list for a new kidney.
“All I’ve ever known before APOLLO was diabetes and cardiovascular issues. Nobody had ever talked about genetics,” Gee adds. “When I tell people, I tread very light. I try to stay in my lane and not to come off as a researcher or a scientist. I just find out information and just share it with them.”
As he spoke during a church function, people began to search for information on their smart phones. He jotted down questions “above his pay grade” to refer to the study’s principal investigator. “When you start talking about genetics and a mutated gene, people really want to find out. That was probably one of the best things I liked about this committee: It allows you to learn, so you can pass it on.”
Jefferson’s encounters are more unstructured, informing people who she meets about her situation and kidney disease. When she traveled from her Des Moines, Iowa, home to Nebraska for a transplant evaluation, the nephrologist there was not aware of the APOL1 gene.
And during a meeting at the Mayo Clinic with a possible living donor, she asked if they would test for the APOL1 gene. “They stopped, looked at me and asked: ‘How do you know about that gene?’ Well, I’m a black woman with kidney failure.”

Patrick O. Gee received his kidney transplant on April 21, 2017, and spent 33 days in the hospital undergoing four surgeries. His new kidney took 47 days to wake up, which he describes as a “very interesting journey.”
About 100,000 U.S. children and adults await a kidney transplant. APOLLO study researchers believe that clarifying the role that the APOL1 gene plays in kidney-transplant failure could lead to fewer discarded kidneys, which could boost the number of available kidneys for patients awaiting transplant.
Gee advocates for other patients and families to volunteer to join the APOLLO Community Advisory Council. He’s still impressed that during the very first in-person gathering, all researchers were asked to leave the table. Only patients and families remained.
“They wanted to hear our voices. You rarely find that level of patient engagement. Normally, you sit there and listen to conversations that are over your head. They have definitely kept us engaged,” he says. “We have spoken the truth, and Dr. Kimmel is forever saying ‘who would want to listen to me about a genotype that doesn’t affect me? We want to hear your voice.’ ”
(Paul L. Kimmel, M.D., MACP, a program director at the National Institute of Diabetes and Digestive and Kidney Diseases, is one of the people overseeing the APOLLO study.)
Jefferson encourages other people personally impacted by kidney disease to participate in the APOLLO study.
“Something Dr. Kimmel always says is ‘You’re in the room.’ We’re in the room while it’s happening. It’s a line from Hamilton. That’s a good feeling,” she says. “I knew right off, these are not necessarily improvements I will see in my lifetime. I am OK with that. With kidney disease, we have not had advances in a long time. As long as my descendants don’t have to go through the same things I have gone through, I figure I have done my part. I have done my job.”