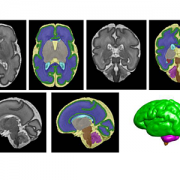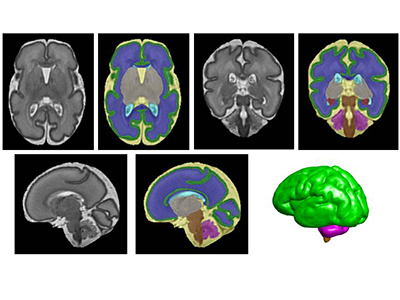
Building “digital twins” to test complicated surgeries
Syed Anwar, Ph.D., is developing self-supervised algorithms for medical imaging.
Syed Anwar, Ph.D., joins the growing AI initiative in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI) at Children’s National Hospital with extensive research experience in machine learning and medical imaging from the University of Engineering and Technology in Taxila, Pakistan, the University of Sheffield, U.K., and the University of Central Florida through the Fulbright Scholars Program. At Children’s National, he’s grateful for the proximity between researchers and clinicians as he studies federated learning and works to build “digital twins” that allow medical teams to test complicated surgical and treatment plans on infants with disorders including Pierre Robin Sequence. This rare congenital birth defect is characterized by an underdeveloped jaw, backward displacement of the tongue and upper airway obstruction. Anwar works alongside Marius George Linguraru, D.Phil., M.A., M.Sc., principal investigator at SZI, and the Precision Medical Imaging Lab to increase AI capacity in all areas of pediatric care at the hospital.
Q: What is the focus of your research work?
A: The main theme is a digital twin. It’s an engineering innovation that people have been using for some time, especially in manufacturing and aviation. For example, you can create a digital simulation of an airplane with a flight simulator. Now, people are starting to use the power of data-driven digital twins for medical applications.
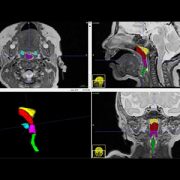
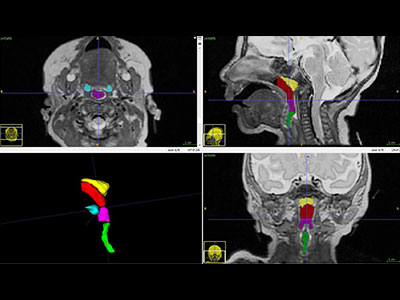
I’m working to create a digital twin for infants born with Pierre Robin Sequence, where they need to have surgical interventions for improving the structure of the bones in the jaws. It includes a lot of clinical approaches, including surgery and ways to address apnea and food intake.
There are multiple areas of clinical expertise involved. With a digital twin, we will have a digital representation of the patient, and the surgeon, the radiologist and other clinicians can experiment with a proposed intervention before actually touching the patient.

Syed Anwar, Ph.D., joins the growing AI initiative in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI) at Children’s National Hospital.
Q: How else are you using your engineering background in your research?
A: Another part of my work is federated learning, which is a type of machine learning. In artificial intelligence, we want big data as the starting point to train our deep learning models. When studying children, this is not always possible because we have smaller data sets.
Federated learning is a tool that helps in these situations. Data is kept at a local site. We train a model to learn from all that data at the different sites. One benefit is that we don’t need to share the data, which is very useful for preserving patient privacy. But you can still apply deep learning models and develop AI solutions using the distributed data for improved clinical outcomes.
Q: What do you see as the main hurdles you have to overcome?
A: For all medical data, and particularly for kids, the amount of data we see in a children’s hospital is small, particularly for rare diseases.
The second hurdle is good, quality labels. For example, if you are doing tumor segmentation, you still need to have some ground rules from a radiologist showing which part of the image is the tumor.
These challenges come together in another focus of my research – self-supervised learning, meaning we can train a machine to learn from the data itself, without the labels or ground rules. From a machine learning point of view, I am in the process of developing self-supervised algorithms for medical imaging and in general for medical data. It’s an amazing time to be in this research area and to enable the translation of AI driven solutions for clinical workflows.
Q: What excites you about being at Children’s National and working at SZI?
A: I come from an engineering background, and my research area has been medical imaging for some time, mainly magnetic resonance imaging. Before coming here, I was working at a university in Pakistan, teaching machine learning and conducting research related to medical imaging and biomedical signal processing. But I was missing strong connections with people caring for patients at the hospital.