In 2025, Innovation District readers gravitated toward stories that explored how research and clinical innovation are reshaping pediatric care in real time. This year’s most popular articles highlighted advances in complex surgical care, evidence-based treatments for chronic and neuropsychiatric conditions and emerging technologies — from wearable data to artificial intelligence — that are changing how clinicians diagnose, treat and support children and families. Read on for our list of the most popular articles we published on Innovation District in 2025.
The Cervical Spine program at Children’s National Hospital is responsible for treating a range of conditions, including trauma, congenital abnormalities and tumors. These conditions can lead to instability or misalignment of the cervical spine. “There are unique challenges in pediatric cases due to anatomical differences. The cervical spines of children are more at risk for injury because of their developmental stage and structural characteristics,” says Matthew Oetgen, MD, MBA, chief of Orthopaedic Surgery and Sports Medicine at Children’s National. (2 min. read)
Increasing evidence-based treatment is a key component of the Addictions Program at Children’s National Hospital, created in 2022 and led by Sivabalaji Kaliamurthy, MD. “We really want to focus on intervening in an evidence-based manner in the primary care setting because that is where most of our patients are going to first access care outside of the emergency room,” explains Dr. Kaliamurthy. (3 min. read)
For many children with short stature and other rare genetic growth disorders, there have been no next steps after usual treatment options prove ineffective. Researchers at Children’s National Hospital are digging deeper to find the root genetic causes of short stature disorders and creating novel, nuanced treatment options that have the opportunity to change how the field approaches these cases. (4 min. read)
Denver D. Brown, MD, nephrologist at Children’s National, is looking at whether untreated metabolic acidosis could potentially contribute to cardiovascular outcomes in children with chronic kidney disease (CKD). Here, she explains her motivation, findings and future directions for this critical research. (3 min. read)
A multidisciplinary therapy model developed at Children’s National shows promise for children with PANS and PANDAS, significantly reducing symptoms through structured cognitive-behavioral therapy and family-centered care. The approach could offer a new standard for treating these rare, complex neuropsychiatric disorders. (2 min. read)
A study from Children’s National reveals that common wearable devices like Fitbits may hold the key to improving how we identify Attention-Deficit/Hyperactivity Disorder (ADHD) in adolescents. By analyzing patterns in heart rate, activity levels and energy expenditure, researchers were able to predict ADHD diagnoses with striking accuracy, offering a glimpse into a future where objective, real-time data supports earlier and more personalized mental healthcare. (2 min. read)
A novel implantable pacemaker designed specifically for infants has demonstrated safety and effectiveness in stabilizing heart rhythms for at least two years. The multi-center study of 29 infants showed stable pacing, normal electrical parameters and expected battery life, offering a viable alternative to standard-size devices for the smallest children. (2 min. read)
Children who had heart surgery and come from less advantaged neighborhoods in the Washington, D.C., region are much more likely to die in the long term than those from neighborhoods with more wealth and opportunity. The finding was part of a presentation titled, Socioeconomic Disadvantage Is Associated with Higher Long-Term Mortality After Cardiac Surgery, by Jennifer Klein, MD, MPH, cardiologist at Children’s National Hospital, during the Society of Thoracic Surgeons Annual Meeting in Los Angeles. (2 min. read)
Experts from Children’s National traveled to Uganda to continue work on a pilot program applying artificial intelligence (AI) to the diagnosis of rheumatic heart disease (RHD). The team created a tool that uses AI to predict RHD by identifying leaky heart valves on handheld ultrasound devices, then prompts a referral for a full echocardiogram. (2 min. read)
Food insecurity is rising in Washington, D.C. and it’s hitting families with children the hardest. That’s why Children’s National Hospital created the Family Lifestyle Program (FLiP) – a multi-layered intervention, which offers Patient Navigation (FLiP-PN) and a Produce Prescription Intervention (FLiPRx). FLiP is a Food Is Medicine, clinical-community initiative that helps families get access to fresh food, build healthy habits and lower their risk of diet-related diseases like diabetes and obesity. (3 min. read)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/12/2025-with-lightbulb-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-12-24 15:07:522025-12-24 16:43:36The best of 2025 from Innovation District
In 2025, Children’s National Hospital was featured in major national news outlets for pioneering advances in pediatric care, groundbreaking clinical research and powerful human stories of healing and hope. From gene therapy for sickle cell disease and innovative pacemakers for newborns to breakthrough transplants, cancer trials and emerging mental health concerns like AI psychosis, these stories highlight the hospital’s leadership across the full spectrum of pediatric medicine. The following ten highlights showcase the patients, families and experts behind this impact, as reported by outlets including NBC News, The Washington Post, Good Morning America, USA Today, Healio, ABC News and ESPN.
Children’s National patient Wedam, 19, begins the first steps for intensive gene therapy for sickle cell disease, discussing his skepticism while his mother expresses her joy and gratitude for the treatment. (NBC News)
Charles Berul, MD, pediatric electrophysiologist and emeritus chief of Cardiology, discusses his study highlighting the safety and efficacy of an innovative smaller pacemaker designed for newborns with critical congenital heart disease. (Healio)
Catherine Bollard, MBChB, MD, senior vice president and chief research officer, and the NexTGen team are poised to recruit patients for a new clinical trial that will take on an old, implacable foe: children’s solid tumors. (The Washington Post)
Yves d’Udekem, MD, PhD, chief of Cardiac Surgery, talked to Good Morning America about how an 11-year-old’s groundbreaking partial heart transplant will change his life and the lives of other children in need of valve replacements. (Good Morning America)
The Lilabean Foundation along with Brian Rood, MD, medical director of the Brain Tumor Institute, talked about how patients like Kasey Zachman are the motivation behind finding a cure for brain cancer. (ABC News)
USA Today Sports spoke with Gavin Brown and his parents, as well as Yi Shi, MD, a pediatric nephrologist at Children’s National Hospital, about their kidney transplant journey. (USA Today)
After Jayden Daniels visited Commanders fan Sarah Addison at Children’s National Hospital while she was being treated for myeloid leukemia, they quickly became friends. (ESPN)
A baby boy in Maryland is back home after being given a second chance at life, just before his first birthday. The boy’s mother and his surgeon, Manan Desai, MD, share the remarkable story of a moment that changed all of their lives. (NBC4)
Ashley Maxie-Moreman, PhD, clinical psychologist, spoke to ABC7 about what AI psychosis is and what parents need to know. (ABC7)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/12/Logo-Collage-2025-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-12-23 13:53:592025-12-31 09:09:17Children’s National in the News: 2025
The annual conference brings together leading clinicians, researchers and innovators from across Neurology, Neurosurgery, Neuro-critical Care, Neurogenetics and Neuroradiology to share the latest insights driving the future of pediatric neuroscience. This year’s program explored the epidemiology and mechanisms of neurological diseases, cutting-edge clinical trials, AI innovations and new models of integrated, high-impact care.
Elizabeth Wells, MD, senior vice president of the Neuroscience and Behavioral Medicine Center at Children’s National and a member of the conference’s Scientific Committee, highlighted the continued impact of this international partnership. “By training and supporting physicians and allied health staff across the region, we’re expanding access to quality care close to home,” said Dr. Wells. “But when children require complex interventions or innovative treatments that aren’t available locally, Children’s National is ready to provide that next level of care. We’re proud to serve both as a partner in strengthening regional capacity and as a global leader in the most advanced pediatric neuroscience therapies.”
“It was a great pleasure to partner once again with Children’s National for this year’s Pediatric Neuroscience Conference,” said Ruba Benini, FRCPSC, MD, PhD, medical director of the Neurodiagnostic Laboratory at Sidra Medicine. “Their high-caliber speakers and the depth of experience they brought to the conference added tremendous value, and we look forward to continuing our collaboration in the future.”
Children’s National brought the largest contingent of external speakers to this year’s meeting, presenting across multiple high-visibility sessions:
Scientific Sessions & Presentations
SESSION II: Neuro-Immunology
Drs. William D. Gaillard, Adelaide Robb and Karen Smith at the 2025 Pediatric Neuroscience Conference.
Elizabeth Wells, MD — Autoimmune Encephalitis – Updates on Diagnosis & Treatment
SESSION III: Neuro-Oncology
Elizabeth Wells, MD — Session Moderator
Robert Keating, MD — Latest Advances in Non-Invasive Focused Ultrasound Treatment for Brain Tumors
SESSION IV: Neurogenetics and Precision Medicine in Neurological Disorders
Sarah Wright, MD — Progress and Innovations in Clinical Trials for Neuromuscular Diseases
William D. Gaillard, MD — Developments in Epilepsy Clinical Trials: Emerging Therapies and Technologies
SESSION V: Epilepsy Symposium
William D. Gaillard, MD — Epilepsy Surgery: Patient Selection, Evaluation and Outcomes
Chima Oluigbo, MD — Advances in Epilepsy Surgery: Options and Procedures
Adelaide Robb, MD — Neuropsychiatric Co-Morbidities in Pediatric Epilepsy
SESSION VI: Complex Neurosurgical Procedures
Robert Keating, MD — Two Decades of Experience With Chiari Malformations: Where Are We Today?
SESSION VII: Artificial Intelligence and Cutting-Edge Research in Neuroscience
Chima Oluigbo, MD — Artificial Intelligence in Neurosurgery: Transforming Diagnosis, Treatment, and Patient Outcomes
Following the conference, Dr. Adelaide Robb and Dr. William D. Gaillard presented Grand Rounds for the psychiatry and neurology departments at Sidra Medicine, further strengthening the educational and clinical collaboration between institutions.
“Our work in the Gulf is rooted in a simple belief: every child deserves access to cutting-edge care and the hope it brings,” says Karen Smith, MD, executive medical director of Global Services at Children’s National. “By partnering with hospitals and government leaders across the region, we’re not only sharing expertise—we’re building sustainable systems that empower communities and transform outcomes for children for years to come.”
Global leaders in pediatric neuroscience, including experts from Children’s National, gather at the 2025 Pediatric Neuroscience Conference in Qatar.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/12/2025-Pediatric-Neuroscience-attendees-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-12-17 13:32:032025-12-17 13:33:56Showcasing global expertise: Children’s National at the 2025 Pediatric Neuroscience Conference in Qatar
Among the 182 patients studied, researchers found that CoQ10 supplementation was significantly more common among children whose headaches ultimately resolved.
A new study from neurology experts at Children’s National Hospital suggests that Coenzyme Q10 (CoQ10) may play a meaningful role in the resolution of new daily persistent headache (NDPH), a rare, debilitating and historically treatment-resistant condition in children. This study analyzed 182 pediatric patients evaluated over six years, making it the largest single-center study of NDPH ever conducted.
Progress in NDPH research has been slow, particularly in the pediatric population. The condition is both rare and highly heterogeneous, making research and controlled trials challenging. Many patients present only after experiencing long-standing symptoms and multiple unsuccessful treatments, complicating efforts to isolate which interventions are truly effective. Additionally, most pediatric headache studies and all industry-sponsored clinical trials specifically exclude children with continuous daily headaches like NDPH.
These obstacles have left clinicians with little evidence-based guidance and families with a trial-and-error approach that can feel discouraging. This new analysis offers hope, highlighting potential treatment avenues and underscoring the need for prospective, controlled studies.
What the study found
Among the 182 patients studied, researchers found that CoQ10 supplementation was significantly more common among children whose headaches ultimately resolved. While other interventions including magnesium, topiramate, onabotulinum toxin A and regular aerobic exercise showed encouraging trends, CoQ10 was the only treatment associated with statistically significant improvement.
“This is the first potential treatment signal we’ve seen in pediatric NDPH,” Dr. Takle explained. “Very few therapies have shown measurable impact in this population, so identifying an association with Coenzyme Q10 is particularly exciting.” The consistency of positive trends across other migraine-related treatments also suggests that NDPH may share more therapeutic overlap with migraine than previously assumed, an insight that could help reshape how clinicians think about the disorder.
Impact on patients and care
For families, the findings offer something the field has long lacked: a more informed starting point. NDPH is notoriously treatment-resistant, and many patients cycle through medications and lifestyle adjustments with little clarity on what may help. The study’s results provide clinicians with data-backed options to guide therapy, hopefully bringing relief to patients sooner.
Emphasizing lifestyle factors such as regular aerobic exercise also gives families accessible, proactive strategies that may support symptom improvement.
Children’s National leads the way
Children’s National houses one of the largest and most systematically characterized pediatric headache registries, enabling the type of robust analysis rarely possible in NDPH research. The hospital’s multidisciplinary Headache Program, led by Dr. Marc DiSabella, has developed standardized evaluations and long-term follow-up that support high-quality data collection and clinical insight.
This study is the first to identify CoQ10 as a potential contributor to symptom resolution in pediatric NDPH, highlighting the unique role Children’s National plays in advancing both scientific understanding and patient care for this challenging disorder.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/12/Coenzyme-Q10-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-12-16 10:14:092025-12-16 10:15:21CoQ10 linked to symptom resolution in children with New Daily Persistent Headache
Dr. Cimino began his role as a principal investigator in the Children’s National Research Institute in October 2025. He will lead new research and bring experts together across the Center for Cancer and Immunology Research, the Brain Tumor Institute and the Division of Pathology and Laboratory Medicine.
The big picture
Dr. Cimino joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Children’s National is grateful to generous donors who have altogether funded 51 professorships.
Professorships support groundbreaking work on behalf of children and their families. They foster new discoveries and innovations in pediatric medicine. These appointments carry prestige and honor that reflects both the recipient’s achievements and the donor’s commitment to advancing and sustaining knowledge.
Why it matters
Dr. Cimino is a nationally recognized physician-scientist and board-certified neuropathologist. He specializes in the molecular genetics of gliomas. His work looks at brain and central nervous system tumors at the molecular level to understand how and why they develop, and guide more accurate diagnosis and treatment. At Children’s National, he will provide clinical pathology and neuropathology services and lead research that contributes to better therapies and patient outcomes.
Previously, Dr. Cimino served as head of the Neuropathology Unit in the Surgical Neurology Branch at the National Institute of Neurological Disorders and Stroke, part of the National Institutes of Health.
“It’s an honor to join Children’s National and become the first Professor of Molecular Neuropathology,” Dr. Cimino says. “I’m grateful to the generous donor who made this possible, and to the hospital for their trust and vision. Our shared commitment and collaboration to uncover what drives hard-to-treat tumors will lead to real breakthroughs for kids and families.”
Moving the field forward
This appointment was made possible by a $96 million strategic investment from an anonymous family in 2023 to advance pediatric brain tumor research and care. It is one of the largest donations in the hospital’s history, and is transforming the ability to give patients a better chance at healthy lifetimes. The Professorship in Molecular Neuropathology is the third created through this investment, which previously endowed the McCullough Distinguished Professorship in Neurosurgery and the Kurt D. Newman, MD, Professorship in Neuro-Oncology. The investment also elevated the Dr. Robert J. and Florence T. Bosworth Distinguished Professorship in Cancer and Transplantation Biology Research and fully funded the William Seamus Hughes Professorship in Neuro-Oncology and Immunology.
Through this incredible investment, Children’s National continues to partner with global experts to lead a powerful, collaborative effort to change what’s possible for children with brain tumors. It unites researchers and clinicians across disciplines to advance the science — developing new, often first-in-child therapies — while improving every aspect of care, from medical treatment to the psychosocial well-being of patients and their families.
“The vision of the anonymous family continues to create lasting impact,” says Roger J. Packer, MD, director of the Brain Tumor Institute and The Gilbert Distinguished Professor of Neurofibromatosis. “Dr. Cimino is an exceptional leader and scientist. We are thrilled to have him as the inaugural Professor of Molecular Neuropathology. His expertise brings exactly what we needed to move this work forward and deepen our understanding of how tumors grow and change.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/12/Patrick-Cimino-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-12-02 08:00:462026-01-05 17:14:03Patrick Cimino, MD, PhD, joins Children’s National as inaugural Professor of Molecular Neuropathology
Fetal alcohol spectrum disorders (FASD) are among the most common preventable causes of developmental disability, affecting an estimated 2% to 5% of children in the United States and Western Europe.
Fetal alcohol spectrum disorders (FASD) are among the most common preventable causes of developmental disability, affecting an estimated 2% to 5% of children in the United States and Western Europe. Yet despite their prevalence, treatment options remain limited, particularly for the cognitive and behavioral challenges that persist throughout life.
Researchers at Children’s National Hospital are working to change that. Through a new $2 million award from the National Institute on Alcohol Abuse and Alcoholism (NIAAA), investigators are advancing the development of a first-of-its-kind drug designed to improve learning and behavior in individuals with FASD.
Dive deeper
The study at Children’s National is led by site principal investigators Li Wang, PhD, and Anup Srivastava, PhD, in the Center for Neuroscience Research. The overall project is led by Masaaki Torii, PhD, in his role as principal investigator at a partnering start-up company co-founded by other Children’s National investigators, Kazue Hashimoto-Torii, PhD, and Hiroki Morizono, PhD, who contribute to the study in their company roles.
The research builds on discoveries made at Children’s National about how prenatal alcohol exposure disrupts brain development. The team identified a potassium channel called KCNN2, whose overactivity appears to play a key role in the neurobehavioral symptoms seen in FASD. To address this mechanism, the researchers developed FA-1, a small peptide compound that blocks KCNN2 activity. When delivered intranasally in preclinical models, FA-1 improved multiple behavioral outcomes, suggesting a potential path toward a targeted therapy.
The newly funded Phase II Small Business Technology Transfer (STTR) project will take FA-1 further along the translational pipeline. Researchers will optimize its intranasal formulation and evaluate its pharmacology, efficacy and safety in pre-clinical models. These studies will generate the data needed for an investigational new drug (IND) application with the U.S. Food and Drug Administration (FDA), paving the way for early clinical testing.
Why it matters
Fetal alcohol spectrum disorders currently have no FDA-approved medication that targets the root neurobiological causes of the disorder. Most available treatments only manage symptoms such as attention deficit or anxiety. If successful, FA-1 could become the first drug to directly improve the cognitive and behavioral functions affected by prenatal alcohol exposure.
“This project is an important step toward bringing a true, biology-based treatment for FASD to the children and families who need it,” said Drs. Wang and Srivastava. “The NIH’s support, combined with our partnership with the start-up, allows us to translate our discoveries at Children’s National into a therapy that we hope will make a meaningful difference in patients’ lives.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/11/pregnant-woman-wine-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-11-07 16:05:502025-11-07 16:07:22Researchers advance new drug development for fetal alcohol spectrum disorders
As children mature into adolescence, their hippocampus becomes increasingly specialized along its longitudinal axis, contributing to the development of memory and other cognitive functions.
In a study published in PNAS (Proceedings of the National Academy of Sciences), researchers found that the hippocampal gradient and its distinct connections with cortical systems are essential for memory development in children.
“This study is important because it helps us understand how the hippocampus develops and how it communicates with the rest of the brain to form episodic memory, or long-term memories of specific events,” said Hua (Oliver) Xie, PhD, research faculty at Children’s National Hospital and assistant professor at The George Washington University.
The big picture
Researchers looked at two resting-state functional magnetic resonance imaging (fMRI) datasets. The primary dataset included 598 participants between the ages of 8 and 21 and a secondary replication dataset of 196 participants from the Nathan Kline Institute (NKI)-Rockland Sample. Participants were scanned for a total of 26 minutes in resting-state where they stayed still, awake and looked at the fixation crosshair.
The results showed that the head and tail of the hippocampus form distinct communication patterns with other brain regions, which can help predict how well children form episodic memories.
As children mature into adolescence, their hippocampus becomes increasingly specialized along its longitudinal axis, contributing to the development of memory and other cognitive functions.
The hold up in the field
Previous studies have primarily focused on the hippocampus, with many researchers treating the anterior and posterior regions as distinct areas of study. By exploring how the hippocampus communicates with other parts of the brain, this study reveals a more comprehensive understanding than before.
“Our research shows that in children, it’s more of a gradual transition of function along the hippocampus’s long axis, like a color gradient rather than two distinct blocks,” Dr. Xie said.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/hippocampus-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-10 16:32:402025-10-10 16:33:37Mapping the brain’s memory gradient: How the hippocampus helps children form lasting memories
Children’s National Hospital’s Neuroimmunology Program has been named a Pediatric Center of Excellence in Rare Neuroimmune Disorders by the Siegel Rare Neuroimmune Association.
The program is led by Elizabeth Wells, MD, Senior vice president of the Neuroscience and Behavioral Medicine Center, Alexandra Kornbluh, MD, director of Neuroimmunology Investigational Therapeutics, and Ilana Kahn, MD, clinical director of Neuroimmunology. Together, they oversee a multidisciplinary team providing state-of-the-art diagnosis, treatment and long-term management for children with antibody-mediated autoimmune encephalitis (AE), acute disseminated encephalomyelitis (ADEM), febrile infection related epilepsy syndrome (FIRES), multiple sclerosis (MS), neuromyelitis optica spectrum disorders (NMOSD), myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), opsoclonus myoclonus ataxia syndrome (OMAS), transverse myelitis (TM), optic neuritis (ON), primary CNS vasculitis and other central nervous system demyelinating and inflammatory conditions.
As a designated CERND, Children’s National offers:
Expert-led care: Specialists at the forefront of clinical practice and research.
Comprehensive services: Coordinated care across neurology, neurosurgery, neuropsychology, psychiatry, psychology, neuroradiology, physical medicine and rehabilitation, critical care, social work, pharmacy and speech therapy.
Research opportunities: Access to clinical trials and studies that drive progress in therapies and patient outcomes.
In addition to delivering high-quality clinical care, the program partners with SRNA to expand educational resources for patients, families and clinicians. Its work aligns with SRNA’s broader objectives to strengthen the CERND network, support innovative research and improve both acute therapies and long-term management strategies for rare neuroimmune disorders.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/2025-CERND-Pediatric-Seal-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-09 11:44:062026-01-05 17:33:05Children’s National Hospital designated Pediatric Center of Excellence in Rare Neuroimmune Disorders
A new $8 million investment from the Gilbert Family Foundation will support groundbreaking research on neurofibromatosis type 1 (NF1) at Children’s National Hospital. The generous five-year grant continues the Foundation’s longstanding research partnership with the hospital. It will accelerate investigations aimed at improving the lives of children and young adults affected by this genetic condition.
“This grant will enable us to expand basic science, translational and clinical research. It will help us perform two to three innovative clinical trials in the next five years — trials we will share with the NF community as a whole,” says Roger J. Packer, MD, the Gilbert Family Distinguished Professor of Neurofibromatosis at Children’s National.
Dr. Packer will lead the research team, which also includes Javad Nazarian, PhD, Steven Stasheff, MD, Karin S. Walsh, PsyD and Sridevi Yadavilli, MD, PhD.
Why this matters
NF1 is one of the most common genetic conditions in young people. It affects approximately 1 in 2,500 children born each year. It causes potentially deadly nervous system tumors and can pose lifelong health complications. These include vision and learning disabilities, skeletal abnormalities and increased cancer risks.
Dive deeper
The new funding will:
Fuel clinical trials testing new therapies that combine MEK inhibitors, which block tumor growth, and checkpoint inhibitors, which help the immune system attack cancer, to treat aggressive NF1 brain tumors. Trials will target high-grade astrocytomas with piloid features (HGAPs) and recalcitrant gliomas. The goal is to improve outcomes for these aggressive tumors by enhancing the body’s immune response to cancer.
Drive cognitive research to understand learning, behavior and social deficits in children with NF1.
Better detect and understand vision loss in children with optic pathway tumors. Discoveries will help doctors predict, treat and prevent disease progression as well as assess the potential benefits of treatment.
Build novel lab models to supercharge drug discovery. The grant will support the expansion and validation of investigational models, including the development of NF1 zebrafish models and patient-derived organoids. NF1 tumor organoid tissues, grown in the lab, mimic the functioning of an actual organ.
Children’s National Leads the Way
In 2007, Dan and Jennifer Gilbert established The Gilbert Family Neurofibromatosis Institute at Children’s National. The Institute advances basic and clinical research, providing a global destination for care. The Gilbert family endowed three professorships that help the hospital advance the field.
Previous funding from the Gilbert Family Foundation has improved our understanding of NF1-related gliomas and how best to treat them. It has supported pioneering work in evaluating the safety and cognitive benefits of novel treatments, primarily MEK inhibitors. The Foundation’s new award will build upon this work. It will yield new insights into one of the most lethal manifestations of NF1: transformation of low-grade gliomas into malignant lesions. Children’s National will explore novel therapies, including immunotherapy, with the potential to save lives.
Gilbert Family Neurofibromatosis Institute accomplishments include:
Becoming one of the leading programs in the Sarcoma Alliance for Research through Collaboration (SARC Alliance) for developing new molecularly-targeted therapies
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
For the fifteenth straight year, Children’s National ranked in 10 specialty services and is the highest U.S. News ranked children’s hospital in Washington, D.C., Maryland and Virginia. Last year, U.S. News introduced pediatric & adolescent behavioral health as a service line in its rankings. While there are no ordinal rankings for behavioral health, the Children’s National program was named one of the top 50 programs in the country for the second year in a row.
“To be named among the nation’s top children’s hospitals for nine years in a row is a reflection of the extraordinary expertise, innovation and heart that our teams bring to every child and family we serve,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “Our leadership in specialties like neurology, cancer, and diabetes and endocrinology underscores the national impact of our work, and we remain focused on setting new standards in pediatric care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“Being a top-ranked pediatric hospital means more than just excelling in a single specialty — it means being a pillar of outstanding care for your entire region,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Our rankings acknowledge these hospitals for their comprehensive excellence, helping families find the very best care conveniently located within their state and community.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/USNWR_CNBadges_Set2SideBySide_2025-26-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-07 01:00:072026-01-05 17:33:17Children’s National Hospital once again ranked among the nation’s best by U.S. News & World Report
Physicians, fellows and faculty from the Neuroscience and Behavioral Medicine Center at Children’s National Hospital will participate in this year’s Child Neurology Society (CNS) Annual Meeting, held October 8–11 in Charlotte, North Carolina. This premier gathering offers child neurologists the opportunity to exchange knowledge, foster collaboration, share research and advance patient care in the field.
Experts from Children’s National will be featured throughout the program, showcasing their leadership and expertise across a range of sessions and presentations.
Speakers and topics
Wei-Liang Chen MD Seminar 9: Games Neurologists Play: AI for Enhanced Diagnosis in Neurology – Brain2Gene – Next Generation Phenotyping Using Artificial Intelligence to Predict the Genetic Diagnosis by Brain MRI Analysis Friday, October 10, 2025 – 9:30-10:45 AM EDT/EST
Marc DiSabella, DO Seminar 8: The Evolution of Migraine Disease from Childhood to Young Adult Friday, October 10, 2025 – 9:30-10:45 AM EDT/EST
Hannah Grindling, MMSc, GC CNS Genetics Summit: Demystifying Next-generation Sequencing: A Hands-On Workshop for Pediatric Neurologists Saturday, October 11, 2025 – 12:30-4:30 PM EDT/EST
Dana Harrar MD, PhD Seminar 7: Optimizing NeuroICU Care: Treating Patients Rather Than Seizures – Novel Therapies and Thresholds Friday, October 10, 2025 – 9:30-10:45 AM EDT/EST
Ilana L Kahn, MD Seminar 2: Updates in Pediatric Multiple Sclerosis Thursday, October 9, 2025 – 2:00-3:15 PM EDT/EST
Alexandra B. Kornbluh, MD Seminar 2: Updates in Pediatric Multiple Sclerosis – Updates in MS Diagnostic Criteria and Implications for Pediatric MS Treatment Thursday, October 9, 2025 – 2:00-3:15 PM EDT/EST
Juma Shee Mbwana, MD Symposium III: Year in Review Symposium – Global Pediatric Neurology Saturday, October 11, 2025 – 9:00 AM-12:00 PM EDT/EST
John Schreiber, MD CNS Genetics Summit: Demystifying Next-generation Sequencing: A Hands-On Workshop for Pediatric Neurologists Saturday, October 11, 2025 – 12:30-4:30 PM EDT/EST
Kuntal Sen, MD Workshop 7: Discovering Mentors: Early Career Leadership Guidance Wednesday, October 8, 2025 – 3:00-4:00 PM EDT/EST CNS Genetics Summit: Demystifying Next-generation Sequencing: A Hands-On Workshop for Pediatric Neurologists Saturday, October 11, 2025 – 12:30-4:30 PM EDT/EST
Jeffrey Strelzik, MD Seminar 8: The Evolution of Migraine Disease from Childhood to Young Adult – Migraine Disease in Early Childhood Friday, October 10, 2025 – 9:30-10:45 AM EDT/EST CNS Genetics Summit: Demystifying Next-generation Sequencing: A Hands-On Workshop for Pediatric Neurologists Saturday, October 11, 2025 – 12:30-4:30 PM EDT/EST
Sinan Turnacioglu, MD Seminar 9: Games Neurologists Play: AI for Enhanced Diagnosis in Neurology Friday, October 10, 2025 – 9:30-10:45 AM EDT/EST
Spectrum of Neurofascin-155 Antibody Mediated Paranodopathy in a Pediatric Cohort: A Single Center Experience, Allison Saunders, MD
Additionally, Dr. DiSabella will be honored with the prestigious Program Director Award, recognizing his outstanding leadership in education, mentorship and curriculum development within child neurology and neurodevelopmental pediatrics.
For more information and to view the full schedule, please visit the CNS conference website.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/CSN-Annual-Conference-2025-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-03 15:09:532026-04-20 16:03:31Children’s National experts at the Child Neurology Society 2025 Annual Meeting
A joint study from Children’s National and UCLA findound that peak alpha frequency (PAF), a simple EEG signal, may help track brain growth in Angelman syndrome.
Angelman syndrome (AS) affects how a child’s brain develops and communicates. Families often face limited or absent speech, seizures, sleep problems and global delays. As several treatments move through late-stage trials, teams need clear ways to see if a therapy is changing the brain. A joint study from Children’s National Hospital and the University of California, Los Angeles (UCLA) points to a simple signal from an electroencephalogram (EEG), a test that records brain activity through small sensors on the scalp.
The signal is called peak alpha frequency (PAF). Alpha is a natural brain rhythm. In most children, the speed of this rhythm rises through childhood as networks mature. The study shows that this pattern is different in Angelman syndrome. Many children with AS have no clear alpha peak. When a peak is present, it is slower than in peers and does not speed up with age. That pattern suggests stalled or altered maturation of brain circuits.
Researchers looked at hundreds of EEGs from children with AS and from age-matched peers. They measured alpha activity in two independent ways to make sure the results were not due to a single analysis choice. Both approaches told the same story. In children who are typically developing, more than nine out of ten EEGs showed a distinct alpha peak, and that peak tended to get faster with age. In children with AS, fewer than half of EEGs showed a peak. When a peak appeared, it sat at a lower frequency and stayed flat across ages.
The team also confirmed a second feature of Angelman EEGs that others have reported: more slow-wave (delta) activity and less overall alpha power than peers. Taken together, these signals point to broad differences in how circuits work in Angelman syndrome.
What could this mean for care and for trials? EEG is familiar, safe, and widely available. If a therapy begins to change how circuits function, that shift could show up in PAF before day-to-day behavior changes are obvious. Adding PAF to trial measures could give clinicians and families an earlier read on brain effects. It can also sit alongside delta power to give a fuller picture – delta reflects broad disruption, while PAF tracks the speed of a key rhythm tied to growth.
There are limits to keep in mind. The EEGs came from several sites and systems, and some recordings were longer than others. The team accounted for these factors in their models, but future work with unified setups will help. A major next step is to follow the same children over time to see whether PAF changes within a child and how those changes relate to speech, movement, seizures, or sleep. The study also hints that genetic subtypes may differ, which could sharpen how trials are designed.
This project was a true collaboration between Children’s National Hospital (PI and corresponding author: Michael S. Sidorov, PhD, co-first author: Sapphire Bowen-Kauth) and UCLA (co-first author: Abigail H. Dickinson, PhD), with contributions from colleagues across both centers. Funding came from the Foundation for Angelman Syndrome Therapeutics (FAST).
For families, the takeaway is hopeful. A routine test can capture a signal linked to brain growth. In Angelman syndrome, that signal is often missing or slow, but it can be measured and tracked. As trials continue, PAF may help teams spot early signs that a therapy is reaching the brain’s core rhythms, information that matters for decisions in clinics and for progress in research.
Read the full study, “Atypical alpha oscillatory EEG dynamics in children with Angelman syndrome,” in Neuroimage: Clinical.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/brain-cutout-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-09-25 11:34:362025-09-25 11:35:36A new electroencephalogram (EEG) measure may help track brain growth in Angelman syndrome
“This award is a tremendous honor,” said Dr. Bramble, principal investigator in the Center for Precision Medicine and Genomics Research at Children’s National. “It will allow us to push the boundaries of our work and explore new ways to understand and treat devastating childhood diseases.”
Children’s National Hospital is proud to congratulate Matthew Bramble, PhD, on being named a 2025 Pew Scholar in the Biomedical Sciences. This highly competitive honor recognizes outstanding early-career researchers who are driving innovation and discovery in human health. Dr. Bramble is one of just 22 scientists nationwide selected this year to join the Pew Scholars Program, which provides four years of funding and access to a network of more than 1,000 leading biomedical researchers.
“This award is a tremendous honor,” said Dr. Bramble, principal investigator in the Center for Precision Medicine and Genomics Research at Children’s National. “It will allow us to push the boundaries of our work and explore new ways to understand and treat devastating childhood diseases.”
Dive deeper
Dr. Bramble’s research focuses on konzo, a little-known but serious neurological condition that causes sudden and irreversible paralysis in children. Konzo primarily affects families in rural regions of sub-Saharan Africa who rely on improperly processed cassava as a staple food. The disease is linked to compounds in cassava that become toxic when combined with poor nutrition.
“Konzo is heartbreaking because it strikes vulnerable children and is entirely preventable,” said Dr. Bramble. “If we can better understand the molecular pathways that lead to paralysis, we can develop strategies to protect children and potentially inform treatments for other neurological disorders.”
His lab uses advanced OMIC’s technologies to study how toxins from cassava interact with a child’s biology, aiming to uncover how the disease damages the nervous system. By examining the molecular biology of konzo, Dr. Bramble hopes to reveal insights not only for affected communities abroad but also for understanding broader principles of brain health and development.
Why it matters
The Pew Scholars Program in the Biomedical Sciences, run by The Pew Charitable Trusts, has supported early-career scientists for 40 years. Scholars receive multiyear funding to pursue bold, creative approaches to complex scientific problems. Many alumni have gone on to win major scientific awards and make discoveries that have shaped modern medicine.
For Dr. Bramble, joining the program provides vital support for high-risk, high-reward science and connects him to a collaborative network of researchers across disciplines.
“This award validates the importance of studying conditions like konzo that don’t often receive attention but have a profound impact on children’s lives,” he said.
Dr. Bramble’s recognition underscores not only Children’s National Hospital’s commitment to advancing pediatric research and fostering discoveries that improve children’s health worldwide but also the institution’s commitment to providing resources and a setting for this type of unique, cutting-edge work. By supporting investigators who explore fundamental biology and rare diseases, the hospital helps build the foundation for tomorrow’s treatments.
With the support of the Pew award, Dr. Bramble and his team are poised to deepen their understanding of konzo and its impact on the nervous system—and, in the process, generate insights with far-reaching implications for pediatric neurology.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/08/Matthew-Bramble-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-08-12 11:36:042026-01-05 17:11:20Dr. Matthew Bramble named Pew Scholar in Biomedical Sciences
Marc DiSabella, DO, of Children’s National Hospital has been named the 2025 recipient of the Child Neurology Society (CNS) Training Director Award.
Marc DiSabella, DO, of Children’s National Hospital has been named the 2025 recipient of the Child Neurology Society (CNS) Training Director Award. This national recognition honors program directors who demonstrate outstanding leadership in education, mentorship and curriculum development within child neurology and neurodevelopmental pediatrics.
Dr. DiSabella joined Children’s National and 2008 and currently serves as associate chief of Neurology Operations, director of the Headache Program. He previously led the Child Neurology Residency Program and served as director of Neurology Education.
A dedicated educator, Dr. DiSabella completed the Master Teacher Leadership Development Program at the George Washington University. His innovative teaching style and commitment to excellence have helped raise the bar for neurology education at Children’s National and beyond.
“Dr. DiSabella is an exceptional, enthusiastic and lucid teacher who has introduced several successful innovations over the past 15 years,” said William D. Gaillard, MD, Chief of Neurology at Children’s National. “He has trained more than 50 child neurologists, many now leaders in the field, and built one of the country’s foremost multidisciplinary headache programs. His administrative talents and positive, can-do attitude continue to benefit the entire department.”
Dr. DiSabella will be honored during the CNS Annual Meeting in Charlotte, North Carolina, in October.
The CNS Training Director Award reflects the organization’s mission to recognize the achievements of child neurologists who are model educators, and to recognize those who shape the future of child neurology through education, mentorship and leadership.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/Marc-DiSabella-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-16 12:25:152026-01-05 17:10:50Marc DiSabella, DO, honored with Child Neurology Society 2025 Training Director Award
One of the first and most important steps in fighting brain tumors is to understand exactly where they are and how big they are – using magnetic resonance imaging (MRI) scans.
Brain tumors are the most common cause of cancer-related death in children. These tumors can be very difficult to treat because they often grow in very delicate areas of the brain. One of the first and most important steps in fighting these tumors is to understand exactly where they are and how big they are – using magnetic resonance imaging (MRI) scans.
Traditionally, doctors have had to look at these scans and manually draw outlines around the tumors. This takes a lot of time and can vary from one doctor to another. But what if artificial intelligence (AI) could help make this easier and more efficient?
A recent international research effort called BraTS-PEDs 2023 (short for Brain Tumor Segmentation in Pediatrics) explored exactly that. This challenge co-led by Children’s National Hospital and Children’s Hospital of Philadelphia invited research teams from around the world – including a team led by Marius George Linguraru, DPhil, MA, MSc – to develop the best AI tools for automatically finding and measuring brain tumors in children’s MRIs.
A global AI competition for pediatric care
The BraTS-PEDs 2023 challenge was the first of its kind focused specifically on children. Teams were given MRI scans from 167 pediatric patients with brain tumors collected by leading consortia – the Children’s Brain Tumor Network, DMG/DIPG Registry – and Collaborative Network for Neuro-oncology Clinical Trials and reviewed by volunteer neuroradiologists from the American Society of Neuroradiology. They used these scans to train their AI programs and then tested them on new cases to see how well they performed. Our team’s algorithm was the best at measuring these tumors.
Most teams used a special type of AI network called a “U-Net,” which is great at looking at images and figuring out shapes and boundaries. The challenge showed that AI can do a very good job at finding the tumor and measuring its volume. However, it was more difficult for AI to accurately mark the small, active parts inside the tumor, known as “enhancing tumor” regions.
These results are a huge step forward. Using AI can help doctors make faster, more precise decisions, and reduce differences between hospitals or between individual doctors.
Why this matters
When doctors can accurately map out a brain tumor, they can plan surgery better, target radiation therapy more precisely, and track how well treatments are working over time. This can lead to fewer side effects and better outcomes for children.
In some cases, timely and accurate measurements can even be the difference between life and death. Having advanced AI tools could mean that children get the right treatments faster and with more confidence.
Looking ahead
The research community is now working on including even more data from different hospitals around the world and making the data and algorithm public, like Children’s National has done here. They also plan to study more types of brain tumors and scans taken after surgery and treatments. In the future, AI could become a regular part of how doctors look at brain tumors — like an extra set of smart eyes that never get tired.
At Children’s National, leaders like Dr. Linguraru are helping turn this vision into reality, giving children with brain tumors a better chance at a healthy future. You can read the full study – BraTS-PEDs: Results of the Multi-Consortium International Pediatric Brain Tumor Segmentation Challenge 2023 – in the MELBA Journal.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/brain-scans-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-14 16:57:502026-01-09 16:03:25New advances in AI help doctors understand pediatric brain tumors
A new study from Children’s National Hospital reveals how a minimally invasive procedure is transforming care for infants with hemimegalencephaly and medically refractory seizures, offering seizure relief with fewer surgical risks.
Until recently, families of infants with hemimegalencephaly and medically refractory seizures had few treatment options, almost all involved major brain surgery such as hemispherectomy, to remove or disconnect the affected portion of the brain. These procedures, while sometimes effective, carry high risks in very young infants due to the fragility of their developing brains and invasive nature of the surgery.
Now, specialists from the Hemimegalencephaly Program at Children’s National Hospital have pioneered a minimally invasive alternative. Leveraging the combined expertise of a multidisciplinary team — spanning neurology, neurointerventional radiology, prenatal pediatrics, neonatology, neurogenetics and neurodevelopmental pediatrics, neuropsychology and neurosurgery — they have developed a technique that induces controlled, targeted strokes in the affected hemisphere using transarterial embolization (TAE). This approach mimics the effect of surgery by reducing seizure activity, without the need for open brain procedures.
This novel strategy is the focus of a new study led by Monica Pearl, MD, director of the Neurointerventional Radiology Program. The research represents the largest retrospective review of its kind, examining 41 TAE procedures performed over an 11-year span in 13 infants under three months of age.
The results are promising: 73% of patients achieved Engel Class I seizure outcomes at follow-up, suggesting that with careful technique and patient selection, TAE may provide meaningful seizure control with fewer perioperative risks than traditional surgery. The study also highlights the technical complexity of the procedure, early complications and the critical role of evolving protocols in ensuring patient safety.
A new AI tool developed by Children’s National and Howard University analyzes brain immune cells 10,000x faster than manual methods.
A new machine learning and artificial intelligence tool from researchers at Children’s National Hospital and Howard University (HU) accelerates discoveries in brain inflammation. Called StainAI, it rapidly and accurately analyzes microglia, the brain’s immune cells. Scientists currently analyze microglia slowly by hand. StainAI automates this process and speeds it up 10,000-fold. Its use will aid discovery of new treatments for inflammatory brain conditions such as infection, autoimmunity, and aging.
Solving a problem
Traditionally, scientists study microglia one cell at a time. They reconstruct each cell’s shape by hand under a microscope. The shape helps classify microglia as “resting” (normal) or “activated” (inflamed). The manual process is tedious and slow. It limits analyses to a few microglia in small brain areas.
StainAI changes that. It uses deep machine learning and artificial intelligence to overcome and exceed the manual method’s limitations. It correctly classifies millions of microglia from standard microscopic images. StainAI also localizes each microglia to its brain region in 3D. These features enable single-cell analyses of immune activity at a scale not feasible before – the entire brain.
A tool with broad impact
The team applied StainAI to two models of brain injury and inflammation to show its utility. In a rodent model of pediatric cardiac arrest, StainAI identified new brain regions susceptible to injury. In a simian model of viral infection, StainAI localized rod-shaped microglia normally found in white matter to an unexpected brain region – the hippocampus. These findings point towards new treatments and highlight StainAI’s value across diseases and species.
StainAI is fast, accurate and adaptable. It uses common laboratory equipment. Its creators, Michael Shoykhet, MD, PhD, at Children’s National and Dr. Tsang-Wei Tu at HU, are making StainAI available to other researchers. They hope StainAI will help labs worldwide discover new ways to protect children’s brains from inflammation and injury.
The Children’s National Heart Center team led activities designed to encourage skin-to-skin contact between parents and infants in the Cardiac Intensive Care Unit and Heart and Kidney Unit.
Clinicians at Children’s National Hospital and Children’s Hospital Orange County are leading a nationwide event to encourage families to practice more skin-to-skin, or kangaroo, care with newborn infants who have congenital heart disease, including throughout hospitalization.
Thirty-one hospitals across the United States will participate in this congenital heart disease focused “Skin-to-skin-a-thon,” that will include family and clinical care provider activities and education throughout pediatric cardiac intensive care units and step-down units.
The event will celebrate the tremendous benefits that research shows both families and infants gain from physical contact early in life.
Early skin-to-skin care has been shown to:
Reduce stress in both baby and the parent
Help with baby’s physiologic stability including regulating vital signs like temperature, heart rate, and blood pressure
Provide infant pain relief
Improve infant digestion and weight gain
Support good sleep/wake cycles in babies.
Increase oxytocin for mothers, which can help improve milk production/support breastfeeding
Most studies showing these benefits have included pre-term babies or those born after a healthy term. The idea of encouraging family skin-to-skin care in the hospital setting has been widely adopted in neonatal intensive care units but is not done routinely in cardiac intensive care units. One study estimated that only 6% of parents whose babies were hospitalized for congenital heart disease reported any skin-to-skin care during their stay, with most stays averaging 22 days.
“Research shows so many benefits for all infants and their parents — and our congenital heart newborns stand to gain even more from this type of contact, but often receive it far less,” says Sarah Schlatterer, MD, PhD, medical director of Neurocardiac Critical Care at Children’s National. “This awareness effort is designed to help families understand how to do this safely and also empower our bedside care providers to encourage skin-to-skin care as much as they can every day.”
The event overall is inspired and supported by the Cardiac Newborn Neurodevelopmental Network SIG of the Cardiac Neurodevelopmental Outcomes Collaborative, who planted the seed of the idea and assisted with dissemination of information and coordinating between participating hospitals.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/skin-to-skin-group-photo-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-05-15 16:34:092026-03-02 09:21:02Children’s National co-leads efforts to increase skin-to-skin care for babies with congenital heart disease
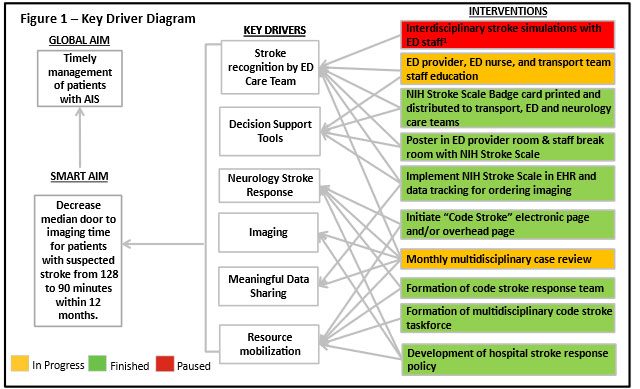
1 – Interdisciplinary stroke simulations were canceled due to short staffing and insufficient nursing support during COVID-19 pandemic.
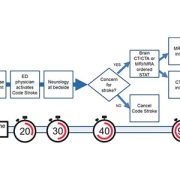
Diagnosis times improved for pediatric arterial ischemic stroke (AIS) patients in the emergency department after the implementation of a quality improvement initiative. According to a new study, published in Pediatrics, the median door-to-imaging time for children with suspected AIS improved from 128 minutes to 68 minutes post-intervention.
What it means
Pediatric AIS is an important cause of morbidity and mortality that requires early recognition to benefit from hyperacute therapies. A quality improvement study at Children’s National Hospital aimed to improve timely diagnosis of AIS through an interdisciplinary stroke response protocol. The researchers implemented a quality improvement initiative from November 2019 to June 2023 in the emergency department that included interventions under two categories – workflow efficiency improvement and staff education. A total of 71 patients who met the criteria for the study were analyzed. Median door-to-imaging time for all patients improved from 128 minutes during the baseline period to 68 minutes.
The researchers note that establishing a well-functioning stroke response protocol is a critical step in detecting pediatric stroke in the community and expediting care for this vulnerable patient population.
“This study highlights the value of quality improvement methodologies in coordinating multiple hospital divisions for the greater goal of improving patient care,” says Theodore Trigylidas, MD, corresponding author and emergency medicine physician at Children’s National. “We hope it serves as a template for other healthcare organizations in developing their own pediatric stroke protocols.”
Code Stroke management algorithm. CT/CTA, computed tomography with or without angiography. MRI/MRA, magnetic resonance imaging with or without angiography.
The hold up in the field
The rarity of AIS in pediatric patients and stroke mimics, like hemiplegic migraine, may cause challenges for a timely diagnosis, and treatments for AIS – thrombolysis and thrombectomy – must be performed within specific time frames.
Moving the field forward
“By taking into consideration local staffing structures and institutional resource availability, the quality improvement approach described here can serve as a framework for how institutions might implement a pediatric acute stroke response protocol given their own unique systems of care and resource considerations,” says Dana Harrar, MD, PhD, study author and director, Pediatric Stroke Program at Children’s National.
The authors plan to expand this initiative to incorporate children at outside facilities with the goal of creating a stroke network with nearby hospitals.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/Code-Stroke-management-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-05-02 09:05:042025-05-02 09:08:20Stroke alert teams beneficial to timely diagnosis of pediatric stroke patients
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-04-22 10:31:052026-04-13 10:39:42REI Week 2025 empowers the future in pediatric research and innovation















 A new $8 million investment from the Gilbert Family Foundation will support groundbreaking research on neurofibromatosis type 1 (NF1) at Children’s National Hospital. The generous five-year grant continues the Foundation’s longstanding research partnership with the hospital. It will accelerate investigations aimed at improving the lives of children and young adults affected by this genetic condition.
A new $8 million investment from the Gilbert Family Foundation will support groundbreaking research on neurofibromatosis type 1 (NF1) at Children’s National Hospital. The generous five-year grant continues the Foundation’s longstanding research partnership with the hospital. It will accelerate investigations aimed at improving the lives of children and young adults affected by this genetic condition.
 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
 Physicians, fellows and faculty from the
Physicians, fellows and faculty from the