Reflective of the myriad symptoms and complications that can accompany hydrocephalus, a multidisciplinary team at Children’s National works with patients and families for much of childhood.
The Doppler image on the oversized computer screen shows the path taken by blood as it flows through the newborn’s brain, with bright blue distinguishing blood moving through the middle cerebral artery toward the frontal lobe and bright red depicting blood coursing away. Pitch black zones indicate ventricles, cavities through which cerebrospinal fluid usually flows and where hydrocephalus can get its start.
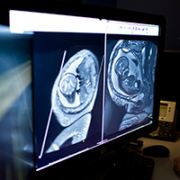
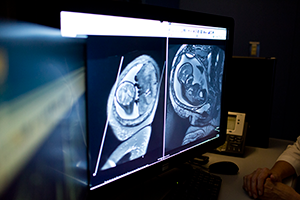
The buildup of excess cerebrospinal fluid in the brain can begin in the womb and can be detected by fetal magnetic resonance imaging. Hydrocephalus also can crop up after birth due to trauma to the head, an infection, a brain tumor or bleeding in the brain, according to the National Institutes of Health. An estimated 1 to 2 per 1,000 newborns have hydrocephalus at birth.
When parents learn of the hydrocephalus diagnosis, their first question tends to be “Is my child going to be OK?” says Suresh Magge, M.D., a pediatric neurosurgeon at Children’s National Health System.
“We have a number of ways to treat hydrocephalus. It is one of the most common conditions that pediatric neurosurgeons treat,” Dr. Magge adds.
Unlike fluid build-up elsewhere in the body where there are escape routes, with hydrocephalus spinal fluid becomes trapped in the brain. To remove it, surgeons typically implant a flexible tube called a shunt that drains excess fluid into the abdomen, an interim stop before it is flushed away. Another surgical technique, called an endoscopic third ventriculostomy has the ability to drain excess fluid without inserting a shunt, but it only works for select types of hydrocephalus, Dr. Magge adds.
For the third year, Dr. Magge is helping to organize the Hydrocephalus Education Day on Feb. 25, a free event that offers parents an opportunity to learn more about the condition.
Reflective of the myriad symptoms and complications that can accompany hydrocephalus, such as epilepsy, cerebral palsy, cortical vision impairment and global delays, a multidisciplinary team at Children’s National works with patients and families for much of childhood.
Neuropsychologist Yael Granader, Ph.D., works with children ages 4 and older who have a variety of developmental and medical conditions. Granader is most likely to see children and adolescents with hydrocephalus once they become medically stable in order to assist in devising a plan for school support services and therapeutic interventions. Her assessments can last an entire day as she administers a variety of tasks that evaluate how the child thinks and learns, such as discerning patterns, assembling puzzles, defining words, and listening to and remembering information.
Neuropsychologists work with schools in order to help create the most successful academic environment for the child. For example, some children may struggle to visually track across a page accurately while reading; providing a bookmark to follow beneath the line is a helpful and simple accommodation to put in place. Support for physical limitations also are discussed with schools in order to incorporate adaptive physical education or to allow use of an elevator in school.
“Every child affected by hydrocephalus is so different. Every parent should know that their child can learn,” Granader says. “We’re going to find the best, most supportive environment for them. We are with them on their journey and, every few years, things will change. We want to be there to help with emerging concerns.”
Another team member, Justin Burton, M.D., a pediatric rehabilitation specialist, says rehabilitation medicine’s “piece of the puzzle is doing whatever I can to help the kids function better.” That means dressing, going to the bathroom, eating and walking independently. With babies who have stiff, tight muscles, that can mean helping them through stretches, braces and medicine management to move muscles smoothly in just the way their growing bodies want. Personalized care plans for toddlers can include maintaining a regular sleep-wake cycle, increasing attention span and strengthening such developmental skills as walking, running and climbing stairs. For kids 5 and older, the focus shifts more to academic readiness, since those youths’ “full-time job” is to become great students, Dr. Burton says.
The area of the hospital where children work on rehabilitation is an explosion of color and sounds, including oversized balance balls of varying dimensions in bright primary colors, portable basketball hoops with flexible rims at multiple heights, a set of foam stairs, parallel bars, a climbing device that looks like the entry to playground monkey bars and a chatterbox toy that lets a patient know when she has opened and closed the toy’s doors correctly.
“We end up taking care of these kids for years and years,” he adds. “I always love seeing the kids get back to walking and talking and getting back to school. If we can get them back out in the world and they’re doing things just like every other kid, that’s success.”
Meanwhile, Dr. Magge says research continues to expand the range of interventions and to improve outcomes for patients with hydrocephalus, including:
Unlike spina bifida, which sometimes can be corrected in utero at some health institutions, hydrocephalus cannot be corrected in the womb. “While we have come a long way in treating hydrocephalus, there is still a lot of work to be done. We continue to learn more about hydrocephalus with the aim of continually improving treatments,” Dr. Magge says.
During a recent office visit, 5-year-old Abagail’s head circumference had measured ¼ centimeter of growth, an encouraging trend, Robert Keating, M.D., Children’s Chief of Neurosurgery, tells the girl’s mother, Melissa J. Kopolow McCall. According to Kopolow McCall, who co-chairs the Hydrocephalus Association DC Community Network, it is “hugely” important that Children’s National infuses its clinical care with the latest research insights. “I have to have hope that she is not going to be facing a lifetime of brain surgery, and the research is what gives me the hope.”