

In this webinar, Jared Hershenson, M.D., pediatric cardiologist and medical director of Cardiac Exercise and Rehabilitation at Children’s National Hospital, discussed the importance, methods, challenges and recommendations of pre-participation cardiac screening, as well as secondary prevention and eligibility recommendations for athletes with known congenital heart disease.


This research, published today in JAMA Network Open, marks a significant step forward in making better information available for the 1.5 million adults in the United States who were born with CHD.
For the first time, adults living with congenital heart disease (CHD) now have valuable insights into their long-term quality of life through data from the Congenital Heart Initiative (CHI). CHI is the nation’s first and largest patient-focused registry for adults with CHD and released its first study involving over 4,500 participants from all 50 states.
This research, published today in JAMA Network Open, marks a significant step forward in making better information available for the 1.5 million adults in the United States who were born with CHD.
“Studies like this that leverage actual patient voices and experiences help us get a better sense of how to advise, support and treat people with CHD as they age,” says Anitha John, M.D., Ph.D., director of the Washington Adult Congenital Heart program at Children’s National Hospital and senior author of the study. “Also, researchers get a clearer picture of the questions that need to be answered to make sure they have the best quality of life possible.”
The study also demonstrates two of the most successful models of current promising trends in clinical research:
Key highlights include:
Treatments for children born with congenital heart disease have improved so significantly in the last two decades that life expectancy continues to increase as well.
“There are now more adults living with congenital heart disease than there are children with CHD,” says Scott Leezer, patient co-principal investigator for the Congenital Heart Initiative registry and co-author of the study. “However, a significant gap remains in what we know about the adult CHD population. As an adult CHD patient, I was excited to contribute to creating this registry, bringing more answers to people like me who want to know how our unique hearts impact our bodies and quality of life over time.”
The authors note that the study’s findings and the registry data currently have a few limitations. First, the registry only contains patient-reported outcomes and no clinical data. The first sub-study of the CHI, the CHI-RON study, addresses this challenge by incorporating additional data sources for a subset of consenting CHI participants.
Additionally, recall bias, underlying neurocognitive challenges and survey fatigue, may have limited participation in the CHI to a smaller subset of adults with CHD. Efforts are underway to develop methods for people with congenital heart disease who have neurodevelopmental deficits or other disabilities to engage in the registry. The CHI is temporarily closed to new registrants as the study team redesigns the study to better align with the needs of the community.
“We are grateful for everyone who joined this registry, answered survey questions and shared their experiences,” says Thomas Carton, Ph.D., chief data officer at Louisiana Public Health Institute and study co-author. “The CHI registry is a big step forward for adults with CHD, but also can serve as a model for how to bring together physicians, researchers and patients as active participants in care, research and advocacy.”
As the registry grows in the future, it will focus on increasing diversity of participants, developing additional partnerships with other organizations, continued innovation in data usage and improved community engagement, all with the goal of guiding future research that will ultimately improve quality of life for all adults with CHD.

 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
This year, U.S. News ended ordinal rankings on its Honor Roll. Instead of assigning a numerical rank from 1 to 10, all hospitals on the Honor Roll will be recognized as having attained the highest standards of care in the nation.
In addition, Children’s National tied for #1 pediatric hospital in the Mid-Atlantic region, which includes New York, New Jersey, Delaware, Pennsylvania, the District of Columbia, West Virginia and Virginia. It’s also best in the Mid-Atlantic in Neonatology.
For the fourteenth straight year, Children’s National ranked in 10 specialty services. New this year, U.S. News included behavioral health as a service line in the rankings. Since it’s the first year, there are no ordinal rankings for behavioral health, but the Children’s National program was named one of the top 50 programs in the country.
“In my first year here, I witnessed what makes Children’s National so special — our commitment to collaboration, empowering one another, and charting a bold path forward for pediatric care,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “I’m proud U.S. News again recognized Children’s National as one of the top in the nation and the highest-ranked pediatric hospital in D.C., Maryland and Virginia. Together, we’ll continue to push the boundaries of care, research and innovation to make a difference for those who matter most — the kids.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“For nearly two decades, U.S. News has published Best Children’s Hospitals to empower the parents and caregivers of children with complex medical needs,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Children’s hospitals appearing on the U.S. News Honor Roll have a track record of delivering unparalleled specialized care.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
The other four specialties ranked among the top 50 are Behavioral Health, Cardiology and Heart Surgery, Pulmonology and Lung Surgery, and Urology.
The project will study the best engagement methods on how to include adults who have both congenital heart disease and neurodevelopmental disorders in the Congenital Heart Initiative (CHI), the first global, patient-powered registry for adults with congenital heart disease.
A first-of-its-kind study focused on including adults with congenital heart disease (CHD) and neurodevelopmental disabilities in patient-reported outcome research has been approved for $2.1 million in funding from the Patient-Centered Outcomes Research Institute (PCORI).
The study, Achieving Equity: Inclusion of Adults with Congenital Heart Disease (CHD) Living with Neurodevelopmental Disorders (NDDs) in Patient Centered Outcomes Research, is led by Anitha John, M.D., Ph.D., at Children’s National Hospital, together with partners from a range of academic, scientific and patient advocacy perspectives.
The project will study the best engagement methods on how to include adults who have both congenital heart disease and neurodevelopmental disorders in the Congenital Heart Initiative (CHI), the first global, patient-powered registry for adults with congenital heart disease. In its current form, individuals with developmental disabilities are often excluded, as they are unable to complete the surveys independently.
Building upon Dr. John’s previous collaborations, the project features a shared leadership model with partners from across the United States.
Leading the study with Dr. John, William Bennett, M.D., (Indiana University) provides expertise in patient engagement research and big data and will serve as dual principal investigator (PI).
The project also utilizes the strengths and long-standing connections with PCORnet®, the National Patient-Centered Clinical Research Network, with Thomas Carton, Ph.D., (Louisiana Public Health Institute/REACHnet) serving as the PCORnet PI, Jamie Jackson, Ph.D., (Nationwide Children’s Hospital/PEDSnet) serving as a scientific PI with psychology expertise, Arwa Saidi, M.B.B.Ch., M.Ed., (University of Florida/OneFlorida) and Emily Ruckdeschel, M.D., (CHOP/PEDSnet) serving as recruiting site PIs.
The Adult Congenital Heart Association (ACHA) continues as part of the leadership team, represented by two parent co-PIs along with the Cardiac Neurodevelopmental Outcomes Collaborative (CNOC), represented by Thomas Miller, D.O., (Maine Medical) and CURA strategies, represented by Scott Leezer.
The study was selected for support through a groundbreaking PCORI funding announcement focused on building an evidence base to support development of measures and approaches that strengthen meaningful engagement in comparative clinical effectiveness research. Much has been learned in recent years about participatory research that seeks to involve the end users of study results, including patients, caregivers, clinicians and others, as partners in the research process. But there has been little systematic study about which engagement techniques are most effective.
Although nearly 2 million adults in the United States are living with a congenital heart defect — more adults than children — it has been historically difficult to gather data on people with these conditions and to identify patient needs, especially in those with neurodevelopmental disabilities. Despite significant investment in cardiac neurodevelopmental programs across North America, CNOC has identified large gaps in current infrastructure to provide a continuum of neurodevelopmental care into adulthood.
Even more challenging is ensuring that the data is representative of the entire population of people living with these conditions. According to a 2024 Scientific Statement from the American Heart Association, “Although not every individual with congenital heart disease will have a developmental delay or disorder, neurodevelopmental deficits rank among the most enduring and impactful complications faced by individuals with complex congenital heart disease.”
Unfortunately, this critical subgroup remains underrepresented even in inclusive efforts such as CHI. Currently to be eligible for the CHI, participants must be able to complete the CHI’s patient-reported outcome tools independently. Individuals with CHD and neurodevelopmental disorders are often ineligible to participate.
The lack of engagement methods to effectively incorporate patients with developmental disabilities presents a major gap in the science of engagement research that hinders a full understanding of the long-term outcomes of all patients with CHD.
This work to engage and capture the experiences of the most vulnerable adults with CHD will be an important enhancement to the CHI and will build upon the work of an ongoing sub-study of the CHI that uses PCORnet®, the National Patient-Centered Clinical Research Network, the CHI-RON study (PCORI RD-2020C2-20347).
The award has been approved pending completion of a business and programmatic review by PCORI staff and issuance of a formal award contract.
PCORI is an independent, nonprofit organization authorized by Congress in 2010. Its mission is to fund research that will provide patients, their caregivers and clinicians with the evidence-based information needed to make better-informed healthcare decisions.

The Congenital Heart Initiative (CHI) is celebrating its third year as the first global patient-powered registry for adults with congenital heart disease (CHD). In 2023, the registry surpassed recruitment targets and launched a data intake process to allow researchers from around the world to submit proposals for patient-centered research and programs around the critical questions for adults with CHD who had their hearts repaired in childhood.
By recruiting over 4,600 participants in all 50 states and 37 countries, the CHI is now the largest patient-powered registry for adults with congenital heart disease. This is the first time researchers and clinicians have been able to access this type of robust data set to help them better understand and address the needs of people with CHD as they continue to age. Even better, the registry’s mechanisms allow for routine feedback and input about priorities directly from the growing patient population.
“Patient-centered research organizations, not providers or universities, have the greatest ability to lead this charge and lay the foundation for future breakthroughs. The inspiring efforts of all participants to date gives me hope that the next generation of advances is within reach,” says Matthew Lewis, M.D., an adult congenital heart specialist and CHI-RON site PI from Columbia University Medical Center.
An ongoing sub-study of CHI uses PCORnet®, the National Patient-Centered Clinical Research Network, to better understand how gaps in care impact the adult patient experience with CHD. The CHI-RON study (PCORI RD-2020C2-20347) fills in these gaps by exploring three distinct data types: patient-reported outcomes, health insurance claims and electronic health records. The effort is led by Children’s National Hospital and Louisiana Public Health Institute.
This year, CHI also launched some of its first studies, focused on pregnancy, health disparities and long-term health care follow-ups. The first academic manuscripts about these studies are expected to publish in the next year.
Although nearly 2 million adults in the United States are living with a congenital heart defect — more adults than children in fact — it’s been historically difficult to gather data on these conditions and to identify patient needs.
As children born with CHD become adults, they have a lot of worry and uncertainty about their limitations and abilities to achieve what might be considered common adult milestones. The research made possible by this registry and the mechanisms to communicate findings to both the participants and the larger clinical community will make a big difference in quality of life and hope to provide more answers to these important questions.
The CHI related meetings have allowed a space where patients and researchers can come together to discuss research priorities.
“Once you go and look at things from the patient’s point of view, there is no going back. It is going to be something that will redefine you as a researcher and a provider,” says Rohan D’Souza, M.D., a maternal-fetal medicine specialist who is an active participant in a PCORI-funded maternal health consortium focused on reducing maternal morbidity and mortality in CHD patients (PCORI EACB-23293).
Additionally, because people with CHD live all over the United States and the world, it can be hard for them to connect with each other to share common questions and experiences with clinicians and each other. The patient-driven registry engages participants and hopes to help make greater connections between people who live with CHD. A key registry partner, the Adult Congenital Heart Association (ACHA), helps create opportunities, such as virtual Coffee Hours, for people in the registry to weigh in on research priorities and share feedback about CHI’s work.
“The ACHA Cafe was born out of a need for connection,” says Aliza Marlin, who founded and organized the café project on behalf of the ACHA. “A virtual social hour, coffee optional, gave the ACHD community a safe space to come together. Using it as a conduit to the Congenital Heart Initiative gave us an empowered voice in our own futures. It’s the perfect example of social connection leading to transformative possibilities.”
Anitha John, M.D., medical director of the Washington Adult Congenital Heart Program and an adult congenital cardiologist at Children’s National Hospital who leads CHI, says that the future looks bright for the registry and the vital information it can provide.
The new data intake process launched this year, she adds, gives anyone with an interest the ability to submit ideas for new grants, projects and studies. The team will also continue to engage with registry participants, researchers and the centers who provide care for people with CHD, all with the goal of finding more answers to the key questions about how to accomplish specific goals, such as improving mental health, the health care transition and overall quality of life for adults with CHD. For more information on how to get involved, please email ACHDresearch@childrensnational.org.

 Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
For the thirteenth straight year, Children’s National also ranked in all 10 specialty services, with eight specialties ranked in the top 10 nationally. In addition, the hospital was ranked best in the Mid-Atlantic for neonatology, cancer, neurology and neurosurgery.
“Even from a team that is now a fixture on the list of the very best children’s hospitals in the nation, these results are phenomenal,” said Kurt Newman, M.D., president and chief executive officer of Children’s National. “It takes a ton of dedication and sacrifice to provide the best care anywhere and I could not be prouder of the team. Their commitment to excellence is in their DNA and will continue long after I retire as CEO later this month.”
“Congratulations to the entire Children’s National team on these truly incredible results. They leave me further humbled by the opportunity to lead this exceptional organization and contribute to its continued success,” said Michelle Riley-Brown, MHA, FACHE, who becomes the new president and CEO of Children’s National on July 1. “I am deeply committed to fostering a culture of collaboration, empowering our talented teams and charting a bold path forward to provide best in class pediatric care. Our focus will always remain on the kids.”
“I am incredibly proud of Kurt and the entire team. These rankings help families know that when they come to Children’s National, they’re receiving the best care available in the country,” said Horacio Rozanski, chair of the board of directors of Children’s National. “I’m confident that the organization’s next leader, Michelle Riley-Brown, will continue to ensure Children’s National is always a destination for excellent care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“For 17 years, U.S. News has provided information to help parents of sick children and their doctors find the best children’s hospital to treat their illness or condition,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Children’s hospitals that are on the Honor Roll transcend in providing exceptional specialized care.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The eight Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
The other two specialties ranked among the top 50 were cardiology and heart surgery, and urology.

“By the time a baby is diagnosed with bronchopulmonary dysplasia, families have already had a long journey with prematurity in the neonatal intensive care unit (NICU),” says Hallie Morris, M.D., neonatologist and lead of the Complex Bronchopulmonary Dysplasia (BPD) Program at Children’s National Hospital. “To be able to have a team that is focused on the holistic health of their child in the context of this diagnosis makes a world of difference to these families.”
Some premature infants with BPD experience more severe respiratory disease with comorbidities associated with their underlying disease processes, but also factors related to their lengthened intensive care unit (ICU) stay. This includes delayed development with neurodevelopmental impairment, ICU delirium, pulmonary hypertension, airway disease, gastroesophageal reflux disease, feeding difficulties, retinopathy of prematurity and more.
The Complex BPD Program at Children’s National encompasses a group of specialists dedicated to improving the care of infants with BPD and other chronic lung disease of infancy. BPD places extreme demands on families. Education is a critical component for families and our team works to make sure they are well informed, have realistic expectations and understand their care plan.
Learn more about the Complex BPD Program.
“Hybrid treatment enables even patients who are extremely high risk for surgery to have a survival advantage.” — Dr. Yerebakan.
Can Yerebakan, M.D., Ph.D., associate chief of Cardiac Surgery, and Joshua Kanter, M.D., director of Interventional Cardiology, created a multi-disciplinary team at Children’s National Hospital to perform the staged surgical approach known as the “hybrid strategy” to support the smallest, most fragile babies born with hypoplastic left heart syndrome (HLHS).
Today, the team performs more of these procedures than almost any other heart center in the United States, and they’ve successful completed it for neonates as small as 1 kg.
The approach gives high-risk babies time to recover from birth trauma and continue developing crucial organs before undergoing more traditional, more-invasive HLHS procedures that require open-heart surgery with cardiopulmonary bypass. Surgeons also have more time to make complete individualized risk assessments for next steps on each case, replacing the historical “one size fits all” operative pathway for HLHS.
Read more about the hybrid surgical strategy for HLHS.
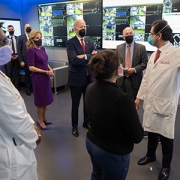









President Joe Biden and First Lady Jill Biden paid a recent visit to the Cardiac Intensive Care Unit (CICU) at Children’s National Hospital, where leaders of our cardiology services toured them through the state-of-the-art telehealth command center embedded on the unit.
Children’s National is pioneering the integration of telemedicine into CICU care. It’s one of the few pediatric hospitals in the world to do this.
Experts liken the telehealth command center to an ‘air traffic control tower’ for the most vulnerable patients with critical heart disease. The President and First Lady saw how complex the environment is, with real-time monitoring of all 26 high-risk patients in the CICU. The system combines traditional remote monitoring, video surveillance and artificial intelligence tools.
“With this technology, we’re helping to predict and prevent major adverse events,” said Ricardo Munoz, M.D., executive director of the Telemedicine Program and chief of the Division of Critical Care Medicine at Children’s National. “For example, our neuromonitoring system can help signal an impending brain injury before it happens.”
Dr. Munoz says President Biden expressed interest in the prevention strategy of adverse events and this new approach to caring for children with critical cardiac illness.
Dr. Ansong hopes bringing awareness of these cardiac capabilities to the President and First Lady is the first of many steps in seeking support for children with congenital and acquired heart disease.

The first patient-powered registry for adults living with congenital heart disease (CHD) — the Congential Heart Initiative (CHI) — celebrates a major milestone this month. In the two years since it was launched in December 2020, the registry has enrolled more than 3,227 adults with CHD from all 50 states and 28 countries.
Although nearly 2 million adults in the United States are living with a congenital heart defect — more adults than children in fact — it’s been historically difficult to gather data on these conditions and to identify patient needs.
“We developed this registry together with numerous patients and providers so it could become a platform for increasing our knowledge and improving care,” says Anitha John, M.D., medical director of the Washington Adult Congenital Heart Program and an adult congenital cardiologist at Children’s National Hospital, who helped drive the registry’s creation. “We want it to become a resource for patients and researchers, a place where they can learn more about what it means for adults who had their hearts repaired in childhood to live a long, healthy life.”
As the treatments for children with CHDs have improved, people born with them are living longer and longer. That means that as they become adults, they have a lot of worry and uncertainty about their limitations and abilities to achieve what might be considered common adult milestones.
“Over the past two years, more than 3,000 adult congenital heart disease (ACHD) patients from around the world, including myself, have worked to support ACHD research by participating in the Congenital Heart Initiative (CHI),” says Scott Leezer, a single-ventricle heart defect patient and co-leader of research and advocacy for the Initiative. “This selfless and simple effort has produced an investment in improving our collective understanding of adult patients living with CHD. We hope these investments will pay dividends in helping guide new research strategies for future generations of CHD patients.”
Participants in the registry receive regular newsletters, highlighting findings and providing access to patient specific resources including content from the Adult Congenital Heart Association (ACHA), a key partner. The ACHA collaboration has also given registry participants the opportunity to interact with other people – a key request identified as important based on input from people who have already registered.
“There is no ’one-size-fits-all’ answer for adults with CHD,” Dr. John adds.
“While other CHD registries exist, they are provider-based and not patient-powered,” said John. “The CHI registry is driven by patients, supporting research but also providing information based on what is important according to the people with CHD themselves.”
A sub-study of the CHI will use PCORnet®, the National Patient-Centered Clinical Research Network, to better understand how gaps in care impact the adult patient experience with CHD. The CHI-RON study, which stands for Congenital Heart Initiative: Redefining Outcomes and Navigation to Adult-Centered Care, will be the first of its kind to fill in these knowledge gaps by exploring three distinct types of data at once: patient reported outcomes, health insurance claims and electronic health records (EHR). The effort is led by Children’s National and Louisiana Public Health Institute.
“PCORnet is a fantastic resource to help us fully understand the impact of gaps in CHD care,” said Tom Carton, dual-principal investigator of CHI-RON and chief data officer at the Louisiana Public Health Institute. “It is essentially turbo-charging our patient-reported data with two additional layers of insights from claims and EHRs, unlocking answers that would be impossible to achieve in isolation.”
In terms of research, the CHI now has enough participants to allow researchers to complete some important studies about pregnancy, mental health and long-term health care follow ups, all of which will kick off within the next year. The research teams hope to engage centers across the United States to better determine the needs of individual ACHD centers and to understand how the CHI can help with these needs.
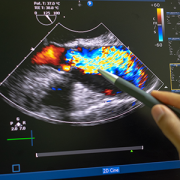
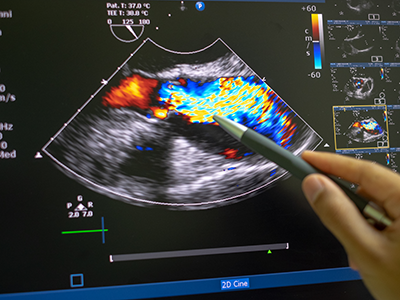
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians.
Researchers at Children’s National Hospital have created a new artificial intelligence (AI) algorithm that promises to be as successful at detecting early signs of rheumatic heart disease (RHD) in color Doppler echocardiography clips as expert clinicians. Even better, this novel model diagnoses this deadly heart condition from echocardiography images of varying quality — including from low-resource settings — a huge challenge that has delayed efforts to automate RHD diagnosis for children in these areas.
Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
Though widely eradicated in nations such as the United States, rheumatic fever remains prevalent in developing countries, including those in sub-Saharan Africa. Recent studies have shown that, if detected soon enough, a regular dose of penicillin may slow the development and damage caused by RHD. But it has to be detected.
Diagnosing RHD requires an ultrasound image of the heart, known as an echocardiogram. However, ultrasound in general is very variable as an imaging modality. It is full of texture and noise, making it one of the most challenging to interpret visually. Specialists undergo significant training to read them correctly. However, in areas where RHD is rampant, people who can successfully read these images are few and far between. Making matters worse, the devices used in these low resource settings have their own levels of varying quality, especially when compared to what is available in a well-resourced hospital elsewhere.
The research team hypothesized that a novel, automated deep learning-based method might detect successfully diagnose RHD, which would allow for more diagnoses in areas where specialists are limited. However, to date, machine learning has struggled the same way the human eye does with noisy ultrasound images.
Using approaches that led to successful objective digital biometric analysis software for non-invasive screening of genetic disease, researchers at the Sheikh Zayed Institute for Pediatric Surgical Innovation, including medical imaging scientist Pooneh Roshanitabrizi, Ph.D., and Marius Linguraru, D.Phil., M.A., M.Sc., principal investigator, partnered with clinicians from Children’s National Hospital, including Craig Sable, M.D., associate chief of Cardiology and director of Echocardiography, and cardiology fellow Kelsey Brown, M.D., who are heavily involved in efforts to research, improve treatments and ultimately eliminate the deadly impacts of RHD in children. The collaborators also included cardiac surgeons from the Uganda Heart Institute and cardiologists from Cincinnati Children’s Hospital Medical Center.
Dr. Linguraru’s team of AI and imaging scientists spent hours working with cardiologists, including Dr. Sable, to truly understand how they approach and assess RHD from echocardiograms. Building the tool based on that knowledge is why this tool stands apart from other efforts to use machine-learning for this purpose. Orienting the approach to the clinical steps of diagnosis is what led to the very first deep learning algorithm that diagnoses mild RHD with similar success to the specialists themselves. After the platform was built, 2,136 echocardiograms from 591 children treated at the Uganda Heart Institute fed the learning algorithm.
The team will continue to collect data points based on clinical imaging data to refine and validate the tool. Ultimately, researchers will look for a way that the algorithm can work directly with ultrasound/echocardiogram machines. For example, the program might be run through an app that sits on top of an ultrasound device and works on the same platform to communicate directly with it, right in the clinic. By putting the two technologies together, care providers on the ground will be able to diagnose mild cases and prescribe prophylactic treatments like penicillin in one visit.
The first outcomes from the program were showcased in a presentation by Dr. Roshanitabrizi at one of the biggest and most prestigious medical imaging and AI computing meetings — the 25th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI).
 Children’s National Hospital named Ricardo Munoz, M.D., the MacCutcheon Family Professor in Cardiac Critical Care Medicine at Children’s National Hospital.
Children’s National Hospital named Ricardo Munoz, M.D., the MacCutcheon Family Professor in Cardiac Critical Care Medicine at Children’s National Hospital.
Dr. Munoz serves as chief of the Division of Cardiac Critical Care Medicine, executive director of Telehealth, and co-director of Children’s National Heart Institute at Children’s National Hospital. He is professor of pediatrics at the George Washington University School of Medicine and the main editor of several books in pediatric cardiac critical care medicine.
Dr. Munoz joins a distinguished group of 42 Children’s National physicians and scientists who hold an endowed chair. Professorships at Children’s National support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and donor’s forethought to advance and sustain knowledge.
As chief of the Division of Cardiac Critical Care Medicine, Dr. Munoz leads a multidisciplinary team of specially trained physicians in providing intensive pediatric cardiac critical care. Dr. Munoz is credited as pioneering telemedicine for pediatric critical care, dedicated to increasing access and quality care for children with special hearts in the nation’s capital and across the world.
The MacCutcheon Family Foundation, through their vision and generosity, are ensuring that Dr. Munoz and future holders of this professorship will launch bold, new initiatives to rapidly advance the field of pediatric cardiac critical care, elevate our leadership and improve the lifetimes of children with special hearts.
Jim MacCutcheon’s involvement with Children’s National dates back to 1983. He has served in many leadership positions, most notably on the Children’s National and Children’s National Hospital Foundation board of directors. Jim and his daughters, Megan MacCutcheon, Candice Kessler and Colleen Crowley have supported Children’s National Heart Institute by funding the development of the MacCutcheon Cardiovascular Operating Suite and the Halle MacCutcheon Playroom on the heart and kidney unit. They have also provided support for the Peter Holbrook Endowed Lecture in Critical Care Medicine, the mobile health clinic and various events and capital improvement projects.
The MacCutcheon family’s investment to establish the MacCutcheon Family Professorship in Cardiac Critical Care Medicine allows Dr. Munoz and his team to provide innovative care utilizing telemedicine and artificial intelligence in support of our patients with special hearts.
Children’s National Hospital named Mary Donofrio, M.D., FAAP, FACC, FASE, as The Van Metre Companies Professor of Fetal Cardiology at Children’s National Hospital.
Children’s National Hospital named Mary Donofrio, M.D., FAAP, FACC, FASE, as The Van Metre Companies Professor of Fetal Cardiology at Children’s National Hospital.
Dr. Donofrio serves as Medical Director of the Prenatal Cardiology Program and Critical Care Delivery Program, Director of the Advanced Cardiac Imaging Fellowship and Co-Director of the Cardiac Neurodevelopmental Outcome Program at Children’s National. She is a Professor of Pediatrics at George Washington University and is the founding and current President of the Fetal Heart Society, a non-profit organization created to advance the field of fetal cardiovascular care and science through collaborative research, education and mentorship.
Dr. Donofrio joins a distinguished group of 42 Children’s National physicians and scientists who hold an endowed chair. Professorships at Children’s National support groundbreaking work on behalf of children and their families and foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflect the recipient’s achievements and donor’s forethought to advance and sustain knowledge.
Dr. Donofrio is an international expert in fetal cardiology. She specializes in the fetal diagnosis and assessment of cardiovascular disease and the in-utero and delivery room management of newborns with complex congenital heart disease (CHD). Dr. Donofrio created an evidenced-based risk-assessment protocol for delivery room management which is now the standard of care for newborns with CHD. Dr. Donofrio has been a co-investigator on several NIH sponsored studies assessing in utero factors that influence neurodevelopmental outcome in children with CHD and more recently a study designed to minimize brain injury during heart surgery using cardiopulmonary bypass. She has published more than 130 papers, including the American Heart Association Scientific Statement on the Diagnosis and Treatment of Fetal Cardiac Disease.
The Van Metre Companies, through their vision and generosity, are ensuring that Dr. Donofrio and future holders of this professorship will launch bold, new initiatives to rapidly advance the field of fetal cardiology, elevate our leadership and improve the lifetimes of children with special hearts.
For the past 65 years, Van Metre Companies has remained one of the Greater Washington D.C. area’s most successful, private, multi-faceted real estate developers. Albert G. Van Metre, the founder of Van Metre Companies, established a tradition of philanthropy focused on local charities. As a homegrown business, perpetuating that legacy of local giving is both a responsibility and a source of pride. The Van Metre Companies Professor of Fetal Cardiology honors Albert G. Van Metre’s memory by continuing this tradition of commitment to the community they call home.
The Van Metre Companies hosts the Annual Van Metre 5K Run in support of Children’s National, a longstanding tradition that has raised nearly $3 million in the past 30 years. In 2010, Children’s National dedicated the Van Metre Companies Cardiovascular Surgery Operating Room, a state-of-the-art cardiovascular surgery suite which was funded through the Annual Van Metre 5K Run. They also established The Van Metre Companies Professorship in Cardiology held by Charles Berul, M.D., Chief of Cardiology and Co-director of Children’s National Heart Institute.

 Children’s National Hospital in Washington, D.C., was ranked No. 5 nationally in the U.S. News & World Report 2022-23 Best Children’s Hospitals annual rankings. This marks the sixth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide. In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the sixth year in a row.
Children’s National Hospital in Washington, D.C., was ranked No. 5 nationally in the U.S. News & World Report 2022-23 Best Children’s Hospitals annual rankings. This marks the sixth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide. In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the sixth year in a row.
For the twelfth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“In any year, it would take an incredible team to earn a number 5 in the nation ranking. This year, our team performed at the very highest levels, all while facing incredible challenges, including the ongoing pandemic, national workforce shortages and enormous stress,” said Kurt Newman, M.D., president and chief executive officer of Children’s National. “I could not be prouder of every member of our organization who maintained a commitment to our mission. Through their resilience, Children’s National continued to provide outstanding care families.”
“Choosing the right hospital for a sick child is a critical decision for many parents,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “The Best Children’s Hospitals rankings spotlight hospitals that excel in specialized care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The seven Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
The other three specialties ranked among the top 50 were cardiology and heart surgery, gastroenterology and gastro-intestinal surgery, and urology.


“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
Penicillin, a widely available and affordable antibiotic, may be one key to turning the tide on the deadly impacts of rheumatic heart disease (RHD) for children in developing nations. This according to the new findings of a large-scale, randomized controlled trial completed in Uganda and published in the New England Journal of Medicine.
The most devastating feature of RHD is severe heart valve damage that is caused by rheumatic fever — a condition that results from the body’s immune system trying to fight poorly treated, repeat infections from streptococcus bacteria, also known as strep throat. Though widely eradicated in nations such as the United States due to the swift detection and treatment of strep throat, rheumatic fever remains prevalent in developing countries including those in sub-Saharan Africa. Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
The study was led by an international panel of pediatric cardiac experts from institutions including Children’s National, Cincinnati Children’s Medical Center, the Uganda Heart Institute and Murdoch Children’s Research Institute in Melbourne, Australia.
“Our study found a cheap and easily available penicillin can prevent progression of latent rheumatic heart disease into more severe, irreversible valve damage that is commonly seen in our hospitals with little or no access to valve surgery,” said co-lead author Emmy Okello, M.D., chief of Cardiology at the Uganda Heart Institute.
To Andrea Beaton, M.D., associate professor of Cardiology at Cincinnati Children’s and co-lead author, this is the first contemporary randomized controlled trial in rheumatic heart disease. “The results are incredibly important on their own, but also demonstrate that high-quality clinical trials are feasible to address this neglected cardiovascular disease,” she said.
Beaton et al. named the trial Gwoko Adunu pa Lutino (GOAL), which means “protect the heart of a child.” The study enrolled 818 Ugandan children and adolescents ages 5 to 17 years old who were diagnosed with latent rheumatic heart disease to see if an injection of penicillin was effective at preventing their heart condition from worsening.
“There are many challenges with recruitment and retention of trial participants in areas like our study region in Uganda,” said Dr. Sable. “But it is critical to work together and overcome barriers, because we must study these treatments in the people most affected by the condition to understand how they, and others like them, may benefit from the findings.”
Of the 799 participants who completed the trial, the group receiving a prophylactic injection of penicillin (399 volunteers) had three participants show evidence of worsened rheumatic heart disease on repeat echocardiogram after two years. In contrast, 33 of the 400 volunteers in the control group, who received no treatment, showed similar progression on echocardiogram results.
Professor Andrew Steer, who is theme director of Infection and Immunity at Murdoch Children’s Research Institute in Melbourne and who served as senior author of the study, said screening for latent rheumatic heart disease was critical to stop progression because heart valve damage was largely untreatable. “Most patients are diagnosed when the disease is advanced and complications have already developed. If patients can be identified early, there is an opportunity for intervention and improved health outcomes.”
The results were shared in a special presentation at the American Heart Association’s Scientific Sessions on the same day that the findings were published in the New England Journal of Medicine.
The trial was supported by the Thrasher Pediatric Research Fund, Gift of Life International, Children’s National Hospital Foundation: Zachary Blumenfeld Fund, Children’s National Hospital Race for Every Child: Team Jocelyn, the Elias/Ginsburg Family, Wiley-Rein LLP, Phillips Foundation, AT&T Foundation, Heart Healers International, the Karp Family Foundation, Huron Philanthropies and the Cincinnati Children’s Hospital Heart Institute Research Core.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:
Two Children’s National Hospital cardiac care leaders received prestigious recognition awards from the American Academy of Pediatrics (AAP) during that organization’s virtual National Conference and Exhibition in October 2021.

Gil Wernovsky, M.D., received the 2021 Maria Serratto Master Educator Award from AAP Section on Pediatric Cardiology and Cardiac Surgery.
The Master Educator Award is presented each year to a pediatric cardiologist or cardiothoracic surgeon who exemplifies excellence as an educator, mentor and/or leader in the field.
A practicing cardiac critical care specialist with more than 30 years’ experience in pediatric cardiology, Dr. Wernovsky trained and mentored more than 300 fellows in pediatric cardiology, cardiac surgery, neonatology, critical care medicine and cardiac anesthesia, in addition to countless residents and fellows. He also organizes national and international symposia to share expertise around the world. During the COVID-19 public health emergency, for example, he co-founded the Congenital Heart Academy (CHA). The CHA provides content from an international faculty of cardiac care to more than 26,000 practitioners in 112 countries and includes a thriving YouTube channel.
Dr. Wernovsky is also a founding member of several international societies focused on bringing together clinicians, researchers and students across sub-specialties of pediatric cardiology and cardiac surgery for knowledge exchange and best practice sharing. These include: the Pediatric Cardiac Intensive Care Society, World Society for Pediatric and Congenital Heart Surgery, the International Society of Pediatric Mechanical Circulatory Support and the Cardiac Neurodevelopmental Outcome Collaborative.
Dr. Wernovsky received the award on October 10 at the virtual Scientific Sessions of the 2021 American Academy of Pediatrics National Conference and Exhibition.
Gerard Martin, M.D., FAAP, FACC, FAHA, C. Richard Beyda Professor of Cardiology, Children’s National Hospital, received the AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award.
The Section on Advances in Therapeutics and Technology (SOATT) educates physicians, stimulates research and development and consults on therapeutics and technology-related matters for the AAP. The Achievement Award recognizes someone who has shown leadership in applying innovative approaches to solve pressing problems.
Dr. Martin is the C. Richard Beyda Professor of Cardiology and has cared for children at Children’s National for more than 30 years. As an advocate for congenital heart disease efforts nationally and internationally, he played an integral role in the development of an innovative use of existing hospital technology—the pulse oximeter—to detect critical congenital heart disease in newborn babies.
Today, Dr. Martin and colleagues across the United States and around the world have worked to make this screening method a standard of care for newborns everywhere. It is a part of the Health Resources and Services Administration (HRSA) Recommended Uniform Screening Panel and has become law in every state. They continue to conduct research to refine the recommendations and hone-in on the most effective ways to harness these tools.
Dr. Martin was selected for this award in 2020. He accepted it and offered remarks during the 2021 virtual AAP National Conference and Exhibition on Monday, October 11, 2021.

An article published in the journal Cardiology in the Young provides a comprehensive timeline mapping the growth trajectory of cardiology and cardiac surgery at one of the nation’s oldest children’s hospitals — Children’s National Hospital in Washington, D.C.
Cardiology and cardiac surgery at Children’s National have grown exponentially in the nearly 80 years since the first heart-related surgery was recorded in 1942. Today, aligned with the growth trajectory of the hospital as it has evolved to become one of the top-ranked pediatric institutions in the country, the Children’s National Heart Institute has also evolved. In the last year, this included welcoming new Cardiac Surgery Chief, Yves d’Udekem, M.D., Ph.D.
The authors, Gerard Martin, M.D., M.A.C.C., C.R. Beyda Professor of Cardiology, and Richard Jonas, M.D., emeritus chief of Cardiac Surgery, both from Children’s National Hospital, note that this history of care has laid the groundwork for the Heart Institute to continue growing and caring for more neonates, infants, children and adults with congenital heart disease in the entire mid-Atlantic region and around the world.
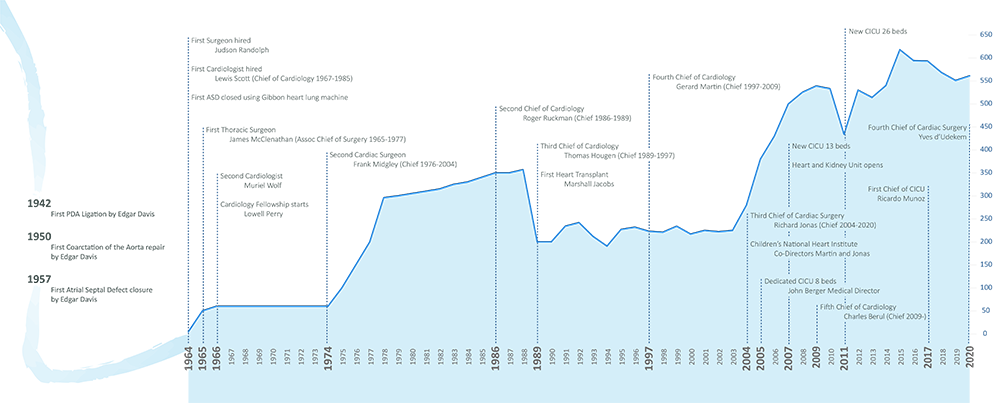
The article features a timeline mapping the growth of cardiac care for neonates, children and adults at Children’s National Hospital.
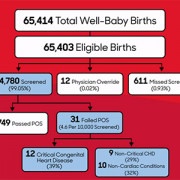
One of the nation’s longest-running newborn screening programs for critical congenital heart disease (CCHD) finds that screening continues to serve as a necessary tool to help identify every child with CCHD — even in states where the majority of babies are diagnosed before birth.
The screening program study findings were published in Pediatrics. The data is some of the first to provide long-term evidence for using pulse oximetry to screen newborns for critical congenital heart disease 24 hours after birth. This screening test was added to the Department of Health and Human Services Recommended Uniform Screening Panel in 2011 and is now required in all 50 states.
“This study reinforces why pulse oximetry screening for CCHD is an important tool in our arsenal to identify and treat critical congenital heart disease, and other conditions that affect the flow of oxygen throughout the body, as soon as possible,” says Bryanna Schwarz, M.D., a cardiology fellow at Children’s National Hospital and lead author. “We know that prompt, early detection and swift intervention is crucial to positive long-term outcomes for these kids.”
The team looked at the data and outcomes for all babies born throughout eight years at Holy Cross Hospital in suburban Maryland, one of the first community birthing hospitals in the country to routinely perform the screening. Over the eight-year period, 64,780 newborns were screened at the site. Of those:
The authors note that the 12 newborns with CCHD identified through pulse oximetry screening are noteworthy because they represent critical congenital heart disease cases that are not found before birth in the state of Maryland, where rates of prenatal diagnosis are relatively high. The finding indicates that screening after birth continues to play a critical role in ensuring every baby with critical congenital heart disease is identified and treated as quickly as possible.
“Holy Cross Health and Children’s National have had a decades-long relationship, as we mutually care for women and infants throughout the region. With Children’s National having the U.S. News & World Report #1 ranking Neonatology service in the nation and Holy Cross Hospital being among the top 10 hospitals for the number of babies delivered each year, we are honored to be leading together the great work that is being done to serve our health care community,” says Ann Burke, M.D., vice president of Medical Affairs at Holy Cross Hospital. “We are committed to continuing to do our part to care for women and infants, as well as contribute to the national landscape for neonatal care. We are delighted in the outcomes we have seen and look forward to continued advancement.”
In this study, infants who did not have critical congenital heart disease were considered “false positives” for CCHD. Still, every one of them was found to have another underlying condition, including non-critical congenital heart disease or non-cardiac conditions (such as sepsis and pneumonia) that would also require monitoring and treatment.
The researchers also ran a projection of recently recommended updates to the screening protocol, which include removing a second re-screen after a newborn fails the initial test, to look at whether removing the second rescreen to verify results would decrease accuracy. While the false positive rate did increase slightly from .03% to .04%, eliminating a second re-screen allowed the newborns who were identified to receive crucial care sooner without having to wait an additional hour for one more test to verify their condition.
“It’s time to stop asking if pulse oximetry is a necessary tool to detect critical heart disease in babies,” says Gerard Martin, M.D., M.A.C.C., senior author of the study and C.R. Beyda Professor of Cardiology at Children’s National Hospital. “Our focus now should be on making evidence-based refinements to the screening protocol based on collected data to ensure the process is simple, can be performed consistently and provides as accurate results as possible.”
