An analysis led by Sarah Schaffer DeRoo, M.D., found that knowledge, attitudes and beliefs about COVID-19 testing plays a key role in preventing COVID-19 transmission among Black parents.
Black-majority communities have been disproportionately affected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections, hospitalizations and deaths. As of September 2021, Black Americans had nearly three times the hospitalization rate and double the death rate due to coronavirus disease 2019 (COVID-19), as compared to White Americans.
An analysis led by Sarah Schaffer DeRoo, M.D., pediatrician at Children’s National Hospital, aimed to characterize knowledge, attitudes and beliefs about COVID-19 testing – a key tool for preventing COVID-19 transmission – among Black parents.
Semi-structured interviews were conducted and analyzed using a phenomenology approach with 26 self-identified Black parents after telemedicine visits with a children’s health center. Three central themes emerged regarding COVID-19 testing decision-making, including perceived COVID-19 disease susceptibility, barriers to testing and cues to action. Parents were keen to pursue testing to ensure the safety of themselves and their loved ones, especially if they perceived a high risk for COVID-19 infection, such as due to a known positive contact. However, barriers to testing for some parents included concerns about accuracy and safety of the tests, as well as possible stigma associated with a positive test result. Parents also shared their concern that a positive test result would not be met with an appropriate medical response due to structural racism in the health care system, making some reluctant to pursue testing.
“When considering the themes that emerged from these interviews, we were able to better understand Black Americans’ views of COVID-19 testing and motivations for accessing testing,” says Dr. Schaffer DeRoo. “Culturally responsive educational campaigns delivered by trusted community members should aim to improve understanding about disease transmission and testing.”
Framing testing as a means to ensure safety and acknowledging and addressing institutionalized racism that affects COVID-19 care may improve self-efficacy to obtain testing. “The health community should learn from these conversations with Black Americans so that disease prevention and mitigation strategies prioritize health equity,” says Dr. Schaffer DeRoo.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/11/boy-getting-covid-test.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-11-17 09:26:172021-11-24 09:15:39Sentiments about COVID-19 testing among Black parents in the United States
“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
Penicillin, a widely available and affordable antibiotic, may be one key to turning the tide on the deadly impacts of rheumatic heart disease (RHD) for children in developing nations. This according to the new findings of a large-scale, randomized controlled trial completed in Uganda and published in the New England Journal of Medicine.
The most devastating feature of RHD is severe heart valve damage that is caused by rheumatic fever — a condition that results from the body’s immune system trying to fight poorly treated, repeat infections from streptococcus bacteria, also known as strep throat. Though widely eradicated in nations such as the United States due to the swift detection and treatment of strep throat, rheumatic fever remains prevalent in developing countries including those in sub-Saharan Africa. Current estimates are that 40.5 million people worldwide live with rheumatic heart disease, and that it kills 306,000 people every year. Most of those affected are children, adolescents and young adults under age 25.
“We know from previous studies that though it is not always well-documented, sub-Saharan Africa continues to have some of the highest numbers of people with rheumatic heart disease and the highest numbers of people dying from it,” said Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and co-senior author of the study. “This study is the first large-scale clinical trial to show that early detection coupled with prophylactic treatment of penicillin is feasible and can prevent rheumatic heart disease from progressing and causing further damage to a child’s heart.”
The study was led by an international panel of pediatric cardiac experts from institutions including Children’s National, Cincinnati Children’s Medical Center, the Uganda Heart Institute and Murdoch Children’s Research Institute in Melbourne, Australia.
“Our study found a cheap and easily available penicillin can prevent progression of latent rheumatic heart disease into more severe, irreversible valve damage that is commonly seen in our hospitals with little or no access to valve surgery,” said co-lead author Emmy Okello, M.D., chief of Cardiology at the Uganda Heart Institute.
To Andrea Beaton, M.D., associate professor of Cardiology at Cincinnati Children’s and co-lead author, this is the first contemporary randomized controlled trial in rheumatic heart disease. “The results are incredibly important on their own, but also demonstrate that high-quality clinical trials are feasible to address this neglected cardiovascular disease,” she said.
Beaton et al. named the trial Gwoko Adunu pa Lutino (GOAL), which means “protect the heart of a child.” The study enrolled 818 Ugandan children and adolescents ages 5 to 17 years old who were diagnosed with latent rheumatic heart disease to see if an injection of penicillin was effective at preventing their heart condition from worsening.
“There are many challenges with recruitment and retention of trial participants in areas like our study region in Uganda,” said Dr. Sable. “But it is critical to work together and overcome barriers, because we must study these treatments in the people most affected by the condition to understand how they, and others like them, may benefit from the findings.”
Of the 799 participants who completed the trial, the group receiving a prophylactic injection of penicillin (399 volunteers) had three participants show evidence of worsened rheumatic heart disease on repeat echocardiogram after two years. In contrast, 33 of the 400 volunteers in the control group, who received no treatment, showed similar progression on echocardiogram results.
Professor Andrew Steer, who is theme director of Infection and Immunity at Murdoch Children’s Research Institute in Melbourne and who served as senior author of the study, said screening for latent rheumatic heart disease was critical to stop progression because heart valve damage was largely untreatable. “Most patients are diagnosed when the disease is advanced and complications have already developed. If patients can be identified early, there is an opportunity for intervention and improved health outcomes.”
The results were shared in a special presentation at the American Heart Association’s Scientific Sessions on the same day that the findings were published in the New England Journal of Medicine.
The trial was supported by the Thrasher Pediatric Research Fund, Gift of Life International, Children’s National Hospital Foundation: Zachary Blumenfeld Fund, Children’s National Hospital Race for Every Child: Team Jocelyn, the Elias/Ginsburg Family, Wiley-Rein LLP, Phillips Foundation, AT&T Foundation, Heart Healers International, the Karp Family Foundation, Huron Philanthropies and the Cincinnati Children’s Hospital Heart Institute Research Core.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/11/Craig-Echoing-in-village.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-11-15 09:48:352025-05-06 13:50:49Penicillin slows impacts of rheumatic heart disease in Ugandan children
When comparing the first and second wave of patients diagnosed with multi-system inflammatory syndrome in children (MIS-C), the second wave patients had more severe illness, according to a new prospective cohort study at Children’s National Hospital in Washington, D.C.
When comparing the first and second wave of patients diagnosed with multi-system inflammatory syndrome in children (MIS-C), the second wave patients had more severe illness, according to a new prospective cohort study of 106 patients at Children’s National Hospital in Washington, D.C. The results, published in The Pediatric Infectious Disease Journal, show that despite increased severity in the second wave cohort, both cohorts had similarities in cardiac outcomes and length of stay. Researchers are still working to better understand the exact immunologic mechanisms that trigger MIS-C and the specific factors accounting for its rare occurrence.
“We’ve now seen three distinct waves of MIS-C since the beginning of the pandemic, each wave following national spikes in cases,” said Roberta DeBiasi, M.D., chief of the Division of Pediatric Infectious Diseases at Children’s National and co-author of the study. “Kids in the second wave cohort had potentially experienced intermittent and/or repeated exposures to the virus circulating in their communities. In turn, this may have served as repeated triggers for their immune system which created the more severe inflammatory response.”
In this new study, key demographic features Children’s National researchers previously identified held true across both waves – including the fact that Black and Latino children are significantly more affected than white children. Of the 106 patients, 54% were Black and 39% were Hispanic. The authors also noted that 75% of the patients were otherwise healthy children with no underlying medical conditions.
“While we believe the most recent third wave associated with the delta variant surge is tapering off, the findings from the first two waves provide important baseline information and are highly relevant for clinicians across the country that are evaluating and treating kids with MIS-C,” said Dr. DeBiasi.
Children’s National has cared for more than 4,200 symptomatic patients with SAR-CoV-2 infection and more than 185 MIS-C patients since the pandemic began. The first wave of MIS-C patients were hospitalized between March 2020 and October 2020. Second wave patients were hospitalized between November 2020 and April 2021. Each wave came 4-6 weeks following periods of COVID-19 surges in the community.
In the study, researchers compared patient demographics, clinical features, laboratory results, radiographic images, therapies and outcomes. The second wave cohort had a higher proportion of children 15 years of age or older. Patients also presented more frequently with shortness of breath and required more advanced respiratory and inotropic support. Researchers also found that patients in the second wave were less likely to test positive for SARS-CoV-2 on a PCR test.
Dr. DeBiasi and her team hope to unlock even more insights as they now analyze data from the third wave associated with the delta variant, which currently appears to have affected less children than the previous two. Children’s National is also working in collaboration with the National Institute of Allergy and Infectious Diseases (NIAID) to study the long-term effects of MIS-C and COVID-19 on the pediatric population after recovery. This is among the largest and longest studies being conducted, and researchers are hopeful the findings will help improve treatment of COVID-19 and MIS-C in the pediatric population both nationally and around the world.
“Our timely established multidisciplinary MIS-C task force here at Children’s National allowed us to reduce the learning curve,” said Ashraf S. Harahsheh, M.D., F.A.A.P., F.A.C.C., director of Quality Outcomes in Cardiology and co-first author of the study. “Experience from other centers showed that immunotherapy was utilized more frequently in recent MIS-C cohorts leading to reduction in percentage of cardiac complications. On the other hand, and despite having increased illness severity in the second cohort, our approach with prompt immunotherapy helped stabilize the rate of cardiac complications.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/10/sick-child-in-palliative-care-hospital-bed.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-11-12 13:30:132021-11-12 13:30:13New study compares first and second wave of MIS-C
The grant enables a unique program – bringing together a team of school nurses in D.C. Public Schools, community health workers and mobile medical services.
The United Health Foundation, the philanthropic foundation of UnitedHealth Group, has awarded a three-year, $3.4 million grant to Children’s National Hospital to improve access to health care for school-aged children in Washington, D.C.’s most under-resourced communities. The support is part of the United Health Foundation’s ongoing commitment to build healthier communities and advance health equity.
The grant enables a unique program – bringing together a team of school nurses in D.C. Public Schools, community health workers and mobile medical services. Wards 7 and 8 face some of the largest health inequities in Washington, D.C., with high rates of child poverty, asthma, obesity and more.
“Children’s National has long worked to make sure every child in our region has access to high-quality care,” said Kurt Newman, M.D., president and CEO of Children’s National. “This new grant from the United Health Foundation will help us create another way to connect our pediatric experts with children and families who are not currently being served by health care providers. We are committed to helping children lead healthier lives which, in turn, makes them more likely to succeed in school and lead healthier lives as adults.”
School nurses employed by Children’s School Services will work with community health workers to connect children and families to mobile health services, Children’s National primary care locations and federally qualified health centers. Health records, immunization records and attendance data will be accessible through data sharing. As a result of the effort, children will receive well-child visits, including vaccinations and vision, hearing, behavioral health and developmental screenings. Additionally, via telemedicine, community health workers can link children to specialists to address behavioral health, asthma and other pressing health needs.
“Reaching school-aged children living in under-resourced communities to provide important routine health care can be challenging, especially amid a pandemic,” said Dr. Margaret-Mary Wilson, associate chief medical officer for UnitedHealth Group. “We are so pleased to be working with Children’s National on this innovative and comprehensive program to identify and close gaps in care — especially for those who have unaddressed needs.”
The effort aims to reduce school absenteeism among chronically absent students by connecting families to health supports and social services. It will also focus on increasing the number of children who are up to date on vaccinations, with a goal of providing 6,000 vaccinations over three years. Additionally, those who screen positive for mental or behavioral health issues will be referred to mental health specialists. The program is under the leadership of Hope Rhodes, M.D., M.P.H., medical director of THEARC, and one of the leaders of the Goldberg Center, and Danielle Dooley, M.D., M.Phil., medical director, Community Affairs and Population Health of the Child Health Advocacy Institute.
The grant will help address challenges identified in the Foundation’s recently released America’s Health Rankings 2021 Health of Women and Children Report. Some of the key findings of the report were:
Anxiety among children ages 3-17 rose 21% nationally between 2017-2018 and 2019-2020, from 7.5% to 9.1%.
Only 1 in 3 (34.3%) U.S. fourth grade public school students scored proficient or above on the national reading assessment. Later in life, there is a strong connection between education attainment and health, with those without a high school education facing the greatest social, economic and health challenges. National reading assessments are an important marker in educational development.
The prevalence of asthma among children in D.C. is 10%, higher than the national average of 7.5%.
On-time childhood vaccinations in D.C. are 75.3%, slightly lower than the national average of 75.8%.
The grant is one of the many ways the United Health Foundation continues to support efforts to build healthier communities and advance health equity. In September, UnitedHealth Group, including the United Health Foundation and UnitedHealthcare, announced a donation of $4.5 million to seven nonprofit organizations in Oklahoma to help increase health care, improve health outcomes and support communities across the state. And in July, the United Health Foundation established a $3.3 million grant partnership with the North Olympic Healthcare Network in Washington state to improve behavioral health for children and adults in the Port Angeles area. To learn more about UnitedHealth Group’s commitment to health equity, please visit the company’s sustainability website at sustainability.uhg.com.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/01/happy-children-running-with-kite.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-11-09 09:12:122023-07-03 10:49:13Children’s National receives United Health Foundation grant
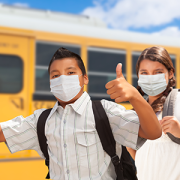
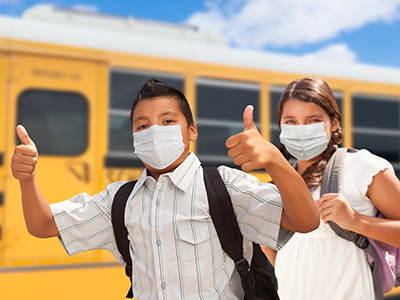
To keep in-person learning and protect students in schools, pediatricians and public health officials must advocate for evidence-based mitigation strategies that can reduce COVID-19 transmission — especially the Delta variant, which overwhelmed pediatric emergency rooms and hospitals, argued Yang et al. in a Perspective published in the journal Pediatrics.
To keep in-person learning and protect students in schools, pediatricians and public health officials must advocate for evidence-based mitigation strategies that can reduce COVID-19 transmission — especially the Delta variant, which overwhelmed pediatric emergency rooms and hospitals, argued Yang et al. in a Perspective published in the journal Pediatrics.
The authors propose that pediatricians and their associated institutions actively advocate for masking in schools and debunk myths and misinformation during well and sick visits. In addition, they encourage doctors to develop and disseminate behavioral strategies to support children’s compliance with masking based on individual abilities and needs. Finally, providers can partner with educators at the local, district, state and national levels to advocate for evidence-based masking policies.
“As pediatricians, it is our responsibility to advocate for universal masking to facilitate safe in-person schooling for all children,” said Sarah Schaffer DeRoo, M.D., pediatrician at Children’s National Hospital and co-author of the Perspective. “Children have readily adapted to masking during the pandemic and continuing this practice in schools is not a significant change from their recent experience.”
To date, nine states have enacted policies to prohibit school masking mandates, disregarding evidence that masking is a crucial COVID-19 preventive measure, Yang et al. wrote. The court overturned these mandates in four states out of the nine because they either exceeded the governor’s executive authority or did not comply with the law granting the executive order’s authority. In other instances, judges have only placed a temporary block.
“Despite politically charged rhetoric and headline-grabbing lawsuits, evidence shows that schools without mask mandates are more likely to have COVID-19 outbreaks,” said Y. Tony Yang, Sc.D., endowed professor of health policy and executive director of the Center for Health Policy and Media Engagement at the George Washington University, and lead author of the Perspective. “Pediatricians have generally commanded a heightened level of public trust, which suggests that pediatricians who make the case for policies that advance sound medical and public health science may have a greater chance than other advocates of generating the public and political will needed to make evidence-based policy ideas, such as school mask mandates, a reality.”
Some localities have found creative ways to circumvent state mask mandate bans by altering the school dress code to include face coverings and finding loopholes that do not apply to individual cities. Parents have also tried to challenge the policies in court, asserting that mask mandate bans violate federal anti-discrimination laws.
“Continued efforts are needed to ensure schools are able to promote reasonable, evidence-based strategies to promote the health of their students, teachers and communities, and we, as advocates for children, are obligated to emphatically support these efforts,” said Yang et al.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/10/kids-in-masks.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-10-20 07:05:402022-03-07 08:38:13Pediatricians and public health officials should unite against controversial school masking bans
Lee Savio Beers, M.D., F.A.A.P., medical director of Community Health and Advocacy at the Child Health Advocacy Institute (CHAI) at Children’s National Hospital and president of the American Academy of Pediatrics (AAP), delivered the President’s Address to AAP members around the world and held a keynote conversation with Olympic gold medalist Simone Biles about mental health during AAP’s National Conference and Exhibition.
After being introduced by her children, Charlotte and Jonah, Dr. Beers thanked AAP members around the world for their ability to adapt and provide quality care to patients throughout the COVID-19 pandemic. “The COVID-19 pandemic has changed our collective calculus of uncertainty, yet you continue to adapt and adjust to provide quality care in your clinics, emergency departments, ICU’s and exam rooms,” said Dr. Beers.
Dr. Beers continued by reflecting on accomplishments that AAP members and volunteers were able to achieve over the last year including the establishment of community immunization efforts, interim guidance provided on numerous pandemic-related issues and bi-weekly COVID-19 townhalls and educational sessions.
Shortly after her address, Dr. Beers sat down with Simone Biles to discuss the importance of advocating for mental health as an athlete.
During their conversation, Biles discussed the importance of making her mental health a priority by withdrawing from several events during the 2020 Tokyo Olympics. She reflected on the outpouring support she received and how it made her feel.
Biles also offered advice for youth dealing with mental health issues and stressed the importance of reaching out to parents or peers so they can get the help and support they need.
AAP’s National Conference and Exhibition, held from October 8 through October 11, serves as an opportunity to keep pediatric providers abreast of the latest best practices in pediatrics and strives to meet participants’ identified educational needs and support their life-long learning with a goal of improving care for children and families.
Speaker and presentation information can be found here.
Simone Biles discussed the importance of making mental health a priority with Dr. Lee Savio Beers.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/10/Simone-Biles-and-Dr.-Beers-tile.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-10-18 10:48:342025-12-08 16:45:45Dr. Lee Beers speaks with Olympic gold medalist Simone Biles about mental health
Until now, little was known about the incidence and virus-specific patient outcome of SARS-CoV-2 compared to common seasonal respiratory viruses in children — including respiratory syncytial virus (RSV), human parainfluenza (hPIV), human metapneumovirus (hMPV), respiratory adenovirus and human rhinovirus (hHRV) and respiratory enterovirus (rENT).
Common respiratory viral infections were associated with a higher proportion of inpatient admissions but were similar in intensive care unit (ICU) admissions and death rates in hospitalized pediatric patients when compared to SARS-CoV-2, according to Children’s National Hospital researchers that led a study published in Infection Control & Hospital Epidemiology.
Until now, little was known about the incidence and virus-specific patient outcome of SARS-CoV-2 compared to common seasonal respiratory viruses in children — including respiratory syncytial virus (RSV), human parainfluenza (hPIV), human metapneumovirus (hMPV), respiratory adenovirus and human rhinovirus (hHRV) and respiratory enterovirus (rENT).
The researchers also noted that there was an overall substantial decrease in seasonal respiratory viral infections, especially the severe forms that require hospitalization. They believe that this correlation might be associated with the adoption of COVID-19 public health mitigation efforts, which played a major role in the reduction of these viruses that often circulate in fall and winter. The retrospective cross-sectional cohort study analyzed over 55,000 patient admissions between Match 15 and December 31, 2020. The findings shed light on the incidences of eight common seasonal respiratory viral infections before and during the COVID-19 pandemic. It also compared patient outcomes associated with COVID-19 and these other viral infections among pediatric patients at Children’s National.
Xiaoyan Song, Ph.D., M.Sc., chief infection control officer at Children’s National, spoke to us about the study.
Q: Why is this important work?
A: This is the first study to date that has described and compared hospitalization rates, ICU admission rates and death associated with COVID-19, RSV, seasonal influenza, rhinovirus, enterovirus and other common respiratory viral infections in children in one study. Previously, studies have compared one or two viruses at a time. This study compared 8 viruses, including the most detected ones – COVID-19, RSV, seasonal flu, rhinovirus and enterovirus.
Q: How will this work benefit patients?
A: This study will inform patients, families and the public that preventative measures like masking, hand hygiene, avoiding crowds and avoiding people who are ill are good practices that work to protect children from getting COVID-19 but also from getting infected with RSV, influenza and other viruses. Any of these respiratory viruses could harm a patient to a point where the child may have to be hospitalized or receive ICU care.
You can read the full study published in Infection Control & Hospital Epidemiology.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/03/illustration-of-lungs-with-coronavirus-inside.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-10-14 16:53:162021-10-14 16:53:16Study compares outcomes of SARS-CoV-2 versus other respiratory viruses
Two Children’s National Hospital cardiac care leaders received prestigious recognition awards from the American Academy of Pediatrics (AAP) during that organization’s virtual National Conference and Exhibition in October 2021.
Gil Wernovsky, M.D., cardiac critical care specialist at Children’s National Hospital, received the 2021 Maria Serratto Master Educator Award from AAP Section on Pediatric Cardiology and Cardiac Surgery, celebrating his 30-plus-years as a clinician, educator, mentor and leader in the field.
Gerard Martin, M.D., FAAP, FACC, FAHA, C. Richard Beyda Professor of Cardiology, Children’s National Hospital, received the AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award, in recognition of his work to establish the use of pulse oximetry to screen newborn infants for critical congenital heart disease in the first 24 hours of life.
Dr. Wernovsky: 2021 Maria Serratto Master Educator Award, AAP Section on Pediatric Cardiology and Cardiac Surgery
Gil Wernovsky, M.D., received the 2021 Maria Serratto Master Educator Award from AAP Section on Pediatric Cardiology and Cardiac Surgery.
The Master Educator Award is presented each year to a pediatric cardiologist or cardiothoracic surgeon who exemplifies excellence as an educator, mentor and/or leader in the field.
A practicing cardiac critical care specialist with more than 30 years’ experience in pediatric cardiology, Dr. Wernovsky trained and mentored more than 300 fellows in pediatric cardiology, cardiac surgery, neonatology, critical care medicine and cardiac anesthesia, in addition to countless residents and fellows. He also organizes national and international symposia to share expertise around the world. During the COVID-19 public health emergency, for example, he co-founded the Congenital Heart Academy (CHA). The CHA provides content from an international faculty of cardiac care to more than 26,000 practitioners in 112 countries and includes a thriving YouTube channel.
Dr. Wernovsky is also a founding member of several international societies focused on bringing together clinicians, researchers and students across sub-specialties of pediatric cardiology and cardiac surgery for knowledge exchange and best practice sharing. These include: the Pediatric Cardiac Intensive Care Society, World Society for Pediatric and Congenital Heart Surgery, the International Society of Pediatric Mechanical Circulatory Support and the Cardiac Neurodevelopmental Outcome Collaborative.
Dr. Wernovsky received the award on October 10 at the virtual Scientific Sessions of the 2021 American Academy of Pediatrics National Conference and Exhibition.
Dr. Martin: AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award
Gerard Martin, M.D., FAAP, FACC, FAHA, C. Richard Beyda Professor of Cardiology, Children’s National Hospital, received the AAP Section on Advances in Therapeutics and Technology (SOATT) Achievement Award.
The Section on Advances in Therapeutics and Technology (SOATT) educates physicians, stimulates research and development and consults on therapeutics and technology-related matters for the AAP. The Achievement Award recognizes someone who has shown leadership in applying innovative approaches to solve pressing problems.
Dr. Martin is the C. Richard Beyda Professor of Cardiology and has cared for children at Children’s National for more than 30 years. As an advocate for congenital heart disease efforts nationally and internationally, he played an integral role in the development of an innovative use of existing hospital technology—the pulse oximeter—to detect critical congenital heart disease in newborn babies.
Today, Dr. Martin and colleagues across the United States and around the world have worked to make this screening method a standard of care for newborns everywhere. It is a part of the Health Resources and Services Administration (HRSA) Recommended Uniform Screening Panel and has become law in every state. They continue to conduct research to refine the recommendations and hone-in on the most effective ways to harness these tools.
Dr. Martin was selected for this award in 2020. He accepted it and offered remarks during the 2021 virtual AAP National Conference and Exhibition on Monday, October 11, 2021.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/10/Wernovsky-and-Martin.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-10-11 12:20:092025-02-18 12:11:10Cardiac care leaders recognized for mentorship and innovation at AAP
Being designated with this recognition recognizes that Children’s National has deployed technologies and strategies to help analyze its data and is starting to achieve meaningful clinical and efficiency outcomes. It’s also experimenting with more advanced technologies, like telehealth, that expand access to care.
Children’s National Hospital received the 2021 Digital Health Most Wired recognition by The College of Healthcare Information Management Executives (CHIME) as a certified ambulatory level nine and acute level eight. The CHIME Digital Health Most Wired program conducts an annual survey to assess how effectively health care organizations apply core and advanced technologies into their clinical and business programs to improve health and care in their communities.
“Children’s National is honored to again receive the Most Wired distinction for our inpatient and ambulatory venues,” said Matt MacVey, chief information officer at Children’s National. “We are particularly excited to see our ongoing consumer digital experience investments propel us to a level 9 in ambulatory.”
Being designated with this recognition recognizes that Children’s National has deployed technologies and strategies to help analyze its data and is starting to achieve meaningful clinical and efficiency outcomes. It’s also experimenting with more advanced technologies, like telehealth, that expand access to care.
“Digital transformation in health care has accelerated to an unprecedented level since 2020, and the next few years will bring a wave of innovation that empowers health care consumers and will astound the industry,” said CHIME President and CEO Russell P. Branzell. “The Digital Health Most Wired program recognizes the outstanding digital leaders who have paved the way for this imminent revolution in health care. Their trailblazing commitment to rapid transformation has set an example for the entire industry in how to pursue a leadership vision with determination, brilliant planning and courage to overcome all challenges.”
A total of 36,674 organizations were represented in the 2021 Digital Health Most Wired program, which includes four separate surveys: acute, ambulatory, long-term care and international acute. The surveys assessed the adoption, integration and impact of technologies in healthcare organizations at all stages of development, from early development to industry leading.
This is the fourth year that CHIME has conducted the survey and overseen the program. In each successive year, CHIME has expanded the survey to capture more types of organizations that serve patients across the continuum of care. CHIME also continues to promote the program internationally to provide a global overview of digital health advancements.
“We are committed to investing in technology that helps us bring safe, high quality care to children,” said Jessica Herstek, M.D., chief medical informatics officer at Children’s National. “We are honored by the ‘Most Wired’ distinction and remain focused on our vision to help children grow up stronger.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/11/telemedicine-1.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-10-08 10:24:102024-09-06 15:19:35Children’s National Hospital technology recognized
When asked a simple “yes” or “no” question about food allergy-related bullying, 17% of kids said they’d been bullied, teased or harassed about their food allergy. But when asked to reply to a multi-item list of victimization behaviors, that number jumped to 31%.
Living with a food allergy can greatly impact a child’s everyday life – from limiting participation in social activities to being treated differently by peers. While previous research indicates many kids experience food allergy-related bullying, a new study in the Journal of Pediatric Psychology found that offering kids with food allergies a multi-question assessment gives a more accurate picture of the size and scope of the problem.
When asked a simple “yes” or “no” question about food allergy-related bullying, 17% of kids said they’d been bullied, teased or harassed about their food allergy. But when asked to reply to a multi-item list of victimization behaviors, that number jumped to 31%. Furthermore, Children’s National Hospital researchers found that only 12% of parents reported being aware of it.
The reported bullying ranged from verbal teasing or criticism to more overt acts such as an allergen being waved in their face or intentionally put in their food. Researchers say identifying accurate assessment methods for this problem are critical so children can get the help they need.
“Food allergy-related bullying can have a negative impact on a child’s quality of life. By using a more comprehensive assessment, we found that children with food allergies were bullied more than originally reported and parents may be in the dark about it,” says Linda Herbert, Ph.D., director of the Psychosocial Clinical and Research Program in the Division of Allergy and Immunology at Children’s National and one of the study’s researcher.
“The results of this study demonstrate a need for greater food allergy education and awareness of food allergy-related bullying among communities and schools where food allergy-related bullying is most likely to occur,” Herbert adds.
The study looked at food allergy-related bullying among a diverse patient population and evaluated parent-child disagreement and bullying assessment methods. It included 121 children and 121 primary caregivers who completed questionnaires. The children ranged in age from 9 to 15-years-old and were diagnosed by an allergist with at least one of the top eight IgE-mediated food allergies – peanut, tree nut, cow’s milk, egg, wheat, soy, shellfish and fish.
Of the 41 youth who reported food allergy-related bullying:
51% reported experiencing overt physical acts such as an allergen being waved in their face, thrown at them or intentionally put in their food.
66% reported bullying experiences that are categorized as non-physical overt victimization acts including verbal teasing, remarks or criticisms about their allergy and verbal threats or intimidation.
Eight reported relational bullying, such as rumors being spread, people speaking behind their back and being intentionally ignored or excluded due to their food allergy.
The researchers also note that food allergy bullying perpetrators included, but were not limited to, classmates and other students, and bullying most commonly occurred at school.
The authors found that only 12% of parents reported that their child had been bullied because of their food allergy and of those, 93% said their child had reported the bullying to them. Some parents reported they had been made fun of or teased themselves because of concerns about their child’s food allergy.
“It’s important to find ways for children to open up about food allergy-related bullying,” Herbert says. “Asking additional specific questions about peer experiences during clinic appointments will hopefully get children and caregivers the help and support they need.”
Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, under Award Number K23AI130184 and National Institute on Minority Health and Health Disparities, part of the National Institutes of Health, under Award Number P20MD000198. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Children’s National Hospital received a combined $2.13 million award from the National Institutes of Health’s (NIH) National Heart, Lung and Blood Institute to better understand the mechanisms of severe viral respiratory infections in patients with Down syndrome and to develop new diagnostic tools and innovative precision medicine approaches for this vulnerable population.
“We have a unique opportunity to discover novel targets that can treat severe viral respiratory infections, including SARS-CoV-2,” said Gustavo Nino, M.D., M.S.H.S., D’A.B.S.M., principal investigator in the Center for Genetic Medicine at Children’s National. “Part of the award will help us accelerate the development of these novel approaches to prevent severe respiratory infections caused by SARS-CoV-2 and other viruses like respiratory syncytial virus infection (RSV) in children and adults with Down syndrome.”
Lower respiratory tract infections are a leading cause of hospitalization and death in children with Down syndrome. Those children have a nine times higher risk for hospitalization and mortality due to respiratory viruses that cause lower respiratory tract infections.
Chromosome 21, which is an extra chromosome copy found in patients with Down syndrome, encodes four of the six known interferon receptors, leading to hyperactivation of interferon response in Down syndrome. With the central role of interferons focused on antiviral defense, it remains puzzling how interferon hyperactivation contributes to severe viral lower respiratory tract infections in children with Down syndrome. This is an area that the researchers will explore to better manage and treat viral lower respiratory tract infections in these patients, with the support of NIH’s INCLUDE initiative. INCLUDE provides institutions with grants to help clinical research and therapeutics to understand and diminish risk factors that influence the overall health, longevity, and quality of life for people with Down syndrome related to respiratory viruses.
“While many of the other studies focus on intellectual and other disabilities, we are exploring a novel viral respiratory infectious disease mechanism and are doing so by working directly with patients and patient-derived samples,” said Jyoti Jaiswal, M.Sc., Ph.D., senior investigator in the Center for Genetic Medicine Research at Children’s National.
Children with Down syndrome have historically been excluded in research related to airway antiviral immunity, which is a focus of this human-based transformative study to improve the health and survival of patients with Down syndrome. There is a critical need for studies that define targetable molecular and cellular mechanisms to address dysregulated antiviral responses in this patient population.
“The clinical expertise at Children’s National in studying Down syndrome and the work of our team in caring for these patients with respiratory and sleep disorders positions us well to pursue this work,” said Jaiswal. “This is further supplemented by our initial studies that have identified a novel mechanism of impaired airway antiviral responses in these patients.”
Congresswoman Eleanor Holmes Norton (D-DC) also celebrated Children’s National and its NIH research funding benefitting people with Down syndrome.
“I am pleased to congratulate Dr. Nino and staff on being the recipients of the National Heart, Lung, & Blood Institute grant. You were chosen from a competitive group of applicants and should be proud of this notable achievement,” said Norton in a letter. “By receiving this grant, you have demonstrated outstanding promise in your field. It is my hope that this grant will enable you to better the local and global community.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/09/RSV-infected-cells.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-09-27 11:49:532021-11-12 09:50:24$2.13M grant accelerates treatments for kids with Down syndrome experiencing respiratory viruses
Racism and childhood obesity are both pervasive factors adversely affecting the health and wellbeing of children and adolescents in the United States, writes Eleanor Mackey, Ph.D., psychologist at Children’s National Hospital, and others in a recent article published by Childhood Obesity.
“The association between racism and obesity has been touched upon in the literature, yet most work has focused on a few dimensions of intersectionality of these two domains at one time,” the Mackey et al. write. “The renewed focus on structural racism as the primary contributor to distress of Black individuals in the United States has highlighted the urgency of identifying the contributions of racism to the childhood obesity epidemic.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/09/sad-boy-with-soccer-ball.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-09-15 09:43:072021-09-15 09:44:44Structural racism and childhood obesity epidemic in Black youth
One of the nation’s longest-running newborn screening programs for critical congenital heart disease (CCHD) finds that screening continues to serve as a necessary tool to help identify every child with CCHD — even in states where the majority of babies are diagnosed before birth.
The screening program study findings were published in Pediatrics. The data is some of the first to provide long-term evidence for using pulse oximetry to screen newborns for critical congenital heart disease 24 hours after birth. This screening test was added to the Department of Health and Human Services Recommended Uniform Screening Panel in 2011 and is now required in all 50 states.
“This study reinforces why pulse oximetry screening for CCHD is an important tool in our arsenal to identify and treat critical congenital heart disease, and other conditions that affect the flow of oxygen throughout the body, as soon as possible,” says Bryanna Schwarz, M.D., a cardiology fellow at Children’s National Hospital and lead author. “We know that prompt, early detection and swift intervention is crucial to positive long-term outcomes for these kids.”
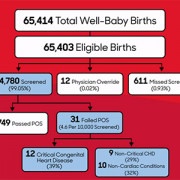
The team looked at the data and outcomes for all babies born throughout eight years at Holy Cross Hospital in suburban Maryland, one of the first community birthing hospitals in the country to routinely perform the screening. Over the eight-year period, 64,780 newborns were screened at the site. Of those:
Thirty-one failed the screening, and every baby who failed was found to have congenital heart disease or another important medical condition.
Twelve of the failures (38.7%) were babies with critical congenital heart disease who were not previously identified by prenatal detection.
Nine others (29%) had a non-critical congenital heart condition.
Ten additional babies (32%) had a non-cardiac condition.
The authors note that the 12 newborns with CCHD identified through pulse oximetry screening are noteworthy because they represent critical congenital heart disease cases that are not found before birth in the state of Maryland, where rates of prenatal diagnosis are relatively high. The finding indicates that screening after birth continues to play a critical role in ensuring every baby with critical congenital heart disease is identified and treated as quickly as possible.
“Holy Cross Health and Children’s National have had a decades-long relationship, as we mutually care for women and infants throughout the region. With Children’s National having the U.S. News & World Report #1 ranking Neonatology service in the nation and Holy Cross Hospital being among the top 10 hospitals for the number of babies delivered each year, we are honored to be leading together the great work that is being done to serve our health care community,” says Ann Burke, M.D., vice president of Medical Affairs at Holy Cross Hospital. “We are committed to continuing to do our part to care for women and infants, as well as contribute to the national landscape for neonatal care. We are delighted in the outcomes we have seen and look forward to continued advancement.”
In this study, infants who did not have critical congenital heart disease were considered “false positives” for CCHD. Still, every one of them was found to have another underlying condition, including non-critical congenital heart disease or non-cardiac conditions (such as sepsis and pneumonia) that would also require monitoring and treatment.
The researchers also ran a projection of recently recommended updates to the screening protocol, which include removing a second re-screen after a newborn fails the initial test, to look at whether removing the second rescreen to verify results would decrease accuracy. While the false positive rate did increase slightly from .03% to .04%, eliminating a second re-screen allowed the newborns who were identified to receive crucial care sooner without having to wait an additional hour for one more test to verify their condition.
“It’s time to stop asking if pulse oximetry is a necessary tool to detect critical heart disease in babies,” says Gerard Martin, M.D., M.A.C.C., senior author of the study and C.R. Beyda Professor of Cardiology at Children’s National Hospital. “Our focus now should be on making evidence-based refinements to the screening protocol based on collected data to ensure the process is simple, can be performed consistently and provides as accurate results as possible.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/08/flow-chart-of-pulse-ox-study-small.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-08-24 15:12:442021-08-27 10:30:14Newborn screening for critical congenital heart disease serves as vital safety net
Despite low numbers of documented acute rheumatic fever cases in sub-Saharan Africa, the region continues to show some of the highest numbers of people with, and dying from, rheumatic heart disease, the serious heart damage caused by repeat instances of rheumatic fever.
Despite low numbers of documented acute rheumatic fever cases in sub-Saharan Africa, the region continues to show some of the highest numbers of people with, and dying from, rheumatic heart disease, the serious heart damage caused by repeat instances of rheumatic fever. A population-based study in the Lancet Global Health collected evidence of acute rheumatic fever in two areas of Uganda, providing the first quantifiable evidence in decades that the disease continues to take a deadly toll on the region’s people.
“These findings matter. Access to life-saving heart surgery is only available to a very small fraction of the hundreds of thousands of patients in Africa who have irreversible heart damage from rheumatic heart disease,” says Craig Sable, M.D., associate chief of Cardiology at Children’s National Hospital and one of the senior authors of the study. “It’s time to focus upstream on capturing these conditions sooner, even in low-resource settings, so we can implement life-sustaining and cost-saving preventive treatments that can prevent further heart damage.”
The authors, who hail from Uganda and several institutions around the United States, including Children’s National and Cincinnati Children’s Hospital Medical Center, note this is the first study to use an active case-finding strategy for diagnosing acute rheumatic fever. They also note that raising awareness in the community and among its healthcare workers while also finding new ways to overcome some of the diagnostic challenges in these low-resource settings greatly improved diagnosis and treatment of the condition.
The study also described clinical characteristics of children ages 5 to 14 presenting with both definitive and possible acute rheumatic fever, providing further clinical data points to help healthcare workers in these communities differentiate between this common infection and some of the other frequently diagnosed conditions in the region.
“With this study, we can now confidently dismiss the myth that acute rheumatic fever is rare in Africa,” the authors write. “It exists at elevated rates in low-resource settings such as Uganda, even though routine diagnosis remains uncommon. While these incidence data have likely underestimated the cases of acute rheumatic fever in two districts in Uganda, they show that opportunity exists to improve community sensitization and healthcare worker training to increase awareness of acute rheumatic fever. Ultimately this leads to diagnosing more children with the condition before they develop rheumatic heart disease, so that they can be offered secondary prophylaxis with penicillin.”
Children with suspected acute rheumatic fever participated in this population-based study. Data was collected over 12 months in Lira district (January 2018 to December 2018) and over nine months (June 2019 to February 2020) in Mbarara district.
Follow-up of children diagnosed in this study will provide more data on the outcomes of acute rheumatic fever, including a better understanding of the risk for a child to develop rheumatic heart disease.
This work was funded by the American Heart Association Children’s Strategically Focused Research Network Grant #17SFRN33670607 and by DEL‐15‐011 to THRiVE‐2 and General Electric.
Learn more about the challenges of rheumatic heart disease in sub-Saharan Africa and other developing parts of the world through the Rheumatic Heart Disease microdocumentary series:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/08/Ugandan-boy-in-hospital-bed.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-08-20 12:04:522025-05-06 13:48:55Acute rheumatic fever often goes undiagnosed in sub-Saharan Africa
A single center study of patients with multisystem inflammatory disease in children (MIS-C) found that half of children diagnosed with MIS-C had a heart complication as part of the disease. The study collected and analyzed data from 39 cases of MIS-C at Children’s National Hospital in 2020. MIS-C is a pediatric disease that has been linked to SARS-CoV-2, the virus that causes COVID-19.
The study’s findings appear in the journal Cardiology of the Young. The authors aimed to describe the type and frequency of cardiac complications in children with MIS-C while also outlining the disease’s short-term progression. They also hoped to better understand the demographics, clinical and laboratory findings, as well as the therapeutic successes for children with cardiac complications from MIS-C.
“While half of all children at our hospital diagnosed with MIS-C did experience a cardiac complication, it’s important to note that almost all of them (84%) also fully recovered from that cardiac complication within 50 days of diagnosis,” says Ashraf Harahsheh, M.D., director of Quality Outcomes in Cardiology at Children’s National Hospital, who led the study. “We were also able to identify a few common factors among those with cardiac complications that, with further research, may help us identify earlier the children with MIS-C who are at greater risk for heart problems.”
The study found that children with cardiac complications had higher levels of natriuretic peptides, which appear in greater numbers when the heart isn’t pumping enough blood to the rest of the body. Additionally, children who developed heart complications also had higher initial white blood cell counts. MIS-C cardiac complications ranged from mild systolic dysfunction to coronary artery abnormalities and/or artery dilation.
This was a retrospective, observational study of 39 patients admitted to Children’s National Hospital from March 2020 to September 2020 who met the Centers for Disease Control and Prevention MIS-C case definition. Patient demographics, clinical features, laboratory values, diagnostic investigations, including echocardiograms, and therapies were extracted from the electronic medical records.
“This syndrome has some similarities to Kawasaki disease, another inflammatory syndrome that is known to cause cardiac complications,” says Dr. Harahsheh. “Thankfully what we’ve learned from studying and treating Kawasaki disease in children has helped us collaborate with partners around the world to find treatments for MIS-C that seem to minimize the impact of these complications, at least in the short term.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/coronavirus.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-08-18 10:33:522021-08-18 10:33:52One-half of MIS-C patients at a single center experienced heart complications
Up to 2,000 children and young adults will be enrolled in a study from Children’s National Hospital in collaboration with the National Institute of Allergy and Infectious Diseases (NIAID) that will examine the long-term effects of COVID-19 and multisystem inflammatory syndrome in children (MIS-C) after these patients have recovered from a COVID-19 infection.
This $40 million multi-year study will provide important information about quality of life and social impact, in addition to a better understanding of the long-term physical impact of the virus, including effects on the heart and lung. The researchers hope to detail the role of genetics and the immune response to COVID-19, so-called “long COVID” and MIS-C, including the duration of immune responses from SARS-CoV-2, the virus that causes COVID-19. It is fully funded by a subcontract with the NIH-funded Frederick National Laboratory for Cancer Research operated by Leidos Biomedical Research, Inc.
“We don’t know the unique long-term impact of COVID-19 or MIS-C on children so this study will provide us with a critical missing piece of the puzzle,” says Roberta DeBiasi, M.D., M.S., chief of the Division of Pediatric Infectious Diseases at Children’s National and lead researcher for this study. “I am hopeful that the insights from this enormous effort will help us improve treatment of both COVID-19 and MIS-C in the pediatric population both nationally and around the world.”
Over the past year, more than 3.6 million children have tested positive for SARS-CoV-2 and over 2,800 cases of MIS-C have been reported throughout the U.S. While the vast majority of children with primary SARS-CoV-2 infection may have mild or no symptoms, some develop severe illness and may require hospitalization, including life support measures. In rare cases, some children who have previously been infected or exposed to someone with SARS-CoV-2 have developed MIS-C, a serious condition that may be associated with the virus. MIS-C symptoms can include fever, abdominal pain, bloodshot eyes, trouble breathing, rash, vomiting, diarrhea and neck pain, and can progress to shock with low blood pressure and insufficient cardiac function. Long COVID is a wide range of symptoms that can last or appear weeks or even months after being infected with the virus that causes COVID-19.
The study is designed to enroll at least 1,000 children and young adults under 21 years of age who have a confirmed history of symptomatic or asymptomatic SARS-CoV-2 infection or MIS-C. Participants who enroll within 12 weeks of an acute infection will attend study visits every three months for the first six months and then every six months for three years. Participants who enroll more than 12 weeks after acute infection will attend study visits every six months for three years. The study will also enroll up to 1,000 household contacts to serve as a control group, and up to 2,000 parents or guardians (one parent per participant) will complete targeted questionnaires.
“The large number of patients who will be enrolled in this study should provide us with a truly comprehensive understanding of how the virus may continue to impact some patients long after the infection has subsided,” says Dr. DeBiasi.
The study primarily aims to determine incidence and prevalence of, and risk factors for, certain long-term medical conditions among children who have MIS-C or a previous SARS-CoV-2 infection. The study will also evaluate the health-related quality of life and social impacts for participants and establish a biorepository that can be used to study the roles of host genetics, immune response and other possible factors influencing long-term outcomes.
Children’s National was one of the first U.S. institutions to report that children can become very ill from SARS-CoV-2 infection, despite early reports that children were not seriously impacted. In studies published in the Journal of Pediatrics in May of 2020 and June of 2021, Children’s National researchers found that about 25% of symptomatic COVID patients who sought care at our institution required hospitalization. Of those hospitalized, about 25% required life support measures, and the remaining 75% required standard hospitalization. Of patients with MIS-C, 52% were critically ill.
Study sites include Children’s National Hospital inpatient and outpatient clinics in the Washington, D.C. area, and the NIH Clinical Center in Bethesda, Maryland.
Those interested in participating should submit this form. You will then be contacted by a study team member to review the study details and determine whether you are eligible to participate.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/coronavirus.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-07-20 10:21:302021-07-22 16:24:50Children’s National Hospital and NIAID launch large study on long-term impacts of COVID-19 and MIS-C on kids
Children’s National Hospital has entered into a licensing agreement with MGeneRx Inc. for its patented pediatric medical device technology using objective digital biometric analysis software for the early and non-invasive screening of dysmorphic genetic diseases such as Noonan syndrome.
Children’s National Hospital has entered into a licensing agreement with life sciences technology company MGeneRx Inc. for its patented pediatric medical device technology using objective digital biometric analysis software for the early and non-invasive screening of dysmorphic genetic diseases. The technology, developed by a multidisciplinary Children’s National team led by Marius George Linguraru, D.Phil, M.A., M.Sc., of the Sheikh Zayed Institute for Pediatric Surgical Innovation and Marshall Summar, M.D., director of the Children’s National Rare Disease Institute (CNRDI), can provide a more advanced diagnostic tool for regions of the world with limited access to geneticists or genetic testing.
The application utilizes artificial intelligence (AI) and machine learning to analyze biometric data and identify facial markers that are indicative of genetic disorders. Physicians can capture biometric data points of a child’s face in real time within the platform, where it scans facial biometric features to determine the potential presence of a genetic disease, which can often be life-threatening without early intervention. Research studies conducted in conjunction with the National Human Genome Research Institute at the National Institutes of Health further enhanced the development of the application in recent years, showing the potential to detect, with a 90 percent accuracy, early diagnosis of 128 genetic diseases across pediatric subjects in 28 countries. These diseases include DiGeorge syndrome (22q11.2 deletion syndrome), Down syndrome, Noonan syndrome and Williams-Beuren syndrome.
“We are delighted to enter into this licensing agreement through Innovation Ventures, the commercialization arm of Children’s National Hospital, which seeks to move inventions and discoveries from Children’s National to the marketplace to benefit the health and well-being of children. Our mission is to add the ‘D’ in development to the ‘R’ in research to accelerate the commercialization of our intellectual property,” says Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National and managing director of Innovation Ventures. “It is through partnerships with startups and the industry that we can achieve this goal and thus we highly value this new partnership with MGeneRx Inc. The acceleration and commercialization of this objective digital biometric analysis technology will not only help diagnose rare genetic disorders – it will also allow for earlier interventions that improve the quality of life for the children living with these conditions.”
Eskandanian adds that the social impact of this technology is especially profound in lower income nations around the world, where there is a high prevalence of rare genetic conditions but a severe lack in the specialty care required to diagnose and treat them. Additional data collected through the expanded use of the technology will help to further develop the application and expand its capabilities to identify and diagnose additional rare genetic conditions.
The licensing agreement was arranged by the Children’s National Office of Innovation Ventures, which is focused on the commercialization of impactful new pediatric medical device technologies and therapies to advance children’s health care. Created to catalyze the ongoing translational research of the Children’s National Research Institute (CNRI) as well as inventions by hospital’s clinicians, Innovation Ventures focuses on four core pillars to advance pediatric medical technologies including a Biodesign program, partnerships and alliances to augment internal capacity, seed funding to de-risk technologies and validate market and clinical relevance, and back-office operations to manage intellectual property and licensing activities. Since 2017, Children’s National intellectual property has served as the basis for over 15 licensing or option agreements with commercial partners.
Providing access to an array of experts and resources for pediatric innovators is one of the aims of the Children’s National Research & Innovation Campus, a first-of-its-kind focused on pediatric health care innovation, with the first phase currently open on the former Walter Reed Army Medical Center campus in Washington, D.C. With its proximity to federal research institutions and agencies, universities, academic research centers, as well as on-site incubator Johnson and Johnson Innovation – JLABS, the campus provides a rich ecosystem of public and private partners, which will help bolster pediatric innovation and commercialization.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/12/Noonan-facial-recognition.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-07-14 15:48:322025-03-10 13:27:11Commercialization of novel facial analysis technology can improve diagnosis of rare disorders in pediatric patients
Young people with autism are distinctly aware of their own challenges in areas such as flexibility, working memory and inhibition—abilities known collectively as “executive function,” according to the first study to measure and compare self-reports in these areas to more traditional reporting from parents.
Young people with autism are distinctly aware of their own challenges in areas such as flexibility, working memory and inhibition — abilities known collectively as “executive function,” according to the first study to measure and compare self-reports in these areas to more traditional reporting from parents. The study appears in the Journal Autism.
While autism research has started to focus on incorporating the experiences of autistic people themselves through self-reporting and greater inclusion in the design and execution of related research, this is the first time that a study has definitively captured self-reports of executive functions directly from young people with autism.
The study, which included 197 autistic youth, found that while both youth and their parents are in basic agreement about which areas of executive functioning that individual youth struggle with most, parents tended to report higher levels of impairment than the youth reported themselves. Executive function is related to a person’s ability to complete tasks such as adjusting to change, making a plan, getting organized and following through, as well as basic daily tasks like getting up and getting dressed or making small talk.
“While parents are reporting on outwardly observed behaviors in the context of home/community, for example, youth are reporting on their inner experiences across many contexts,” said Lauren Kenworthy, Ph.D., first author on the study and director of the Center for Autism Spectrum Disorders at Children’s National Hospital. “Our findings support the idea that autistic youth may be drawing their conclusions from different environmental data and cognitive frameworks than their parents, which adds a new dimension to our understanding of executive function in people with autism.”
The data are especially compelling because youth and parent reports of executive function were gathered on parallel measures with consistent items and factor structure, allowing for a true one-to-one comparison between youth and parent reporting.
“These kids are very aware of the areas where they struggle,” Dr. Kenworthy said. “And the findings from this study further elevate the importance of making sure that assessments of executive function take into account the perspective of the youth themselves, which can provide powerful insights into the interventions that they may benefit from the most.”
The study also compared reports from autistic youth to reports from both neurotypical youth and those with attention deficit hyperactivity disorder (ADHD), another condition where executive functioning skills can be challenged. There were distinct differences between all three groups—and the challenges profiled by youth with autism and those with ADHD were distinct from each other. For example, autistic youth reported greater challenges with flexibility, emotional control and self-monitoring than those with ADHD, who reported greater struggles with working memory.
The authors noted that future studies should include more performance-based measures, as well as larger numbers of females and people with intellectual disabilities to better understand how self-reporting can play a role in understanding and helping these specific groups. Additionally, developing new measures that capture the inner experience of autism by engaging autistic people in their creation could provide deeper insight into how young people with autism experience the world and how interventions designed to assist them are working (or not).
“These data provide clear evidence of the executive functioning challenges actually experienced by autistic youth as well as the primary role inflexibility plays in the lives of these young people,” the authors concluded. “This additional perspective and context for the experiences of these executive functioning challenges are of high clinical value and complement more frequently gathered assessments in ways never captured before.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/07/boy-with-autism-blowing-bubbles.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-07-09 14:29:072021-07-09 14:30:50Autistic youth self-reporting critical to understanding of executive function challenges
Sub-Saharan Africa has only 0.19 pediatric cardiac surgeons per million children — nowhere near enough surgeons to care for all the pediatric congenital heart disease and acquired heart disease present in the people who live there.
A literature review in the journal Current Opinion in Cardiology draws further attention to the pressing needs for better pediatric cardiac care in regions of the world where the population continues to grow, but the development of specialty care for children continues to lag. The article focuses specifically on sub-Saharan Africa.
“If 40% of live births occur in Africa by 2050 as the projections suggest, congenital heart disease may well become the most important contributor to infant mortality rate in sub-Saharan Africa in the next three decades,” stated the authors, including Annette Ansong, M.D., who recently joined Children’s National Hospital as medical director of outpatient cardiology.
As highlighted previously by other authors within the Global Health Initiative at Children’s National and through the work of the American Heart Association, the region’s needs are already significant in tackling the impacts of existing congenital heart disease and rheumatic heart disease. Rheumatic heart disease is a devastating long-term outcome of rheumatic fever caused by untreated streptococcus infections.
“If 40% of live births occur in Africa by 2050 as the projections suggest, congenital heart disease may well become the most important contributor to infant mortality rate in sub-Saharan Africa in the next three decades,” stated the authors, including Annette Ansong, M.D., who recently joined Children’s National Hospital as medical director of outpatient cardiology.
Dr. Ansong and colleagues reiterate the point that today, “whereas one cardiac center caters to approximately 120,000 people in North America, 33 million people in sub-Saharan Africa must depend on one center for care.” They also note that this region of Africa has only 0.19 pediatric cardiac surgeons per million children compared with more than 58 times as many in North America.
Changing the trajectory of pediatric cardiac care in sub-Saharan Africa will take motivation on several fronts, the authors write. Dedication to early detection and intervention (medical or surgical), an emphasis on building an in-country pipeline of human resources and skills’ sets are needed to tackle the increasing numbers of children requiring this specialty care. Political will and better financial resources can also support the training and development of centers that specialize in these capabilities.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/06/Crowded-makeshift-buildings-of-a-shantytown.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-06-30 16:33:222021-08-25 14:49:48Calling greater attention to sub-Saharan Africa’s pressing challenges in pediatric cardiac care
In a new observational study, researchers provide insight into key features distinguishing MIS-C patients to provide a more realistic picture of the burden of disease in the pediatric population and aid with the early detection of disease and treatment for optimal outcomes.
Multisystem Inflammatory Syndrome in Children (MIS-C) significantly affected more Black and Latino children than white children, with Black children at the highest risk, according to a new observational study of 124 pediatric patients treated at Children’s National Hospital in Washington, D.C. Researchers also found cardiac complications, including systolic myocardial dysfunction and valvular regurgitation, were more common in MIS-C patients who were critically ill. Of the 124 patients, 63 were ultimately diagnosed with MIS-C and were compared with 61 patients deemed controls who presented with similar symptoms but ultimately had an alternative diagnosis.
In the study, published in The Journal of Pediatrics, researchers provide insight into key features distinguishing MIS-C patients to provide a more realistic picture of the burden of disease in the pediatric population and aid with the early detection of disease and treatment for optimal outcomes. The COVID-linked syndrome has affected nearly 4,000 children in the United States in the past year. Early reports showed severe illness, substantial variation in treatment and mortality associated with MIS-C. However, this study demonstrated that with early recognition and standardized treatment, short-term mortality can be nearly eliminated.
“Data like this will be critical for the development of clinical trials around the long-term implications of MIS-C,” says Dr. Roberta DeBiasi, M.D., lead author and chief of the Division of Pediatric Infectious Diseases at Children’s National. “Our study sheds light on the demographic, clinical and biomarker features of this disease, as well as viral load and viral sequencing.”
Of the 63 children with MIS-C, 52% were critically ill, and additional subtypes of MIS-C were identified including those with and without still detectable virus, those with and without features meeting criteria for Kawasaki Disease, and those with and without detectable cardiac abnormalities. While median age (7.25 years) and sex were similar between the MIS-C cohort and control group, Black (46%) and Latino (35%) children were overrepresented in the MIS-C group, especially those who required critical care. Heart complications were also more frequent in children who became critically ill with MIS-C (55% vs. 28%). Findings also showed MIS-C patients demonstrated a distinct cytokine signature, with significantly higher levels of certain cytokines than those of controls. This may help in the understanding of what drives the disease and which potential treatments may be most effective.
In reviewing viral load and antibody biomarkers, researchers found MIS-C cases with detectable virus had a lower viral load than in primary SARS-CoV-2 infection cases, but similar to MIS-C controls who had alternative diagnoses, but who also had detectable virus. A larger proportion of patients with MIS-C had detectable SARS-CoV-2 antibodies than controls. This is consistent with current thinking that MIS-C occurs a few weeks after a primary COVID-19 infection as part of an overzealous immune response.
Viral sequencing was also performed in the MIS-C cohort and compared to cases of primary COVID-19 infection in the Children’s National geographic population. 88% of the samples analyzed fell into the GH clade consistent with the high frequency of the GH clade circulating earlier in the pandemic in the U.S. and Canada, and first observed in France.
“The fact that there were no notable sequencing differences between our MIS-C and primary COVID cohorts suggests that variations in host genetics and/or immune response are more likely primary determinants of how MIS-C presents itself, rather than virus-specific factors,” says Dr. DeBiasi. “As we’ve seen new variants continue to emerge, it will be important to study their effect on the frequency and severity of MIS-C.”
Researchers are still looking for consensus on the most efficacious treatments for MIS-C. In a recent editorial in the New England Journal of Medicine, Dr. DeBiasi calls for well-characterized large prospective cohort studies at single centers, and systematic and long-term follow-up for cardiac and non-cardiac outcomes in children with MIS-C. Data from these studies will be a crucial determinant of the best set of treatment guidelines for immunotherapies to treat MIS-C.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/06/little-boy-at-doctors.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2021-06-25 11:34:002021-07-28 11:56:16Demographic, clinical and biomarker features of MIS-C