Five Children’s National Hospital faculty named to Society for Pediatric Research

The Society for Pediatric Research (SPR) announced five new members from Children’s National Hospital: Drs. Rana Hamdy, Panagiotis Kratimenos, Brynn Marks, Shayna Coburn and Katie Donnelly.
The Society for Pediatric Research (SPR) announced five new members from Children’s National Hospital. Established in 1929, SPR’s mission is to create a multi-disciplinary network of diverse researchers to improve child health.
Membership in SPR is a recognized honor in academic pediatrics. It requires nomination by academic peers and leaders as well as recognition of one’s role as an independent, productive child health researcher.
“I am so proud of our faculty and all that they have accomplished. I am thrilled that they have been recognized for their achievements,” said Beth A. Tarini, M.D., M.S., SPR president and associate director for the Center for Translational Research at Children’s National Hospital.
SPR 2021 active new members from Children’s National are:
-
- Katie Donnelly, M.D., M.P.H., attending physician in the Emergency Department at Children’s National Hospital. She is the medical director for Safe Kids DC, an organization dedicated to preventing accidental injuries in children in Washington DC. Her personal research interest is in preventing firearm injuries in children and she is a member of Safer through Advocacy, Firearm Education and Research (SAFER), a multidisciplinary team dedicated to firearm injury prevention at Children’s National. She is also the medical director of the newly founded hospital-based violence intervention program at Children’s National and an associate professor of pediatrics and emergency medicine at The George Washington University.“To be recognized by my peers as a researcher with a significant contribution to our field is very validating. It also opens a world of potential collaborations with excellent scientists, which is very exciting!” said Dr. Donnelly. “I am grateful for the immense support offered to me by the Division of Emergency Medicine to complete the research I am passionate about, especially my mentor Monika Goyal.”
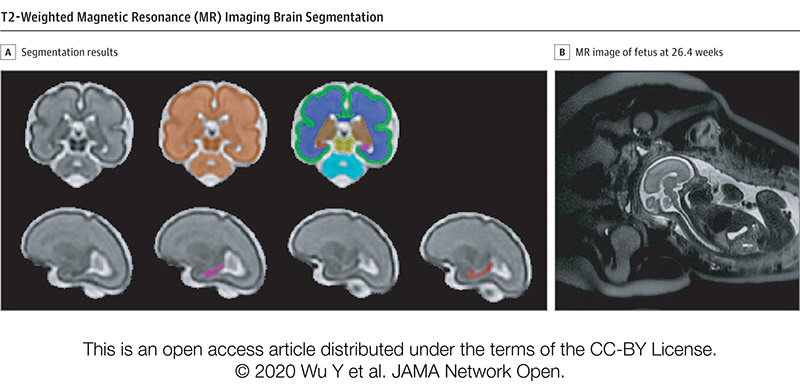
- Panagiotis Kratimenos, M.D., Ph.D., newborn intensivist and neuroscientist at Children’s National. He studies mechanisms of brain injury in the neonate, intending to prevent its sequelae later in life. Dr. Kratimenos’ interest lies in identifying therapies to prevent or improve neurodevelopmental disabilities of sick newborns caused by prematurity and perinatal insults.“Being a member of SPR is a deep honor for me. SPR has always been a ‘mentorship home’ for me since I was a trainee and a member of the SPR junior section,” said Dr. Kratimenos. “A membership in the SPR allows us to access a very diverse, outstanding team of pediatric academicians and researchers who support the development of physician-scientists, honors excellence through prestigious grants and awards, and advocates for children at any level either locally, nationally, or internationally.”
- Rana Hamdy, M.D., M.P.H., M.S.C.E., pediatric infectious diseases physician at Children’s National and Director of the Antimicrobial Stewardship Program. She is an assistant professor of pediatrics at George Washington University School of Medicine and Health Sciences. Her area of expertise focuses on the prevention and treatment of antimicrobial resistant infections and the promotion of good antimicrobial stewardship in inpatient and outpatient settings.“It’s an honor to be joining the Society for Pediatric Research and becoming part of this distinguished multidisciplinary network of pediatric researchers,” said Dr. Hamdy. “I look forward to the opportunity to meet and work with SPR members, make connections for future collaborations, as well as encourage trainees to pursue pediatric research through the opportunities that SPR offers.”
- Shayna Coburn, Ph.D., director of Psychosocial Services in the Celiac Disease Program at Children’s National. She is a licensed psychologist specializing in coping and interpersonal relationships in chronic illness treatment, particularly for conditions involving specialized diets. She holds an appointment as assistant professor of psychiatry and behavioral sciences at The George Washington University School of Medicine and Health Sciences. Her work has focused on promoting effective doctor-patient communication, reducing healthcare disparities and supporting successful adherence across the developmental span of childhood and adolescence. She currently has a Career Development Award from National Institute of Diabetes and Digestive and Kidney Diseases to refine and test a group intervention designed to improve self-management and quality of life in teens with celiac disease.
“I hope that my background as a psychologist researcher will help diversify SPR. As an SPR member, I hope to encourage more opportunities for training, awards, and other programs that would be inclusive of clinician researchers who may not hold a traditional medical degree,” said Dr. Coburn. - Brynn Marks, M.D., M.S.-H.P.Ed., endocrinologist at Children’s National. As a clinical and translational scientist her goal is to use unique personal experiences and training to optimize both patient and provider knowledge of and behaviors surrounding diabetes technologies thereby realizing the potential of diabetes technologies improve the lives and clinical outcomes of all people living with diabetes. Her experiences as a person living with Type 1 diabetes have undoubtedly shaped her clinical and research interests in diabetes management and medical education.
“It is an honor to be accepted for membership in the Society for Pediatric Research,” said Dr. Marks. “Being nominated and recognized by peers in this interprofessional pediatric research community will allow me networking and growth opportunities as I continue to advance my research career.”