“It is a market failure that we are dealing with – a lack of incentives leading to a stagnation in innovation with respect to small markets, such as pediatrics. Children’s National Hospital and our partners in other children’s hospitals in the country play a critical role in making noise and sending a message that children should not be an afterthought.”
Hear more from Kolaleh Eskandanian, Ph.D., M.B.A., during her recent appearance at POLITICO. As vice president and chief innovation officer at Children’s National and Alliance for Pediatric Device Innovation principal investigator, Dr. Eskandanian shared her approach to engaging with the Food and Drug Administration (FDA) to advance artificial intelligence (AI) and machine learning technologies for pediatric healthcare. To date, she noted, the FDA has authorized 950 healthcare-related technologies enabled with AI and machine learning.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/10/Politico-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-10-01 11:11:532025-03-10 13:30:17In the news: The future of patient care and access
The future of healthcare is unfolding before scientists and clinicians: Doctors are assisted by virtual scribes trained by artificial intelligence. Algorithms are reading MRIs. Smartphones are helping to detect strep throat. Machines diagnose children without access to care.
These and dozens of other artificial intelligence (AI) applications are being tested to enhance pediatric healthcare, and many were on display at the 2nd annual Children’s National Hospital-Virginia Tech Symposium on AI for Pediatric Health at the Children’s National Research & Innovation Campus.
Some highlights from the daylong conversation about the future of pediatric medicine, augmented by AI and generative AI models capable of producing new and critical content:
Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation: “Children are just not mini-adults. In pediatric care, we train pediatric specialists because kids die from different diseases than those that kill adults. Children also suffer from very impactful and rare conditions. If we train pediatric specialists well, we have to train AI algorithms in the same fashion.”
Rowland Illing, M.D., Ph.D., chief medical officer and director of global healthcare and nonprofits at Amazon Web Services: “In a short period of time, the complexity of the models available is astounding. Generative AI, just like AI, can impact outcomes at every step of the patient pathway, including the clinical workflow, care management and patient engagement. By creating a specific use case with generative AI, every step can be optimized to be smarter, which ultimately leads to improved patient care and outcomes.”
Children’s National Chief Academic Officer Nathan Kuppermann, M.D., M.P.H.: “AI in pediatric health is not just about identifying rare diseases. Its potential includes all aspects of clinical care, clinical operations, education and research. It has the potential to help educators enhance the novelty and impact of their methods and advance research with powerful tools to gather and analyze data.”
Alda Mizaku, vice president and chief data and artificial intelligence officer at Children’s National: “What excites me most about our future is the endless possibilities. We can use AI and data to uncover many things: rare diseases, operational efficiencies, time-saving and cost-saving solutions. This has to be done in a responsible way, and we must look at what some of the guardrails need to be.”
Throughout the day, expert panels offered insights into regulatory pathways to deploy AI in pediatric drugs and devices. The Food and Drug Administration’s Office of Science and Engineering Laboratories also provided guidance on collaborative tools for improving the representation of children and perinatal patients in AI-powered medical devices.
Moving the field forward
Early adopters of AI at Children’s National shared applications already under investigation, including efforts to segment and measure brain tumors on imaging, weigh the risk of strep throat with a smartphone camera and detect rheumatic heart disease with portable technology and an algorithm.
Dr. Linguraru, an expert in healthcare AI, said that artificial intelligence is no longer a hypothetical technology but is already remaking the healthcare system. “AI is here. What matters now is how we use it and how we train doctors to use it well,” he said.
The big picture
Through growing partnerships, Children’s National experts are teaming up with researchers at Virginia Tech on a series of AI-driven projects aimed at advancing pediatric health, including programs to rethink privacy in federated learning, forecast emergency department surges, extract clinical variables from documents to predict sepsis risks, identify rare genetic syndromes in children, and predict single-cell responses to genetic perturbations in pediatric developmental disorders.
Naren Ramakrishnan, Ph.D., director of the Sanghani Center at Virginia Tech and the Thomas L. Phillips Professor in the College of Engineering, said the partnership between the two academic centers is changing healthcare already and will continue to as the organizations offer future seed grants to support innovation in cardiology, neuroscience and oncology. “The roots have borne fruit,” he said.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/09/AI-symposium-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-09-24 11:38:032024-09-24 11:40:33Transforming pediatric care: How AI is driving the next medical revolution
Cheng-Chia “Fred” Wu, M.D., Ph.D., joins the team at the campus as an assistant professor at Virginia Tech’s Fralin Biomedical Research Institute. Image credit: Fralin Biomedical Research Institute.
Experience, talent and technology are coming together at the Children’s National Research & Innovation Campus to solve the complex challenges of treating pediatric brain tumors through a growing partnership between Children’s National Hospital and Virginia Tech.
Cheng-Chia “Fred” Wu, M.D., Ph.D., joins the team at the campus as an assistant professor at Virginia Tech’s Fralin Biomedical Research Institute. He hopes to improve treatment for pediatric brain tumors and other cancers by leveraging technological advances in focused ultrasound and studying how this modality can be combined with other novel therapies. Children’s National physicians and scientists are collaborating with Virginia Tech scientists to develop these new approaches.
Why we’re excited
Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research and interim chief academic officer at Children’s National, said collaborations — including the partnership between Children’s National and Virginia Tech — are essential to solving formidable scientific challenges.
“We are thrilled to be working with Dr. Wu to develop cutting-edge therapeutics for pediatric brain tumors,” Dr. Bollard said. “With Dr. Wu’s experience and the talents of our team at Children’s National, I have great hope that we will be able to combine our novel technologies and therapies to provide tremendous breakthroughs for treating pediatric patients with brain tumors.”
Before joining Virginia Tech, Dr. Wu was an assistant professor of radiation oncology at Columbia University Irving Medical Center in New York, where he treated pediatric cancers and central nervous system malignancies.
“Partnering with Children’s National connects us to a world-class clinical trial institute that has been a pioneer in treating brain tumors with focused ultrasound technology, and this presents a unique opportunity to help children and families struggling with cancer,” Dr. Wu said. “I can’t wait to see where this takes us.”
Dr. Wu played a key role in the Initiative for Drug Delivery Innovation for Childhood Brain Tumors at Columbia, developing a bench-to-bedside platform to facilitate the translation of promising technologies for targeted drug delivery in children with brain tumors.
Within three years, the team demonstrated the safety and feasibility of using focused ultrasound in the brainstem and adding radiation in preclinical models. They then opened two clinical trials for kids with relapsed diffuse midline glioma, an aggressive and difficult-to-treat brain tumor that occurs in the brain stem, thalamus and spinal cord.
What’s ahead
Dr. Wu will be involved in a wide range of research touching both organizations, including veterinary medicine and biomedical engineering at Virginia Tech.
Michael Friedlander, Ph.D., executive director of the Fralin Biomedical Research Institute at Virginia Tech Carilion and vice president for health sciences and technology at Virginia Tech, welcomed Dr. Wu’s experience as a pediatric radiation oncologist, translational physician-scientist and clinical trialist who has led an innovative drug delivery program.
“He is armed with a unique set of skills to identify promising new technology and implement it in areas of great need for treatment of pediatric cancers,” Dr. Friedlander said. “We are absolutely delighted to have Dr. Wu as part of the team. He represents a powerful new part of the strong partnership between Virginia Tech and Children’s National Hospital for addressing pediatric brain cancer.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/08/Doctor-Wu-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-08-22 12:03:472024-08-22 12:04:52Expanding team innovates to take on pediatric brain tumors
The adoption of artificial intelligence (AI) has the potential to enhance radiological imaging, improve diagnostic capabilities and reduce burnout in the field.
The adoption of artificial intelligence (AI) has the potential to enhance radiological imaging, improve diagnostic capabilities and reduce burnout in the field, provided that physicians and scientists work together to ensure its careful integration into the practice of medicine, according to a special report in Radiology: Artificial Intelligence, a journal of the Radiological Society of North America (RSNA).
Assembled by experts in radiology, medical imaging and machine learning, the special report lays out the clinical, cultural, computation and regulatory considerations that are being introduced, particularly as generative AI models become part of the field.
“AI tools can play a key role in radiology, but radiologists must be able to trust in the systems’ design and receive adequate training. As the physicians most familiar with these tools, radiologists should establish clear guidelines regarding clinical accountability,” said Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation.
Moving the field forward
Dr. Linguraru and his peers assembled the report based on a series of seminars hosted by RSNA and the Medical Image Computing and Computer Assisted Intervention (MICCAI) Society. They collected input from multidisciplinary experts to outline the current clinical uses of AI and its future potential.
The experts agreed that collaboration between radiologists and AI scientists will be essential to successfully integrate AI into the discipline of radiology. This partnership should focus on establishing a unified agenda, shared language and clear expectations of the tools developed. By working together, they can ensure that AI tools are designed and implemented to meet the practical needs of radiology, particularly with the incorporation of language and vision models.
What’s next
Among the challenges ahead, clinical institutions must align their staffing, data management and computational resources to deploy and monitor AI systems effectively. This alignment includes ensuring that personnel are adequately trained to use AI tools, that data is managed and processed efficiently and that sufficient computational power is available to support AI operations. Cloud computing may be vital to hospitals that don’t have hardware and technical maintenance resources.
“The successful integration of AI in radiology depends on trust in AI design, collaborative efforts between radiologists and AI scientists, and the alignment of clinical resources to support AI deployment,” Dr. Linguraru said. “With these factors in place, AI can play a transformative role in improving radiological practices and outcomes.”
The research from Children’s National Hospital provides mounting evidence that children of the pandemic, even those far too young to understand it, need ongoing assessments of developmental or mental health support later in life.
A critical part of the brain linked to risks for anxiety later in life – the left amygdala – was significantly smaller by volume in babies of mothers who reported stress during the COVID-19 pandemic, according to a new manuscript published in JAMA Network Open.
The right hippocampus, which governs spatial, visual and verbal memories, and the white matter were also reduced in children whose mothers reported stress.
The research from Children’s National Hospital provides mounting evidence that children of the pandemic, even those far too young to understand it, need ongoing assessments of developmental or mental health support later in life.
“Looking ahead, we want to use this information – and studies with similar findings – to empower pregnant mothers to request support to mitigate their stress, especially in the event of another global health crisis,” said Nickie Andescavage, M.D., a neonatologist and principal investigator at the Center for Prenatal, Neonatal & Maternal Health Research. “We also want to make sure babies born during COVID-19 get the services that they need in life if they develop anxiety or other mental health disorders.”
The fine print
Researchers at the center used magnetic resonance imaging (MRI) to compare the brains of 103 babies born between 2014 and 2019 prior to the pandemic to 59 born between 2020 and 2022. Mothers who had COVID-19 or other complications in their pregnancies were excluded. The babies underwent MRI imaging while in utero and again soon after delivery.
The mothers were evaluated for stress and anxiety, using the Spielberger State-Train Anxiety Inventory and other evidence-based scoring measures. Pre-pandemic, 21% of mothers reported elevated symptoms of anxiety; in the pandemic cohort, that number jumped to nearly 62%.
Their babies’ brains were also changed, as regions widely understood to control emotion and anxiety displayed smaller volumes on MRI imaging. Given the global impact of the pandemic and universal reports of mental distress worldwide, the potential impact of these findings may impact an entire generation of children born during the pandemic. The team is just beginning to unravel the medical significance.
What’s next
Catherine Limperopoulos, Ph.D., director of the Center for Prenatal, Neonatal & Maternal Health Research, said understanding the impact of stress is vital in supporting the healthy development of young children. Current studies are underway at her center to tease apart the role of stress in prenatal development and examine its long-term impact on development, including cognition, behavior and mental health.
“We all know that being pregnant can be quite stressful, and there are certain times of collective stress that can provide us windows to understand how the body and mind manage it,” Dr. Limperopoulos said. “At our center, we care deeply about the health of mothers and babies, and our researchers plan to continue investigating the role of stress in development to continue building data to show that mental health must be a greater priority.”
This study – “Prenatal maternal psychological distress during the COVID-19 pandemic and newborn brain development” – was supported by the National Institutes of Health, the Intellectual and Developmental Disabilities Research Center, and the A. James & Alice B. Clark Foundation. You can read the full study in JAMA Network Open.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/06/pregnant-woman-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-06-20 14:17:032024-06-20 15:02:32Pandemic stress in pregnant mothers may affect anxiety regions of babies’ brains
In the complex world of pediatric diseases, researchers need access to data to develop clinical trials and the participation of vulnerable patients to develop new devices and therapies. Both are in short supply, given that most children are born healthy, and most severe pediatric diseases are rare.
That creates a dilemma: how do researchers build a foundation to advance new treatments? Enter artificial intelligence (AI).
“AI is the equalizer: accelerated intelligence for sick kids. No other advance on the horizon holds more promise for improving equity and access to pediatric healthcare when diseases are rare and resources are limited,” says Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). “AI will shrink the distance between patient and provider, allowing our physicians and scientists to provide targeted healthcare for children more efficiently. The possibilities are endless.”
Why we’re excited
By pioneering AI innovation programs at Children’s National Hospital, Dr. Linguraru and the AI experts he leads are ensuring patients and families benefit from a coming wave of technological advances. The team is teaching AI to interpret complex data that could otherwise overwhelm clinicians. Their work will create systems to identify at-risk patients, forecast disease and treatment patterns, and support complex clinical decisions to optimize patient care and hospital resources. Already, the AI team at SZI has developed data-driven tools touching nearly every corner of the hospital:
AI for rheumatic heart disease (RHD): In partnership with Children’s National cardiology leaders, including Craig Sable, M.D., the Uganda Heart Institute and Cincinnati Children’s Hospital, the AI team has developed an algorithm that can use low-cost, portable ultrasound imaging to detect RHD in children and young adults, a disease that takes nearly 400,000 lives annually in limited-resource countries. Early testing shows the AI platform has the same accuracy as a cardiologist in detecting RHD, paving the way for earlier treatment with life-saving antibiotics. This year, Children’s National physicians will be in Uganda, screening 200,000 children with local cardiology experts and AI technology.
Newborn screening for genetic conditions with mGene: Working with Rare Disease Institute clinicians and Chief of Genetics and Metabolism Debra Regier, M.D., the AI team has built technology to detect rare genetic disorders, using an algorithm and a smartphone camera to identify subtle changes in facial features. Tested on patients from over 30 countries and published in The Lancet Digital Health, the application helps screen children for advanced care when a geneticist may not be within reach. With funding from the National Institutes of Health, Children’s National and its research partners are piloting a newborn screening program in the Democratic Republic of the Congo.
Pediatric brain tumors: To improve and personalize the treatment decisions for children with brain tumors, Dr. Linguraru’s team is working with Brain Tumor Institute Director Roger Packer, M.D., the Gilbert Family Distinguished Professor of Neurofibromatosis, on algorithms that can characterize and measure brain tumors with unprecedented precision. The team recently won the International Pediatric Brain Tumor Segmentation Challenge, distinguishing the Children’s National algorithm as among the best in the world.
Ultra-low field magnetic resonance imaging (MRI): With a grant from the Bill & Melinda Gates Foundation, the AI team is working alongside Children’s Hospital Los Angeles, King’s College London and the UNITY Consortium to expand global brain imaging capacity. The consortium is helping clinicians in limited-resource countries improve the treatment of neonatal neurological conditions, using AI to boost the quality of ultra-low field MRI and expand access to this portable and more affordable imaging option.
Federated learning: Children’s National has collaborated with NVIDIA and other industry leaders to accelerate AI advances through federated learning. Under this approach, institutions share AI models rather than data, allowing them to collaborate without exposing patient information or being constrained by essential data-sharing restrictions. The SZI team was the only pediatric partner invited to join the largest federated learning project of its kind, studying the lungs of COVID-19 patients. Details were published in Nature Medicine.
Children’s National leads the way
Looking ahead, the Children’s National AI team is pursuing a wide range of advances in clinical care. To support patients treated at multiple clinics, they are developing systems to harmonize images from different scanners and protocols, such as MRI machines made by different manufacturers. Similar work is underway to analyze pathology samples from different institutions consistently.
Automation is also making care more efficient. For example, using data from 1 million chest X-rays, the team is collaborating with NVIDIA to develop a conversational digital assistant that will allow physicians to think through 14 possible diagnoses.
Dr. Linguraru says he and his colleagues are galvanized by the jarring statistic that one in three children with a rare disease dies before age 5. While well-implemented AI initiatives can change outcomes, he says the work must be done thoughtfully.
“In the future, patients will be evaluated by human clinicians and machines with extraordinary powers to diagnose illness and determine treatments,” Dr. Linguraru said. “Our team at Children’s National is leading conversations about the future of pediatric healthcare with a focus on safety, resource allocation and basic equity.”
Learn more about our AI initiatives
Innovation leaders at Children’s National Hospital are building a community of AI caregivers through educational and community-building events. At the inaugural Symposium on Artificial Intelligence in 2023 at the Children’s National Research & Innovation Campus, experts from Virginia Tech, JLABS, Food and Drug Administration, Pfizer, Oracle Health, NVIDIA, AWS Health and elsewhere laid out a vision for using data to advance pediatric medicine. The symposium will return on Sept. 6.
Dr. Linguraru is the program chair of MICCAI 2024, the top international meeting on medical image computing and computer-assisted intervention and the preeminent forum for disseminating AI developments in healthcare. The conference is an educational platform for scientists and clinicians dedicated to AI in medical imaging, with a focus on global health equity. It will take place for the first time in Africa on Oct. 6-10.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/04/Marius-AI-lecture-CNRI.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-04-24 09:20:052025-10-29 16:12:15Artificial – and accelerated – intelligence: endless applications to expand health equity
Winners and finalists competed at UCLA during annual L.A. MedTech Week 2024. Left to right are: Nada Hanafi, MedTech Color Board treasurer; Vernessa Pollard, MedTech Color Board secretary; Dr. Sanna Gaspard, CEO and founder of Rubitection, (winner -$35,000 first prize); Dr. Kolaleh Eskandanian, Children’s National vice president and chief innovation officer; Kwame Ulmer, MedTech Color founder and board chair. Photo credit: MedTech Color
Alliance for Pediatric Device Innovation (APDI), a federally funded consortium led by Children’s National Hospital, and member MedTech Color announced the winners of the recent edition of the Make Your Medical Device Pitch for Kids!™ competition, which focused on recognizing and supporting African American and Hispanic pediatric medical device innovators. The awardees received a combined $50,000 in grant funding from APDI, made possible by the U.S. Food and Drug Administration (FDA) to support the advancement of pediatric medical technologies to the market.
The winners were selected from a field of five finalists who gave pitch presentations on their innovation’s attributes, benefits to patients and pathway to commercialization before a panel of five expert judges. The event was held on March 15 at the University of California, Los Angeles, as part of the annual MedTech Color Pitch Competition during L.A. MedTech Week 2024, powered by BioscienceLA.
The award-winning pediatric devices and companies are:
Rubitection, Pittsburgh, Pa.– A low-cost skin assessment management tool for chronic wounds, Rubitection measures the properties of the skin. The system allows the user to monitor incremental changes in skin health to predict risk, monitor progression and customize care.
Kofimi Technology Inc., Danvers, Mass. – This patent-pending pulse oximeter device is designed specifically for pediatric populations to provide superior accuracy for all levels of skin pigmentation. A pulse oximeter measures oxygen levels in the blood.
Why we’re excited
“Funding innovators of African American and Hispanic backgrounds is crucial for advancing diversity, equity, and inclusion initiatives because it addresses systemic barriers and inequities that have historically hindered this group from accessing resources and opportunities in the life sciences sector,” said Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer at Children’s National and APDI program director and principal investigator. “Supporting a diverse group of innovators enriches the research and development process by bringing a variety of perspectives and viewpoints representing all populations.”
Along with the grant award, all finalists receive access to a network of supportive resources and expertise as part of their connection to APDI and MedTech Color.
Along with the pitch presentations, the event program included a keynote talk from Tonya Kinlow, vice president of Community Engagement, Advocacy and Government Affairs at Children’s National, highlighting advocacy initiatives leading to an all-inclusive system of care for children.
Children’s National leads the way
Julia Finkel, M.D., pediatric anesthesiologist at Children’s National and principal investigator for APDI, participated in the panel discussion “Inequity within Inequity,” which highlighted how racial disparities in pediatric healthcare remain a critical challenge across the United States. APDI’s goal is to advance pediatric devices that meet patient needs while promoting a more inclusive approach to discovering and supporting talented innovators.
“We believe there is a community of companies focused on platforms that treat or diagnose pediatrics,” said Kwame Ulmer, founder of MedTech Color. “This partnership allows us to significantly increase the support we provide for entrepreneurs in this area. We are delighted to be a part of the Children’s National community to drive positive patient outcomes.”
The patient benefit
Founded in 2017, MedTech Color is a nonprofit organization built on the same ideal: diverse leadership in the medical technology ecosystem leads to greater innovation and better outcomes. The organization works to advance the representation of people of color in the medical device industry and to nurture the next generation of founders. For more information on MedTech Color, visit medtechcolor.org.
APDI is one of five nonprofit consortia in the FDA’s Pediatric Device Consortia program that receives funding to provide a platform of services, expertise and grants to support pediatric innovators in bringing medical devices to the market that address the needs of children. Along with Children’s National, APDI members include Johns Hopkins University, CIMIT at Mass General Brigham, Tufts Medical Center, Medstar Health Research Institute, OrthoPediatrics Corp. and MedTech Color.
Advancements in pediatric medical devices continue to lag significantly behind those of adults, which is why APDI is focused on helping more pediatric medical device innovations achieve commercialization. For more information on APDI, visit innovate4kids.org
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/03/1st-Place-Peds-Rubitection-CNRI.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-03-21 13:07:012025-03-10 13:59:53Two pediatric medical device companies awarded at pitch competition
Catherine Limperopoulos, Ph.D., was drawn to understanding the developing brain, examining how early adverse environments for a mother can impact the baby at birth and extend throughout its entire lifetime. She has widened her lens – and expanded her team – to create the new Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital.
“Despite the obvious connection between mothers and babies, we know that conventional medicine often addresses the two beings separately. We want to change that,” said Dr. Limperopoulos, who also directs the Developing Brain Institute. “Given the current trajectory of medicine toward precision care and advanced imaging, we thought this was the right moment to channel our talent and resources into understanding this delicate and highly dynamic relationship.”
Moving the field forward
Since its establishment in July 2023, the new research center has gained recognition through high-impact scientific publications, featuring noteworthy studies exploring the early phases of human development.
Dr. Limperopoulos has been at the forefront of groundbreaking research, directing attention to the consequences of maternal stress on the unborn baby and the placenta. In addition, under the guidance of Kevin Cook, Ph.D., investigators published a pivotal study on the correlation between pain experienced by premature infants in the Neonatal Intensive Care Unit and the associated risks of autism and developmental delays.
Another area of research has focused on understanding the impact of congenital heart disease (CHD) on prenatal brain development, given the altered blood flow to the brain caused by these conditions during this period of rapid development. Led by Josepheen De Asis-Cruz, M.D., Ph.D., a research team uncovered variations in the functional connectivity of the brains of infants with CHD. In parallel, Nickie Andescavage, M.D., and her team employed advanced imaging techniques to identify potential biomarkers in infants with CHD, holding promise for guiding improved diagnostics and postnatal care. Separately, she is investigating the impact of COVID-19 on fetal brain development.
In the months ahead, the team plans to concentrate its efforts on these areas and several others, including the impact of infectious disease, social determinants of health and protecting developing brains from the negative impacts of maternal stress, pre-eclampsia and other conditions prevalent among expectant mothers.
Assembling a team
Given its robust research plan and opportunities for collaboration, the center pulled together expertise from across the hospital’s faculty and has attracted new talent from across the country, including several prominent faculty members:
Katherine L. Wisner, M.S., M.D., has accumulated extensive knowledge on the impact of maternal stress on babies throughout her career, and her deep background in psychiatry made her a natural addition to the center. While Dr. Wisner conducts research into the urgent need to prioritize maternal mental health, she will also be treating mothers as part of the DC Mother-Baby Wellness Initiative — a novel program based at Children’s National that allows mothers to more seamlessly get care for themselves and participate in mother-infant play groups timed to align with their clinical appointments.
Catherine J. Stoodley, B.S., M.S., D.Phil., brings extensive research into the role of the cerebellum in cognitive development. Dr. Stoodley uses clinical studies, neuroimaging, neuromodulation and behavioral testing to investigate the functional anatomy of the part of the brain responsible for cognition.
Katherine M. Ottolini, M.D., attending neonatologist, is developing NICU THRIVE – a research program studying the effects of tailored nutrition on the developing newborn brain, including the impact of fortifying human milk with protein, fat and carbohydrates. With a grant from the Gerber Foundation, Dr. Ottolini is working to understand how personalized fortification for high-risk babies could help them grow.
Early accolades
The new center brings together award-winning talent. This includes Yao Wu, Ph.D., who recently earned the American Heart Association’s Outstanding Research in Pediatric Cardiology award for her groundbreaking work in CHD, particularly for her research on the role of altered placental function and neurodevelopmental outcomes in toddlers with CHD. Dr. Wu became the third Children’s National faculty member to earn the distinction, joining an honor roll that includes Dr. Limperopoulos and David Wessel, M.D., executive vice president and chief medical officer.
Interim Chief Academic Officer Catherine Bollard, M.D., M.B.Ch.B., said the cross-disciplinary collaboration now underway at the new center has the potential to make a dramatic impact on the field of neonatology and early child development. “This group epitomizes the Team Science approach that we work tirelessly to foster at Children’s National,” Dr. Bollard said. “Given their energetic start, we know these scientists and physicians are poised to tackle some of the toughest questions in maternal-fetal medicine and beyond, which will improve outcomes for our most fragile patients.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/Newborn-baby-CNRI.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-02-29 11:07:062026-04-15 16:20:40Pioneering research center aims to revolutionize prenatal and neonatal health
Children’s National experts pioneered a novel approach of inducing strokes to stop seizures and improve neurodevelopmental outcomes in newborns under three months old with hemimegalencephaly (HME). The procedure, called an endovascular embolic hemispherectomy, can be safely used to provide definitive treatment of HME-related epilepsy in neonates and young infants. Monica Pearl, M.D., neurointerventional radiologist, and Panagiotis Kratimenos, M.D., Ph.D., neonatologist, discuss why having a multidisciplinary team skilled at this procedure is the reason we’re the only center in the world capable of providing this treatment.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/HME-teamwork-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-02-23 15:32:502024-02-23 15:34:25New hemimegalencephaly procedure is all about teamwork
Traditionally, when a baby is diagnosed with hemimegalencephaly (HME), doctors turn to a hemispherectomy at 3 months of age, which involves surgically removing half of a baby’s brain. At Children’s National Hospital, our doctors pioneered the endovascular embolic hemispherectomy, an approach using induced controlled strokes to eliminate the affected part of the brain, halting seizures. Monica Pearl, M.D., neurointerventional radiologist, and Tammy Tsuchida, M.D., Ph.D., neonatal neurologist, talk about this life-changing procedure.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/baby-being-monitored-Feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-02-23 15:21:162024-02-23 15:37:27The history behind the novel hemimegalencephaly procedure
When a family from Texas received a shocking diagnosis for their newborn daughter, they knew there was one place they needed to go – Children’s National Hospital in Washington, D.C. At birth, Angelique was diagnosed with a rare and devastating condition known as hemimegalencephaly (HME) which causes uncontrollable and frequent seizures. Monica Pearl, M.D., neurointerventional radiologist, and the team at Children’s National have pioneered an approach to treat HME, where they induce controlled strokes to eliminate the affected part of the brain, halting seizures in their tracks. They’re the only team in the world doing this work. Angelique’s parents knew the clock was ticking — every day they waited meant irreversible damage to their daughter’s developing brain.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/Angelique-and-family-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-02-23 14:09:202024-02-23 15:37:11Inducing strokes to better treat babies with hemimegalencephaly
The team found differences in the brains of both infants whose mothers were infected with COVID while pregnant, as well as those born to mothers who did not test positive for the virus.
Babies born during the COVID-19 pandemic have differences in the size of certain structures in the brain, compared to infants born before the pandemic, according to a new study led by researchers at Children’s National Hospital.
The team found differences in the brains of both infants whose mothers were infected with COVID while pregnant, as well as those born to mothers who did not test positive for the virus, according to the study published in Cerebral Cortex.
The findings suggest that exposure to the coronavirus and being pregnant during the pandemic could play a role in shaping infant brain development, said Nickie Andescavage, M.D., the first author of the paper and associate chief for the Developing Brain Institute at Children’s National.
The fine print
The study’s authors looked at three groups of infants: 108 born before the pandemic; 47 exposed to COVID before birth; and 55 unexposed infants. In all cases, researchers performed magnetic resonance imaging (MRI) scans of the newborns’ brains during the first few weeks of life. The MRI scans, which are non-invasive and do not expose patients to radiation, provided 3D images of the brain, allowing doctors to calculate the volume of different areas.
Researchers found several differences in the brains of babies exposed to COVID. They had larger volumes of the gray matter that makes up the brain’s outermost layer, compared to the two other groups. In contrast, an inner area of the brain, known as deep gray matter, was smaller than in unexposed babies. These are areas that contain large numbers of neurons that generate and process signals throughout the brain. “Their brains formed differently if they were exposed to COVID,” said Dr. Andescavage, adding that “those exposed to COVID had unique signatures” in the brain.
Doctors also measured the depths of the folds in the babies’ brains – a way to determine how the brain is maturing during early development. Babies born to mothers who had COVID in pregnancy had deeper grooves in the frontal lobe, while babies born during the pandemic – even without being exposed to COVID – had increased folds and grooves throughout the brain, compared to babies born before the pandemic. “There was something about being born during the pandemic that changed how the brain developed,” Dr. Andescavage said.
What’s ahead
The study authors can’t fully explain what caused the differences in brain development in these babies, Dr. Andescavage said. But other studies have linked maternal stress and depression to changes in the newborn brain. In a future study, Dr. Andescavage and her colleagues will examine the relationship between infant brain development and how stress and anxiety during the pandemic may have played a role in early development.
Because the babies in the study were just a few weeks old, researchers don’t know if their altered brain development will affect how they learn or behave. Researchers plan to follow the children until age 6, allowing them to observe whether pandemic-era babies hit key developmental milestones on time, such as walking, talking, holding a crayon and learning the alphabet.
Although the coronavirus rarely crosses the placenta to infect the fetus directly, there are other ways maternal infection can influence the developing baby. Dr. Andescavage said inflammation is one potential harm to a developing baby. In addition, if a pregnant woman becomes so sick that the levels of oxygen in her blood fall significantly, that can deprive the fetus of oxygen, she added.
In recent decades, studies of large populations have found that maternal infections with influenza and other viruses increased the risk of serious problems in children even years later, including autism, attention deficit hyperactivity disorder and schizophrenia, although the reasons behind the association are not well understood. Technology may allow doctors to answer a number of questions about COVID and the infant brain.
“With advanced imaging and MRI, we’re in a position now to be able to understand how the babies are developing in ways we never previously could,” Dr. Andescavage said. “That will better allow us to identify the exposures that may be harmful, and at what times babies may be especially vulnerable, to better position us to promote maternal wellness. This, in turn, helps infant wellness.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/02/pregnant-woman-with-doctor-CNRI.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-02-21 19:05:552024-02-27 11:10:38Prenatal COVID exposure associated with changes in newborn brain
Explore some of the notable medical advancements and stories of bravery that defined 2023, showcasing the steadfast commitment of healthcare professionals at Children’s National Hospital and the resilient spirit of the children they support. Delve into our 2023 news highlights for more.
According to a study published in British Medical Journal Global Health, women who get COVID during pregnancy are nearly eight times more likely to die and face a significantly elevated risk of ICU admission and pneumonia. Sarah Mulkey, M.D., prenatal-neonatologist neurologist, discussed findings based on her work with pregnant women and their babies. (Fortune)
A study led by Christopher Vaughan, Psy.D., pediatric neuropsychologist, suggests that — despite what many people may presume — getting kids back to school quickly is the best way to boost their chance for a rapid recovery after a concussion. (CNN)
David Wessel, M.D., executive vice president, chief medical officer and physician-in-chief, explained that one reason parents were still having trouble getting their children beds in a pediatric hospital or a pediatric unit after the fall 2022 respiratory surge is that pediatric hospitals are paid less by insurance. (CNN)
Anisha Abraham, M.D., M.P.H., chief of the Division of Adolescent and Young Adult Medicine, joined America’s Newsroom to discuss the impact social media access has had on children’s mental health.
(FOX News)
After 13-year-old Antonio was nearly killed outside his mom’s apartment, Children’s National Hospital went beyond treating his bullet wounds. Read how our Youth Violence Intervention Program team supported him and his family during his recovery.
(The Washington Post)
Erin and Jade Buckles underwent a successful separation at Children’s National Hospital. Nearly 20 years later they returned to meet with some of the medical staff who helped make it happen. (Good Morning America)
Shilpa Patel, M.D., M.P.H., medical director of the Children’s National IMPACT DC Asthma Clinic, weighed in on a letter published in Annals of Allergy, Asthma & Immunology, asserting that the disparities in mortality due to asthma in the United States vary based on whether they occurred in a hospital, ethnicity or race and age of the patient. (Healio)
After one family embarked on a perilous journey from Afghanistan through Mexico to the U.S.-Mexico border, they eventually secured entry to the U.S. where Karen Smith, M.D., medical director of Global Services, aided the family’s transition and provided their daughter with necessary immediate medical treatment. (NPR)
With the number of young people shot by guns on the rise in the U.S., providers and staff at Children’s National Hospital are trying to break the cycle of violence. But it’s not just the physical wounds though that need treating: young victims may also need help getting back on the right track — whether that means enrolling in school, finding a new group of friends or getting a job. (BBC News)
Callie, a 6-year-old diagnosed with diffuse intrinsic pontine glioma, was treated with low-intensity focused ultrasound (LIFU) at Children’s National Hospital and is the second child in the world to receive this treatment for a brain tumor. LIFU is an emerging technology that experts like Hasan Syed, M.D., and Adrianna Fonseca, M.D., are trialing to treat this fatal childhood brain tumor. (The Washington Post)
The FDA approved a new genetic therapy, giving people with sickle cell disease new opportunities to eliminate their symptoms. David Jacobsohn, M.B.A., M.D., confirmed that Children’s National Hospital is one of the authorized treatment centers and talked about giving priority to the sickest patients if they are on Vertex’s list.
(The New York Times)
After the potential need for open-heart surgery threatened Caroline’s Nutcracker performance, Manan Desai, M.D., a cardiac surgeon, figured out a less invasive procedure to help reduce her recovery time so she could perform in time for the holidays. (Good Morning America)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/01/News-logo-collage-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-01-18 12:50:142024-01-23 09:43:11Children’s National in the News: 2023
Artificial intelligence (AI) has the potential to detect rheumatic heart disease (RHD) with the same accuracy as a cardiologist, according to new research demonstrating how sophisticated deep learning technology can be applied to this disease of inequity. The work could prevent hundreds of thousands of unnecessary deaths around the world annually.
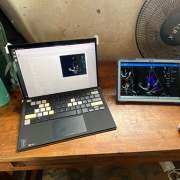
Developed at Children’s National Hospital and detailed in the latest edition of the Journal of the American Heart Association, the new AI system combines the power of novel ultrasound probes with portable electronic devices installed with algorithms capable of diagnosing RHD on echocardiogram. Distributing these devices could allow healthcare workers, without specialized medical degrees, to carry technology that could detect RHD in regions where it remains endemic.
RHD is caused by the body’s reaction to repeated Strep A bacterial infections and can cause permanent heart damage. If detected early, the condition is treatable with penicillin, a widely available antibiotic. In the United States and other high-income nations, RHD has been almost entirely eradicated. However, in low- and middle-income countries, it impacts the lives of 40 million people, causing nearly 400,000 deaths a year.
“This technology has the potential to extend the reach of a cardiologist to anywhere in the world,” said Kelsey Brown, M.D., a cardiology fellow at Children’s National and co-lead author on the manuscript with Staff Scientist Pooneh Roshanitabrizi, Ph.D. “In one minute, anyone trained to use our system can screen a child to find out if their heart is demonstrating signs of RHD. This will lead them to more specialized care and a simple antibiotic to prevent this degenerative disease from critically damaging their hearts.”
The big picture
The new AI system combines the power of novel ultrasound probes with portable electronic devices installed with algorithms capable of diagnosing RHD on echocardiogram.
Millions of citizens in impoverished countries have limited access to specialized care. Yet the gold standard for diagnosing RHD requires a highly trained cardiologist to read an echocardiogram — a non-invasive and widely distributed ultrasound imaging technology. Without access to a cardiologist, the condition may remain undetected and lead to complications, including advanced cardiac disease and even death.
According to the new research, the AI algorithm developed at Children’s National identified mitral regurgitation in up to 90% of children with RHD. This tell-tale sign of the disease causes the mitral valve flaps to close improperly, leading to backward blood flow in the heart.
Beginning in March, Craig Sable, M.D., interim division chief of Cardiology, and his partners on the project will implement a pilot program in Uganda incorporating AI into the echo screening process of children being checked for RHD. The team believes that a handheld ultrasound probe, a tablet and a laptop — installed with the sophisticated, new algorithm — could make all the difference in diagnosing these children early enough to change outcomes.
“One of the most effective ways to prevent rheumatic heart disease is to find the patients that are affected in the very early stages, give them monthly penicillin for pennies a day and prevent them from becoming one of the 400,000 people a year who die from this disease,” Dr. Sable said. “Once this technology is built and distributed at a scale to address the need, we are optimistic that it holds great promise to bring highly accurate care to economically disadvantaged countries and help eradicate RHD around the world.”
Children’s National Hospital leads the way
To devise the best approach, two Children’s National experts in AI — Dr. Roshanitabrizi and Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation — tested a variety of modalities in machine learning, which mimics human intelligence, and deep learning, which goes beyond the human capacity to learn. They combined the power of both approaches to optimize the novel algorithm, which is trained to interpret ultrasound images of the heart to detect RHD.
Already, the AI algorithm has analyzed 39 features of hearts with RHD that cardiologists cannot detect or measure with the naked eye. For example, cardiologists know that the heart’s size matters when diagnosing RHD. Current guidelines lay out diagnostic criteria using two weight categories — above or below 66 pounds — as a surrogate measure for the heart’s size. Yet the size of a child’s heart can vary widely in those two groupings.
“Our algorithm can see and make adjustments for the heart’s size as a continuously fluid variable,” Dr. Roshanitabrizi said. “In the hands of healthcare workers, we expect the technology to amplify human capabilities to make calculations far more quickly and precisely than the human eye and brain, saving countless lives.”
Among other challenges, the team had to design new ways to teach the AI to handle the inherent clinical differences found in ultrasound images, along with the complexities of evaluating color Doppler echocardiograms, which historically have required specialized human skill to evaluate.
“There is a true art to interpreting this kind of information, but we now know how to teach a machine to learn faster and possibly better than the human eye and brain,” Dr. Linguraru said. “Although we have been using this diagnostic and treatment approach since World War II, we haven’t been able to share this competency globally with low- and middle-income countries, where there are far fewer cardiologists. With the power of AI, we expect that we can, which will improve equity in medicine around the world.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/01/RHD-AI-system-CNRI-feature.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-01-16 08:00:362025-05-06 13:50:21Novel AI platform matches cardiologists in detecting rheumatic heart disease
Advanced MRI visualization techniques to follow blood flow in the hearts of cardiac patients. Gene therapy for pediatric patients with Duchenne muscular dystrophy. 3D-printed casts for treating clubfoot. These were among the most popular articles we published on Innovation District in 2023. Read on for our full list.
Cardiac imaging specialists and cardiac surgeons at Children’s National Hospital are applying advanced magnetic resonance imaging visualization techniques to understand the intricacies of blood flow within the heart chambers of children with single ventricle heart defects like hypoplastic left heart syndrome. The data allows surgeons to make critical corrections to the atrioventricular valve before a child undergoes the single ventricle procedure known as the Fontan. (3 min. read)
Children’s National Hospital became the first pediatric hospital to administer a commercial dose of Elevidys (delandistrogene moxeparvovec-rokl), the first gene therapy for the treatment of pediatric patients with Duchenne muscular dystrophy (DMD). Elevidys is a one-time intravenous gene therapy that aims to delay or halt the progression of DMD by delivering a modified, functional version of dystrophin to muscle cells. (2 min. read)
Researchers at Children’s National Hospital developed a pre-clinical model to test drugs and therapies for Becker Muscular Dystrophy (BMD), a debilitating neuromuscular disease that is growing in numbers and lacks treatment options. The work provides scientists with a much-needed method to identify, develop and de-risk drugs for patients with BMD. (2 min. read)
In 2022, five newborns with life-threatening congenital heart disease affecting their heart rhythms were the first in the United States to receive a novel modified pacemaker generator to stabilize their heart rhythms within days of birth. Two of the five cases were cared for at Children’s National Hospital. In a follow-up article, the team at Children’s National shared that “early post-operative performance of this device has been excellent.” (2 min. read)
Experts from the Food and Drug Administration, Pfizer, Oracle Health, NVIDIA, AWS Health and elsewhere came together to discuss how pediatric specialties can use AI to provide medical care to kids more efficiently, more quickly and more effectively at the inaugural symposium on AI in Pediatric Health and Rare Diseases, hosted by Children’s National Hospital and the Fralin Biomedical Research Institute at Virginia Tech. (3 min. read)
The American Academy of Pediatrics (AAP) named a 2019 study led by clinician-researchers at Children’s National Hospital one of the 12 most influential Pediatric Emergency Medicine articles ever published in the journal Pediatrics. The findings showed that states with stricter gun laws and laws requiring universal background checks for gun purchases had lower firearm-related pediatric mortality rates but that more investigation was needed to better understand the impact of firearm legislation on pediatric mortality. (2 min. read)
Children’s National Hospital recently welcomed pediatric and adult colorectal surgeon Erin Teeple, M.D., to the Division of Colorectal and Pelvic Reconstruction. Dr. Teeple is the only person in the United States who is board-certified as both a pediatric surgeon and adult colorectal surgeon, uniquely positioning her to care for people with both acquired and congenital colorectal disease and help them transition from pediatric care to adult caregivers. (3 min. read)
The sickle cell team at Children’s National Hospital received a grant from the Founders Auxiliary Board to launch a first-of-its-kind, personalized holistic transformative program for the management of pain in sickle cell disease. The clinic uses an inter-disciplinary approach of hematology, psychology, psychiatry, anesthesiology/pain medicine, acupuncture, mindfulness, relaxation and aromatherapy services. (3 min read)
Non-invasive prenatal testing using cell-free DNA (cfDNA) is currently offered to all pregnant women regardless of the fetal risk. In a study published in the American Journal of Obstetrics and Gynecology, researchers from Children’s National Hospital provided context and expert recommendations for maternal and fetal evaluation and management when cfDNA screening is positive for monosomy X or Turner Syndrome. (2 min. read)
While clubfoot is relatively common and the treatment is highly successful, the weekly visits required for Ponseti casting can be a significant burden on families. Researchers at Children’s National Hospital are looking for a way to relieve that burden with a new study that could eliminate the weekly visits with a series of 3D-printed casts that families can switch out at home. (1 min. read)
A new validated self-report tool provides researchers with a way to characterize the gender of research participants beyond their binary designated sex at birth. The multi-dimensional Gender Self-Report, developed using a community-driven approach and then scientifically validated, was outlined in a peer-reviewed article in the American Psychologist, a journal of the American Psychological Association. (2 min. read)
In a study published by Advances in Chronic Kidney Disease, a team at Children’s National Hospital reviewed cardiovascular and bone diseases in chronic kidney disease and end-stage kidney disease patients with a focus on pediatric issues and concerns. (1 min. read)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/2023-with-lightbulb-CNRI-feature.png385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-12-27 10:55:522023-12-28 11:49:10The best of 2023 from Innovation District
Catherine Limperopoulos, Ph.D., Yao Wu, Ph.D., and David Wessel, M.D.
Children’s National Hospital is celebrating a remarkable milestone as three of its faculty members have been honored over 15 years with the American Heart Association’s Outstanding Research in Pediatric Cardiology Award. Yao Wu, Ph.D., became the latest researcher to earn the accolade for her groundbreaking work into congenital heart disease (CHD).
A research faculty member with the newly established Center for Prenatal, Neonatal & Maternal Health Research, Dr. Wu received the award specifically for her studies on the role of altered placental function, measured by advanced in utero imaging, and neurodevelopmental outcomes in toddlers with CHD.
Honored at the association’s annual meeting in Philadelphia, Dr. Wu returned to Children’s National to warm congratulations from her colleagues who had previously won the award: David Wessel, M.D., executive vice president and chief medical officer, and Catherine Limperopoulos, Ph.D., director of the new center.
“I am thrilled to pass the baton to one of our own,” Dr. Limperopoulos said. “Dr. Wu’s recognition speaks to the outstanding and innovative research happening at Children’s National among junior faculty who are focusing on advancing our understanding of congenital heart disease and its long-term neurodevelopmental outcomes.”
Why we’re excited
The prestigious award represents more than individual accomplishments; it symbolizes three generations of mentorship and collaboration at the hospital. In 2007, Dr. Wessel joined Children’s National to enhance the care of newborns across specialty services by expanding programs and research, with a focus on critically ill newborns with heart disease. He recruited and mentored Dr. Limperopoulos in 2010, who became one of his research partners and creator of the hospital’s Center for Prenatal, Neonatal & Maternal Health Research. Dr. Limperopoulos, in turn, recruited and mentored Dr. Wu, providing her with the tools to conduct advanced imaging on in-utero brains and placentas, as well as the development of children with CHD.
“Each one of us is in different phases of our careers, yet we are connected by our deep interest in advancing cardiac care for critically ill newborns,” Dr. Wessel said. “In this collaborative environment, we learn from each other to improve entire lifetimes for our patients.”
Dr. Wu said she believes in sharing scientific developments for the advancement of the entire medical community. “It was an honor to be chosen to join this esteemed club, which has a relentless focus on improving health outcomes,” she said.
Children’s National leads the way
The award winners shared five collaborations published in leading journals to contribute to the ongoing dialogue in the field and the innovative work happening at Children’s National:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/Triple-heart-award-CNRI-Feature.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-12-13 12:02:522026-04-20 16:01:37AHA’s Outstanding Research Award: Three generations of pediatric cardiac excellence
Premature infants exposed to pain while in the Neonatal Intensive Care Unit (NICU) are at greater risk for motor delays, language deficits and autism, even in the absence of structural brain injuries, according to findings from the new Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital.
Premature infants exposed to pain while in the Neonatal Intensive Care Unit (NICU) are at greater risk for motor delays, language deficits and autism, even in the absence of structural brain injuries, according to findings from the new Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital.
The research sheds light on the potential outcomes of routine medical interventions – such as heel pricks, venipunctures and IV placements – and correlates these skin breaks to changes in neurological connectivity in the preterm infants’ brains. Published in BMC Medicine, the work provides valuable insights about the far-reaching impact of early medical care.
“We know that premature babies are often exposed to repeated medical interventions, light, sound and other stimuli that they would not experience in utero, and we wanted to better understand the long-term effect,” said Kevin Cook, Ph.D., research faculty at the new center and an expert in fetal and neonatal neurology. “Through this study, we can see that early and repeated exposure to pain appears to alter brain development and put children at risk for poor neurodevelopmental outcomes.”
The big picture
Globally, nearly 1 in 10 babies is born preterm, and the Children’s National team was particularly interested in the experience of those born “very” and “extremely” preterm, which is considered any delivery earlier than 32 and 28 weeks of gestation, respectively. While rates of prematurity have been relatively stable, survival rates of these babies have increased remarkably in recent decades, thanks to improved interventions and therapies for preterm infants. Yet neurodevelopmental challenges among these children persist, with noteworthy risks of autism and other neurological deficits.
At Children’s National, researchers are working to understand the mechanism behind those challenges. Given that the late second trimester and the third trimester are critical periods for brain development, the team wanted to study the effects of exposing babies to the world outside the womb early.
The fine print
Dr. Cook and his colleagues collected resting-state functional MRI (fMRI) scans from 148 infants born at least four weeks prematurely, along with 99 infants born full term. The fMRI scans, uniquely suited for studying the resting state of the brain in non-responsive infants, revealed significant hyperconnectivity within the cerebellum, which coordinates muscle activity, and the limbic and paralimbic regions, which govern emotions, motivation and cognitive functions.
Notably, the hyperconnectivity correlated with the number of skin break procedures, including heel pricks, venipunctures and IV placements. When the children returned for developmental evaluations at 18 months, the skin breaks were strongly associated with an increased risk of autism and lower motor and language scores. The toddlers identified at risk for autism had an average of 118 skin breaks, which is significantly more than the average of 65 skin breaks in those who were not at risk.
What’s ahead
Catherine Limperopoulos, Ph.D., director of the Center for Prenatal, Neonatal & Maternal Health Research, said the findings have important implications for understanding how painful NICU procedures can impact long-term outcomes and how physicians conceptualize the risks of care given to preterm babies. She and her team at the center recommend further research into managing pain in premature babies, especially given the limits of current options and the known risk of opioids.
“With this foundational study, we should consider ways to improve pain management for preterm infants and methods to better weigh the interventions used on these incredibly vulnerable patients,” Dr. Limperopoulos said. “Saving their lives is certainly the priority, and the quality of that life should also be forefront of our minds.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/NICU-baby-featured.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-12-12 16:12:052023-12-12 16:14:22Painful NICU procedures change neurological development in preterm babies
The hospital will advocate for the unique needs of children as part of nationwide network working to accelerate transformative health solutions.
Children’s National Hospital was selected as a spoke for the Investor Catalyst Hub, a regional hub of ARPANET-H, a nationwide health innovation network launched by the Advanced Research Projects Agency for Health (ARPA-H).
The Investor Catalyst Hub seeks to accelerate the commercialization of groundbreaking and accessible biomedical solutions. It uses an innovative hub-and-spoke model designed to reach a wide range of nonprofit organizations and Minority-Serving Institutions, with the aim of delivering scalable healthcare outcomes for all Americans.
“The needs of children often differ significantly from those of adults. This partnership reflects our commitment to advancing pediatric healthcare through innovation and making sure we’re addressing those needs effectively,” said Kolaleh Eskandanian, Ph.D., M.B.A., vice president and chief innovation officer at Children’s National. “Leveraging the strength of this hub-and-spoke model, we anticipate delivering transformative solutions to enhance the health and well-being of the patients and families we serve.”
Children’s National joins a dynamic nationwide network of organizations aligned to ARPA-H’s overarching mission to improve health outcomes through the following research focus areas: health science futures, proactive health, scalable solutions and resilient systems. Investor Catalyst Hub spokes represent a broad spectrum of expertise, geographic diversity and community perspectives.
“Our spoke network embodies a rich and representative range of perspectives and expertise,” said Mark Marino, vice president of Growth Strategy and Development for VentureWell and project director for the Investor Catalyst Hub. “Our spokes comprise a richly diverse network that will be instrumental in ensuring that equitable health solutions reach communities across every state and tribal nation.”
As an Investor Catalyst Hub spoke, Children’s National gains access to potential funding and flexible contracting for faster award execution compared to traditional government contracts. Spoke membership also offers opportunities to provide input on ARPA-H challenge areas and priorities, along with access to valuable networking opportunities and a robust resource library.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/11/ARPA-H-Spoke-Graphic-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-11-13 11:36:432025-06-10 12:21:38Children’s National selected as member of ARPA-H Investor Catalyst Hub spoke network
Children’s National Hospital was awarded nearly $7.5 million in a five-year grant to continue its leadership of an FDA-funded pediatric device consortium. Building upon a decade of previous consortium leadership, the new consortium is Alliance for Pediatric Device Innovation (APDI) and features a new and expanded roster of partners that reflects its added focus on providing pediatric innovators with expert support on evidence generation, including the use of real-world evidence (RWE), for pediatric device development.
Collaborating for success
With the goal of helping more pediatric medical devices complete the journey to commercialization, APDI is led by Children’s National, with Kolaleh Eskandanian, Ph.D., M.B.A., vice president and chief innovation officer, serving as program director and principal investigator, and Julia Finkel, M.D., pediatric anesthesiologist and director of Pain Medicine Research and Development in the Sheikh Zayed Institute for Pediatric Surgical Innovation, serving as principal investigator.
Consortium members include Johns Hopkins University, CIMIT at Mass General Brigham, Tufts Medical Center, Medstar Health Research Institute and MedTech Color. Publicly traded OrthoPediatrics Corp., which exclusively focuses on advancing pediatric orthopedics, is serving as APDI’s strategic advisor and role model for device innovators whose primary focus is children.
Why we’re excited
Consortium initiatives got underway quickly with the announcement of a special MedTech Color edition of the “Make Your Medical Device Pitch for Kids!”™ competition that focuses on African American and Hispanic innovators. Interested innovators can find details and apply at MedTech Color Pitch Competition. The competition was announced at the recent MedTech Color networking breakfast on Oct. 10,2023 at The MedTech Conference powered by AdvaMed.
“We all benefit from greater equity and inclusion among pediatric MedTech founders, decision-makers, investigators and developers in more effectively addressing the needs of the entire pediatric population,” said Eskandanian. “We need the expertise and insights of innovators from diverse backgrounds, and we want to provide these talented individuals with more opportunities to present their work and share their perspectives on pediatric device development.”
Additional details
APDI is one of five FDA-funded consortia created to provide a platform of services, expertise and funding to help pediatric innovators bring medical devices to the market that specifically address the needs of children.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/11/Childrens-National-MedTech-Color-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-11-02 17:47:342025-03-10 13:58:01Children’s National awarded nearly $7.5 million by FDA to lead pediatric device innovation consortium
In their study, the team at Children’s National Hospital found that specific brain regions become especially vulnerable to injury around 24 weeks of pregnancy when developing babies begin to have high energy demands and rapid neurovascular changes.
For the first time, researchers have found that babies born with congenital heart disease (CHD) have alterations to the emerging functional connectivity of their brains in utero. The changes are related to the subtype of their CHD and their oxygen status before they have lifesaving surgery to treat their cardiac malformation, according to new findings published in the American Heart Association’s Circulation Research.
In their study, the team at Children’s National Hospital found that specific brain regions become especially vulnerable to injury around 24 weeks of pregnancy when developing babies begin to have high energy demands and rapid neurovascular changes. That leaves certain parts of the brain, including the brainstem, more susceptible to injury from cardiac complications and poor circulation.
“We used a special type of magnetic resonance imaging to safely study the brains of these unborn babies, and we found that they have weakened connectivity in the deep grey structures, which are responsible for sensation, movement, alertness and other core functions,” said Josepheen De Asis-Cruz, M.D., Ph.D., assistant professor at the Developing Brain Institute at Children’s National and an author of the study. “This offers an important clue in utero to the type of care the babies will eventually need when they are born.”
The big picture
In the past decade, the survival rate for fetuses with CHD has greatly improved. About 80% of cases – even some of the most high-risk heart defects – can be successfully treated or palliated with surgery and survive. Yet Dr. Cruz said researchers are finding that the rates of poor neurodevelopmental outcomes are about the same. That’s why she and her colleagues are looking at what precisely may be injuring the brains of these newborns prior to surgery, offering a possible roadmap to interventions.
The fine print
The research team studied 107 healthy, low-risk pregnancies and 75 pregnancies known to be complicated by CHD. They used functional connectivity magnetic resonance imaging (fcMRI) to examine the emerging connections of the brains of unborn babies, given fcMRI’s unique ability to query the brain in a resting state when a patient is unable to respond to tasks. They also studied the oxygen saturation levels of the babies after they were born and then mapped all of this information to the type of CHD that they were diagnosed with.
“Our findings indicate that the compromised connectivity in the brains of CHD patients before delivery is linked to hypoxia after birth,” Cruz said. “There were important differences in the low- and high-risk CHD groups. Babies born with transposition of the great arteries or hypoplastic left heart syndrome – two of the most high-risk diagnoses – have notable changes in their brain function, which could someday be used as biomarkers to guide their care.”
What’s ahead
Researchers at Children’s National are working together, using a variety of modalities, to move toward precision imaging in utero to help predict a child’s neurodevelopmental outcomes. The ultimate goal: better interventions sooner.
“This work is foundational. As we fine-tune more techniques to identify babies at risk, we can understand how environmental, genetic and epigenetic factors impact brain development and guide care decisions,” said Catherine Limperopoulos, Ph.D., director of the Center for Prenatal, Neonatal & Maternal Health Research and a senior author of the paper. “We can imagine a day where we can offer pregnant mothers highly detailed and personalized information about their unborn baby, and individualized interventions that lead to healthier lifetimes.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/10/pregnant-woman-looking-at-sonogram.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2023-11-01 07:00:492026-04-15 16:19:51Babies with congenital heart disease display disrupted brain function before birth
































 Advanced MRI visualization techniques to follow blood flow in the hearts of cardiac patients. Gene therapy for pediatric patients with Duchenne muscular dystrophy. 3D-printed casts for treating clubfoot. These were among the most popular articles we published on Innovation District in 2023. Read on for our full list.
Advanced MRI visualization techniques to follow blood flow in the hearts of cardiac patients. Gene therapy for pediatric patients with Duchenne muscular dystrophy. 3D-printed casts for treating clubfoot. These were among the most popular articles we published on Innovation District in 2023. Read on for our full list.




 The hospital will advocate for the unique needs of children as part of nationwide network working to accelerate transformative health solutions.
The hospital will advocate for the unique needs of children as part of nationwide network working to accelerate transformative health solutions.
 Children’s National Hospital was awarded nearly $7.5 million in a five-year grant to continue its leadership of an FDA-funded pediatric device consortium. Building upon a decade of previous consortium leadership, the new consortium is Alliance for Pediatric Device Innovation (APDI) and features a new and expanded roster of partners that reflects its added focus on providing pediatric innovators with expert support on evidence generation, including the use of real-world evidence (RWE), for pediatric device development.
Children’s National Hospital was awarded nearly $7.5 million in a five-year grant to continue its leadership of an FDA-funded pediatric device consortium. Building upon a decade of previous consortium leadership, the new consortium is Alliance for Pediatric Device Innovation (APDI) and features a new and expanded roster of partners that reflects its added focus on providing pediatric innovators with expert support on evidence generation, including the use of real-world evidence (RWE), for pediatric device development.
