Several experts, including Gerard R. Martin, M.D., recently published recommendations for the use and standardization of pulse oximetry screening for critical congenital heart defects in newborns.
The European Pulse Oximetry Screening Workgroup recently published recommendations for the use and standardization of pulse oximetry screening for critical congenital heart defects in newborns. Children’s National Medical Director of Global Services Gerard R. Martin, M.D., was among the experts that compiled the recommendations.
Approximately 1 in 500 babies is born with a critical congenital heart defect (CCHD). Because these conditions can cause serious, life-threatening symptoms, early detection and intervention is essential. Pulse oximetry screening (POS) – a method that measures oxygen saturation – is regarded as a simple, quick and reliable tool for early detection of CCHD, and was recommended for use in screening by the American Academy of Pediatrics and the American Heart Association in 2011.
In Europe, although POS is being used by an increasing number of hospitals, few countries have issued national guidelines recommending universal POS. To remedy this situation, neonatologists, experts in CCHD screening, and representatives from major scientific pediatric societies across Europe came together to create recommendations for the use and standardization of POS for early detection of CCHD across Europe.
Their recommendations, which were published in The Lancet, are as follows:
POS for critical congenital heart defects should be recommended for all European countries
POS should be done with new-generation equipment that is motion tolerant
Screening should occur after 6 hours of life or before discharge from the birthing centre (preferably within 24 hours after birth)
Screening should be done in two extremities: the right hand and either foot
Each country should consider the advantages and disadvantages of the two available protocols and use that which best suits their population
A new four-year NIH grant will enable Zhe Han, Ph.D., to carry out the latest stage in the detective work to determine how histone-modifying genes regulate heart development and the molecular mechanisms of congenital heart disease caused by these genetic mutations.
The National Institutes of Health (NIH) has awarded $1.75 million to a research lab led by Zhe Han, Ph.D., principal investigator and associate professor in the Center for Genetic Medicine Research, in order to build models of congenital heart disease (CHD) that are tailored to the unique genetic sequences of individual patients.
Han was the first researcher to create a Drosophila melanogaster model to efficiently study genes involved in CHD, the No.1 birth defect experienced by newborns, based on sequencing data from patients with the heart condition. While surgery can fix more than 90 percent of such heart defects, an ongoing challenge is how to contend with the remaining cases since mutations of a vast array of genes could trigger any individual CHD case.
In a landmark paper published in 2013 in the journal Nature, five different institutions sequenced the genomes of more than 300 patients with CHD and their families, identifying 200 mutated genes of interest.
“Even though mutations of these genes were identified from patients with CHD, these genes cannot be called ‘CHD genes’ since we had no in vivo evidence to demonstrate these genes are involved in heart development,” Han says. “A key question to be answered: How do we efficiently test a large number of candidate disease genes in an experimental model system?”
In early 2017, Han published a paper in Elife providing the answer to that lingering question. By silencing genes in a fly model of human CHD, the research team confirmed which genes play important roles in development. The largest group of genes that were validated in Han’s study were histone-modifying genes. (DNA winds around the histone protein, like thread wrapped around a spool, to become packed into a higher-level structure.)
The new four-year NIH grant will enable Han to carry out the next stage of the detective work to determine precisely how histone-modifying genes regulate heart development. In order to do so, his group will silence the function of histone-modifying genes one by one, to study their function in the fly heart development and to identify the key histone-modifying genes for heart development. And because patients with CHD can have more than one mutated gene, he will silence multiple genes simultaneously to determine how those genes work in partnership to cause heart development to go awry.
By the end of the four-year research project, Han hopes to be able to identify all of the histone-modified genes that play pivotal roles in development of the heart in order to use those genes to tailor make personalized fly models corresponding to individual patient’s genetic makeup.
Parents with mutations linked to CHD are likely to pass heart disease risk to the next generation. One day, those parents could have an opportunity to sequence their genes to learn the degree of CHD risk their offspring face.
“Funding this type of basic research enables us to understand which genes are important for heart development and how. With this knowledge, in the near future we could predict the chances of a baby being born with CHD, and cure it by using gene-editing approaches to prevent passing disease to the next generation,” Han says.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/11/Fruit-Fly-Han-Lab-HomePage-e1501524130644.jpg299399Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-07-31 13:42:542019-11-18 14:31:15Lab led by Zhe Han, Ph.D., receives $1.75 million from NIH
In the Clinical Report, a study team describes the current state of play and offers evidence-based recommendations to guide clinicians on how to approach metabolic syndrome in children and adolescents.
For more than a decade and a half, researchers and clinicians have used the term “metabolic syndrome” (MetS) to describe a set of symptoms that can raise the risk of cardiovascular disease. Although this constellation of factors has proven to be a good predictor of cardiometabolic risk in adults, it has not been as useful for children. That’s why the American Academy of Pediatrics (AAP) now recommends that pediatricians instead focus on clusters of cardiometabolic risk factors that are associated with obesity, a condition that currently affects one in six U.S. children and adolescents.
In a new collaborative report, a study team from Children’s National Health System’s Division of Endocrinology and Diabetes, Harvard Medical School and Duke Children’s Hospital and Health Center describes the current state of play and offers evidence-based recommendations to guide clinicians on how to approach MetS in children and adolescents.
Adults with MetS have at least three of the following five individual risk factors:
Decreased high-density lipoprotein cholesterol (HDL-C), so-called “good” cholesterol and
Elevated blood pressure (hypertension).
This toxic combination ups adults’ odds of developing diabetes or heart disease. The process is set in motion by insulin resistance. Think Mousetrap, with each new development facilitating the next worrisome step. As fat expands, the cells become enlarged and become more resistant to insulin – a hormone that normally helps cells absorb glucose, an energy source. However, insulin retains the ability to stimulate fatty acids, which promotes even more fat cell expansion. Ectopic fat ends up stored in unexpected places, such as the liver. To top it off, the increased fat deposits end up causing increased inflammation in the system.
At least five health entities, including the World Health Organization, introduced clinical criteria to define MetS among adults, the study authors write. Although more than 40 varying definitions have been used for kids, there is no clear consensus whether to use a MetS definition for children at all, especially as adolescents mature into adulthood. Depending on the study, at least 50 percent of kids no longer meet the diagnostic criteria weeks or years after diagnosis.
“Given the absence of a consensus on the definition of MetS, the unstable nature of MetS and the lack of clarity about the predictive value of MetS for future health in pediatric populations, pediatricians are rightly confused about MetS,” the study authors write.
As a first step to lowering their patients’ cardiometabolic risks, pediatricians should prevent and treat obesity among children and adolescents, the study authors write. Each year, clinicians should perform annual obesity screening using body mass index (BMI) as a measure, and also should screen children once a year for elevated blood pressure. Nonfasting non-HDL-C or fasting lipid screening should be done for children aged 9 to 11 to identify kids whose cholesterol levels are out of line. The team also recommends screening for abnormal glucose tolerance and Type 2 diabetes in youth with BMI greater than or equal to the 85th percentile, 10 years or older (or pubertal), with two additional risk factors, such as family history, high-risk race/ethnicity, hypertension or a mother with gestational diabetes.
Pediatricians do not need to use cut points based on MetS definitions since, for many risk factors, the growing child’s risk lies along a continuum.
Treatments can include lifestyle modifications – such as adopting a negative energy balance diet, drinking water instead of sugar-sweetened beverages, participating in a moderate- to high-intensity weight-loss program, increasing physical activity and behavioral counseling.
“Identifying children with multiple cardiometabolic risk factors will enable pediatricians to target the most intensive interventions to patients who have the greatest need for risk reduction and who have the greatest potential to experience benefits from such personalized medicine,” the study authors conclude.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/07/tape-measure.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-07-25 14:55:122024-09-06 15:19:23Defining cardiovascular disease and diabetes risks in kids
A research project led by Subechhya Pradhan, Ph.D., aims to shed light on metabolism of the placenta, a poorly understood organ, and characterize early biomarkers of fetal congenital heart disease.
The placenta serves as an essential intermediary between a pregnant mother and her developing fetus, transporting in life-sustaining oxygen and nutrients, ferrying out waste and serving as interim lungs, kidneys and liver as those vital organs develop in utero.
While the placenta plays a vital role in supporting normal pregnancies, it remains largely a black box to science. A research project led by Subechhya Pradhan, Ph.D., and partially funded by a Clinical and Translational Science Institute Research Award aims to shed light on placenta metabolism and characterize possible early biomarkers of impaired placental function in fetal congenital heart disease (CHD), the most common type of birth defect.
“There is a huge information void,” says Pradhan, a research faculty member of the Developing Brain Research Laboratory at Children’s National Health System. “Right now, we do not have very much information about placenta metabolism in vivo. This would be one of the first steps to understand what is actually going on in the placenta at a biochemical level as pregnancies progress.”
The project Pradhan leads will look at the placentas of 30 women in the second and third trimesters of healthy, uncomplicated pregnancies and will compare them with placentas of 30 pregnant women whose fetuses have been diagnosed with CHD. As volunteers for a different study, the women are already undergoing magnetic resonance imaging, which takes detailed images of the placenta’s structure and architecture. The magnetic resonance spectroscopy scans that Pradhan will review show the unique chemical fingerprints of key metabolites: Choline, lipids and lactate.
Choline, a nutrient the body needs to preserve cellular structural integrity, is a marker of cell membrane turnover. Fetuses with CHD have higher concentrations of lactate in the brain, a telltale sign of a shortage of oxygen. Pradhan’s working hypothesis is that there may be differing lipid profiles and lactate levels in the placenta in pregnancies complicated by CHD. The research team will extract those metabolite concentrations from the spectral scans to describe how they evolve in both groups of pregnant women.
“While babies born with CHD can undergo surgery as early as the first few days (or sometimes hours) of life to correct their hearts, unfortunately, we still see a high prevalence of neurodevelopmental impairments in infants with CHD. This suggests that neurological dysfunctional may have its origin in fetal life,” Pradhan says.
Having an earlier idea of which fetuses with CHD are most vulnerable has the potential to pinpoint which pregnancies need more oversight and earlier intervention.
Placenta spectral data traditionally have been difficult to acquire because the pregnant mother moves as does the fetus, she adds. During the three-minute scans, the research team will try to limit excess movement using a technique called respiratory gating, which tells the machine to synchronize image acquisition so it occurs in rhythm with the women’s breathing.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/07/baby.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-07-19 15:17:392022-05-17 12:37:58Spectral data shine light on placenta
Ten-year-old Angioletta was clinically diagnosed with rheumatic heart disease in 2014 (severe leakage of her mitral valve). She’s been medically managed at the clinic Children’s helps support and conducts research at in Gulu, and she is a very active participant in the support group led by Children’s National research assistant, Amy Scheel. Angioletta hasn’t had any major complications, but her only hope for long-term survival is to undergo open heart surgery to replace her abnormal valve. Experts are looking towards the research from the new Center to help prevent future generations of children like Angioletta from developing RHD.
Known as the ‘world’s forgotten disease,’ Rheumatic Heart Disease (RHD) is caused by untreated streptococcal throat infections that progress into acute rheumatic fever (ARF) and eventually weaken the valves of the heart. It is the most common cardiovascular disease in children and young adults globally – affecting nearly 33 million people and causing 345,000 deaths annually – yet, it is preventable with early detection and access to penicillin.
To help end the epidemic, Children’s National Health System has been awarded a $3.7 million grant from the American Heart Association (AHA) to launch a Rheumatic Heart Disease Center, with the goal of developing innovative strategies and economic incentives to improve the prevention and diagnosis of RHD in high-risk, financially disadvantaged countries and low-income communities across the United States.
Children’s National is one of four centers in the AHA’s Strategically Focused Children’s Research Network, which is dedicated to improving children’s heart health and reducing the global burden of cardiovascular disease and stroke. AHA selected Children’s for the grant based on its proven record of global collaboration to solve complex health issues and the potential impact of this research. The program will use Children’s robust telemedicine infrastructure to connect co-collaborators around the world, as well as train the next generation of globally minded cardiovascular researchers.
“While it’s often thought that we’ve already beaten rheumatic heart disease, data shows there’s nearly no decrease in mortality rates in low-income countries. The disease is endemic in Sub-Saharan Africa, and some poverty-stricken communities in the U.S. are hit nearly as hard,” said Craig Sable, M.D., associate division chief of cardiology. “We are thrilled to receive this funding from the AHA, which will help us close the research gap for this neglected disease and change the plight of millions of children around the world.”
About the center and research focus areas
Over the next four years, the Rheumatic Heart Disease Center, led by Children’s National Heart Institute experts Dr. Sable and Andrea Beaton, M.D., cardiologist, along with RHD leaders around the globe, will develop evidence-based strategies to strengthen the health system’s response to RHD through synergistic basic, clinical and population science research along the entire spectrum of the disease.
The Rheumatic Heart Disease Center, led by Children’s National Heart Institute experts Andrea Beaton, M.D., and Craig Sable, M.D., along with RHD leaders around the globe, will develop evidence-based strategies to strengthen the health system’s response to RHD.
The basic research project, led by James Dale, M.D., chief of the division of infectious disease at the University of Tennessee in Memphis, will work to better define the immune system response to Group A Streptococcal (GAS) infection, or strep throat, paving the way for vaccine development. In collaboration with a partner site in Cape Town, South Africa, experts will recruit 300 children ages 5-15 to participate for 24 months in a study capturing and classifying various strains of the GAS bacteria. Similar to the common flu, the strains of GAS bacteria vary from region to region and year to year. By identifying immune system targets, or how our bodies fight GAS, the research can inform the creation of effective and long-lasting vaccines.
Dr. Beaton will lead the clinical project that will work to improve understanding and detection of ARF, the precursor to RHD. According to Dr. Beaton, the current, outdated paradigm is that patients with RHD at one point experienced a full-blown episode of ARF – including fever, severe joint pains and rash. These symptoms should be unmistakable and prompt treatment, but in truth the disease remains vastly underdiagnosed in high-risk regions. Through an on-the-ground partnership with experts at Mulago National Referral Hospital in Uganda, the clinical project will work to enroll over 1,000 children ages 3-18 with more subtle symptoms, potentially suggestive of ARF, in order to paint a more accurate picture of the disease in Africa today.
“The gap between the low number of children diagnosed with ARF and the high number of young adults with advanced RHD remains one of the most challenging mysteries and barriers to improved RHD prevention,” said Dr. Beaton. “For the first time, we will systematically characterize the clinical, laboratory and echocardiographic features of ARF in low-resource settings, with the goal of developing a biological signature for ARF that can be translated into a diagnostic test and improve detection.”
Dr. Beaton expects that this research could benefit other related diseases too, such as kidney disease or serious skin infections.
The population research project, led by David Watkins, M.D., M.P.H., an expert in epidemiological and economic modeling at the University of Washington in Seattle, will work to build an economic case for prevention around the world, using the data from the basic and clinical work. The goal is to identify local gaps in delivery of health services for disease prevention and treatment and to measure the cost-effectiveness of RHD interventions, as well as the cost of inaction – especially as patients suffering from advanced RHD are often in the prime of their productive, adult lives. Researchers anticipate the findings will provide effective tools for addressing RHD in other endemic countries too.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/07/Angioletta-Rheumatic-Heart-Disease.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-07-03 09:41:002025-02-28 12:24:29Rheumatic Heart Disease Center Launches with $3.7 Million AHA Grant
“Children should have access to the latest advances in treatment and the best care. By challenging the status quo and designing new, safe and effective alternative study designs, we can give them the best opportunity to grow up stronger,” notes David Wessel, M.D., executive vice president and chief medical officer, Hospital and Specialty Services at Children’s National Health System. Dr. Wessel is internationally recognized for his pioneering work in caring for children with heart disease. As the senior author of the new joint statement and principal investigator of the STARTS-1 trial, which is the catalyst for this collaboration, he says he is “optimistic about this forward progress.”
According to the statement, less than 50 percent of drugs approved for use in the United States have sufficient data to support labeling for dosing, safety and efficacy in children. Additionally, a 2008 report by Pasquali et al, which reviewed more than 30,000 records of hospitalized children with cardiovascular disease, found that 78 percent received at least one off-label medication and 31 percent received more than three.
There are numerous challenges in the development and approval of medications for children – especially those with rare diseases – but the paper’s lead author, Craig Sable, M.D., associate division chief of cardiology at Children’s National, says we can and need to do better.
“While randomized clinical drug trials remain the gold standard in advancing care for adults with cardiovascular disease, relying solely on these types of trials for children unnecessarily limits the drugs approved for use in children,” says Dr. Sable. “Through this unique collaboration that unifies the voice of leaders in pediatric cardiology and the FDA, our goal is to provide a framework to better define which drugs are needed and how we can create novel study designs to overcome the current trial barriers.”
To read more about the barriers and ideas presented, please find the full statement here.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-06-29 15:51:592025-02-28 12:24:55Children’s National Heart Institute experts partner with FDA and nation’s leading cardiology organizations to advance pediatric drug development
Anthony S. Fauci, M.D., director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, discussed the possibility of a reemergence of Zika virus at Children’s National Research and Education Week.
Temperatures are rising, swelling the population of Aedes mosquitoes that transmit the Zika virus and prompting an anxious question: Will the Zika epidemic re-emerge in 2017?
Anthony S. Fauci, M.D., director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (NIH), sketched out contrasting scenarios. Last year in Puerto Rico, at least 13 percent of residents were infected with Zika, “a huge percentage of the population to get infected in any one outbreak,” Dr. Fauci says. But he quickly adds: “That means that 87 percent of the population” did not get infected. When the chikungunya virus swept through the Caribbean during an earlier outbreak, it did so in multiple waves. “We are bracing for a return of Zika, but we shall see what happens.” Dr. Fauci says.
When it comes to the continental United States, however, previous dengue and chikungunya outbreaks were limited to southern Florida and Texas towns straddling the Mexican border. Domestic Zika transmission last year behaved in much the same fashion.
“Do we think we’re going to get an outbreak [of Zika] that is disseminated throughout the country? The answer is no,” Dr. Fauci adds. “We’re not going to see a major Puerto Rico-type outbreak in the continental United States.”
Dr. Fauci’s remarks were delivered April 24 to a standing-room-only auditorium as part of Research and Education Week, an annual celebration of the cutting-edge research and innovation happening every day at Children’s National. He offered a sweeping, fact-filled summary of Zika’s march across the globe: The virus was first isolated from a primate placed in a treehouse within Uganda’s Zika forest to intentionally become infected; Zika lurked under the radar for the first few decades, causing non-descript febrile illness; it bounced from country to country, causing isolated outbreaks; then, it transformed into an infectious disease of international concern when congenital Zika infection was linked to severe neural consequences for babies born in Brazil.
Zika virus lurked under the radar for several decades, causing non-descript febrile illness; it bounced from country to country, resulting in isolated outbreaks; then, it transformed into an infectious disease of international concern.
“I refer to Brazil and Zika as the perfect storm,” Dr. Fauci told attendees. “You have a country that is a large country with a lot of people, some pockets of poverty and economic depression – such as in the northeastern states – without good health care there, plenty of Aedes aegypti mosquitoes and, importantly, a totally immunologically naive population. They had never seen Zika before. The right mosquitoes. The right climate. The right people. The right immunological status. And then, you have the explosion in Brazil.”
In Brazil, 139 to 175 babies were born each year with microcephaly – a condition characterized by a smaller than normal skull – from 2010 to 2014. From 2015 through 2016, that sobering statistic soared to 5,549 microcephaly cases, 2,366 of them lab-confirmed as caused by Zika.
Microcephaly “was the showstopper that changed everything,” says Dr. Fauci. “All of a sudden, [Zika] went from a relatively trivial disease to a disease that had dire consequences if a mother was infected, particularly during the first trimester.”
As Zika infections soared, ultimately affecting more than 60 countries, the virus surprised researchers and clinicians a number of times, by:
Being spread via sex
Being transmitted via blood transfusion, a finding from Brazil that prompted the Food and Drug Administration to recommend testing for all U.S. donated blood and blood products
Decimating developing babies’ neural stem cells and causing a constellation of congenital abnormalities, including vision problems and contractions to surviving infants’ arms and legs
Causing Guillain-Barré syndrome
Triggering transient hearing loss
Causing myocarditis, heart failure and arrhythmias
When it comes to the U.S. national response, Dr. Fauci says one of the most crucial variables is how quickly a vaccine becomes available to respond to the emerging outbreak. For Zika, the research community was able to sequence the virus and launch a Phase I trial in about three months, “the quickest time frame from identification to trial in the history of all vaccinology,” he adds.
Zika is a single-stranded, enveloped RNA virus that is closely related to dengue, West Nile, Japanese encephalitis and Yellow fever viruses, which gives the NIH and others racing to produce a Zika vaccine a leg up. The Yellow fever vaccine, at 99 percent effectiveness, is one of the world’s most effective vaccines.
“I think we will wind up with an effective vaccine. I don’t want to be over confident,” Dr. Fauci says. “The reason I say I believe that we will is because [Zika is] a flavivirus, and we have been able to develop effective flavivirus vaccines. Remember, Yellow fever is not too different from Zika.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/zika-virus.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-06-05 09:40:482024-09-06 15:23:39Will the Zika epidemic re-emerge in 2017?
In a recent review article published in Circulation Research, Nobuyuki Ishibashi, M.D., and his colleagues at Children’s National Health System summarized what is currently known about how congenital heart disease affects brain maturation.
What’s known
Among all known birth defects, congenital heart disease (CHD) is the leading cause of death in infants. Fortunately, advances in surgical techniques and treatments are improving the outlook for these children, and more and more are reaching adulthood. However, because of this increased longevity, it has become increasingly clear that children born with CHD are at risk of developing life-long neurological deficits. Several risk factors for these neurodevelopmental abnormalities have been identified, but direct links between specific factors and neurological defects have yet to be established.
What’s new
In a recent review article published in Circulation Research, a team from Children’s National Health System summarized what is currently known about how CHD affects brain maturation. Drawing from studies conducted at Children’s National as well as other research institutions, Paul D. Morton, Ph.D., Nobuyuki Ishibashi, M.D., and Richard A. Jonas, M.D., write that clinical findings in patients, improvements in imaging analysis, advances in neuromonitoring techniques and the development of animal models have greatly contributed to our understanding of the neurodevelopmental changes that occur with CHD.
Findings from Children’s National include:
An assessment of the intraoperative effects of cardiopulmonary bypass surgery on white matter using neonatal piglets.
An arterial spin labeling MRI study that showed newborns with complex CHD have a significant reduction in global cerebral blood flow.
A rodent study that modeled diffuse white matter brain injury in premature birth and identified the cellular and molecular mechanisms underlying lineage-specific vulnerabilities of oligodendrocytes and their regenerative response after chronic neonatal hypoxia.
The authors conclude that although there is ample clinical evidence of neurological damage associated with CHD, there is limited knowledge of the cellular events associated with these abnormalities. They offer perspectives about what can be done to improve our understanding of neurological deficits in CHD, and emphasize that ultimately, a multidisciplinary approach combining multiple fields and myriad technology will be essential to improve or prevent adverse neurodevelopmental outcomes in individuals with CHD.
Questions for future research
Q: What are the cellular events associated with each factor involved in neurodevelopmental delays?
Q: How does the neurodevelopmental status of a patient with CHD change as they age?
Q: How do the genes involved in structural congenital cardiac anomalies affect brain development and function?
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/Nobuyuki-Ishibashi.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-06-02 12:02:112024-09-06 15:02:26Congenital heart disease and the brain
Children’s National has developed a cardio-oncology program to closely follow the heart health of oncology patients to detect and stop progression of heart disease.
The five-year survival rate for pediatric cancers has climbed to nearly 82 percent, but the damaging, long-term side effects of rigorous treatment are prevalent. Cardiac toxicity, specifically the association of several cancer therapy agents with the development of left ventricular dysfunction, cardiomyopathy, dysrhythmia, valve disease and hypertension, is an issue of growing concern. Cardiac complications are the third leading cause of death for childhood cancer survivors, only after cancer recurrence and secondary malignancy. Cardiac mortality is 10-fold higher among this population as compared with age-matched control subjects.
The American Heart Association released a statement in 2013 pointing to the need for closer monitoring of cardiac affects from cancer treatments. Craig Sable, M.D., Associate Division Chief of Cardiology at Children’s National, co-authored the statement titled “Long-term Cardiovascular Toxicity in Children, Adolescents, and Young Adults Who Receive Cancer Therapy: Pathophysiology, Course, Monitoring, Management, Prevention, and Research Directions.” The statement concluded that it is crucial to develop an optimal monitoring regimen for this specific subgroup of patients, affirming: “As clinicians continue to learn about the cardiovascular effects of cancer treatment, the importance of primary prevention becomes abundantly clear. The objective of effective monitoring is to identify signs of cardiac disease early enough to potentially prevent, reverse, or slow the deterioration of the structure and function of the heart. We must tailor therapies to decrease the risk of cardiotoxicity while balancing the beneficial effects of the cancer therapy.”
The American College of Cardiology also launched a Cardio-Oncology section dedicated to the subspecialty and noting the need for increased and closer cardiac monitoring for cancer patients. Cardiologists and oncologists at Children’s National came together to address this issue by formalizing a multidisciplinary path of care for patients with malignancies as they enter the care system.
Multidisciplinary care from point of diagnosis
“It is tremendously important that we care for the whole child, including each individual health anomaly. Working closely with the oncology team, we try to balance how we treat their cancer at the same time as managing their heart disease,” says Niti Dham, M.D.
In response to the outstanding need for cardiac observation and follow-up care for cancer patients, Children’s National developed a Cardio-Oncology Program in 2011 to closely follow the heart health of oncology patients to detect and stop progression of heart disease. Led by Niti Dham, M.D., the cardio-oncology program within the Division of Cardiology includes the Cardiology Oncology Blood (COB) Clinic, a special clinic dedicated to pediatric cancer patients. The clinic assesses cancer patients, including bone marrow transplant (BMT) patients, who have been exposed to certain medications or radiation that have shown potential long-term, negative cardiac outcomes. Patients are monitored for any early signs of cardiac changes in hopes to halt or even reverse the disease.
When a child is diagnosed with cancer that requires certain chemotherapies and radiation for treatment, Children’s National oncologists coordinate with Dr. Dham and her team for a cardiac evaluation prior to beginning treatment. Appropriate cardiac screening tests are administered based on the planned cancer treatment regimen. Cardiac health is evaluated regularly throughout the treatment course as well as after completion to continue monitoring for early signs of changes.
“The frequent, close monitoring allows Children’s experts to notice even the slightest differences in the heart, with a goal of preventing progression of cardiac disease,” says Dr. Dham.
The cardiology team works closely with the oncology team through the whole process, alerting them immediately of any changes noted. Together, the subspecialists develop a plan that is safe for each individual patient.
The program also sees patients that have pre-existing cardiac conditions prior to cancer treatments.
“It is tremendously important that we care for the whole child, including each individual health anomaly. Working closely with the oncology team, we try to balance how we treat their cancer at the same time as managing their heart disease,” says Dr. Dham.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/05/EKG-Monitor-e1496323111173.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-05-22 16:23:022025-02-28 12:24:42Protecting the hearts of pediatric cancer patients
Fat cells from obese patients have the ability to send signals that can accelerate biological processes leading to atherosclerosis.
Obesity has been linked to a variety of adverse health conditions, including Type 2 diabetes, cancer, heart attack and stroke – conditions that may begin as early as childhood in patients whose obesity also begins early. While this much is known, it has been unclear how extra fat mass might lead to these chronic health conditions.
New research from Children’s National Health System scientists might help answer this question. In findings presented at the 2017 annual meeting of the Pediatric Academic Societies, the research team shows that exosomes – nanosized chemical messages that cells send to each other to regulate protein production – isolated from very obese teenage patients behave very differently from those derived from lean patients and could be key players in heightening the risk of developing atherosclerosis. This hardening of the arteries can, in turn, increase the risk of heart disease and stroke in adulthood.
A research team led by Robert J. Freishtat, M.D., M.P.H., chief of emergency medicine at Children’s National, is exploring possible links between extra belly fat and obesity-related diseases, such as atherosclerosis, a buildup of plaque in arteries that can harden and restrict blood flow. More precise knowledge of the mechanisms by which obesity ratchets up heart risks holds the promise of helping the next generation of kids avoid experiencing chronic disease.
The working theory is that exosomes derived from belly fat from obese patients have the distinct ability to accelerate biological processes leading to atherosclerosis.
The research team isolated exosomes from five obese teenagers and compared them to five sex-matched lean adolescents. It turns out that exosomes derived from fat pick up their marching orders from microRNA content likely to target cholesterol efflux genes, which help reduce cholesterol buildup in cells.
The research team looked at differences in cholesterol efflux gene expression in THP-1 macrophages. Uptake of low-density lipoprotein cholesterol, “bad” cholesterol, was 92 percent higher than in those exposed to exosomes from obese patients compared with their lean counterparts. Exposure to obese exosomes also reduced cholesterol efflux.
“Atherogenic properties of fat-cell derived exosomes from obese patients differ markedly from the non-atherogenic profile of exosomes from lean patients. It is especially concerning that we see biological clues of heightened risk in teenagers, and the finding underscores how the seeds for atherosclerosis can be planted very early in life,” Dr. Freishtat says.
The presentation is the latest finding from a research team that, over years of work, is unraveling the mechanisms of cellular signaling by fat cells. By closely examining very obese children – who have the most severe cardiometabolic disease – the team identified strong molecular signals of disease risk that they can search for in leaner patients who may be at risk for disease years from now.
“We know that morbidly obese patients have cardiovascular issues,” explains Dr. Freishtat. “An unanswered question is for patients with no clinical symptoms who are a little overweight. Can we look at them and say whether they are at risk for developing atherosclerosis, insulin resistance or Type 2 diabetes five or 10 years down the line? That’s the whole rationale for doing this work.”
The critical issue is what exosomes are up to. Dr. Freishtat says in lean people, they’re active and are very important in maintaining stable metabolism and homeostatic processes.
“When a person becomes obese, however, exosomes evolve,” he says. “They no longer support insulin signaling, which is helpful, and drive processes in the reverse direction, repressing insulin signaling – which can be harmful,” he adds.
Ultimately, the research team aims to revolutionize how chronic diseases like Type 2 diabetes are diagnosed. For far too long, clinicians have relied on symptoms like high glucose levels and excess urination to diagnose diabetes.
“By the time you have symptoms, it’s too late,” says Dr. Freishtat. “In many cases, damage has been done by relentless exposure to high sugar levels. The biological processes that underlie the Type 2 diabetes process began five, 10, 15 years earlier. If we can detect it earlier, before symptoms arise, intervention is going to have a more significant impact on improving and extending patients’ lives.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/05/Fat-Cells.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-05-22 10:02:172023-07-03 10:34:13Cellular signals may increase atherosclerosis risk
Children’s National Health System is pleased to announce the addition of Can Yerebakan, M.D., and Karthik Ramakrishnan, M.D., to our team of pediatric cardiac surgeons.
Dr. Yerebakan comes to Children’s National from the prestigious Pediatric Heart Center in Giessen, Germany, where he was appointed as an Associate Professor of Cardiac Surgery at the Justus-Liebig-University and performed hybrid treatment of hypoplastic left heart syndrome (HLHS). He was deeply involved in mechanical circulatory support and pediatric heart transplantation in Giessen – a leading center for pediatric heart transplantation in Europe. He also served as Chief of Clinical and Experimental Research in the Department of Congenital Cardiac Surgery at Justus-Liebig-University of Giessen, where he acquired several research grants and contributed to more than 20 abstract presentations at national and international meetings and 20 papers in peer-reviewed journals. . Dr. Yerebakan has published approximately 70 scientific papers with more than 160 impact points in three different languages. He is an active reviewer for journals such as the Journal of Thoracic and Cardiovascular Surgery, European Journal of Cardiothoracic Surgery and serves as assistant editor of the Interactive Cardiovascular and Thoracic Surgery journal and Multimedia Manual Cardiothoracic Surgery journal, both of which are official journals of the European Association of Cardiothoracic Surgery. He has had a distinguished academic career and is internationally recognized for his contributions to the field of congenital cardiac surgery, particularly in the treatment of HLHS and novel surgical treatments for heart failure in the pediatric population. Prior to his tenure at Pediatric Heart Center, Dr. Yerebakan completed his fellowship at Children’s in 2011.
Dr. Ramakrishnan joined Children’s National as a fellow in 2014 after completing his fellowship in congenital cardiac surgery at two major centers in Australia. After his two-year fellowship at Children’s, he joined the faculty. Dr. Ramakrishnan has extensive experience in managing children with congenital heart disease. Apart from routine open heart procedures, he has a special expertise in extracorporeal membrane oxygenation (ECMO) procedures and patent ductus arteriosus (PDA) ligation in extremely premature babies. He also has a keen interest in studying clinical outcomes after pediatric heart surgery. His research projects have included analysis of the United Network of Organ Sharing (UNOS) and the Pediatric Health Information System® (PHIS) databases, and his research has resulted in numerous presentations at national and international meetings. Dr. Ramakrishnan is currently the principal investigator at Children’s National for the Pediatric Heart Transplant Study (PHTS) group and the study coordinator for the Congenital Heart Surgeons’ Society (CHSS) studies. He also is a member of the PHTS working group on the surveillance and diagnosis of cellular rejection, and his clinical studies have resulted in several publications in top peer-reviewed journals.
Drs. Yerebakan and Ramakrishanan join Richard Jonas, M.D., Co-director of Children’s National Heart Institute and Chief of Cardiac Surgery, and Pranava Sinha, M.D., on the Cardiac Surgery attending staff. We look forward to continuing to strengthen our program with the addition of these physicians.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-04-25 14:39:262025-02-28 12:29:01International cardiac surgery experts join Children’s National
Strokes are common and devastating complications for patients with sickle cell anemia, often leading to severe and lifelong motor and neurocognitive problems for people with this congenital blood disorder. Results of a clinical trial published in 1998 showed that having regular blood transfusions could reduce the risk of having a first stroke by 90 percent in children with sickle cell anemia. Since then, doctors have employed this prophylactic treatment widely. However, blood transfusions can be painful, inconvenient and carry substantial risks themselves — including the potential of blood-borne infections, iron overload and immune-related reactions to blood products. Finding a way to reduce stroke risk without over-relying on blood transfusions could substantially benefit patients with sickle cell anemia.
What’s new
A team of researchers, including Naomi L.C. Luban, M.D., a Children’s National Health System hematologist and laboratory medicine specialist, tested transfusions against a drug treatment called hydroxycarbamide in a clinical trial to see if the pharmaceutical intervention could reduce strokes at least as well as transfusions. The clinical trial, known as “TCD With Transfusions Changing to Hydroxyurea (TWiTCH),” assigned 60 patients with sickle cell anemia who had abnormally high transcranial Doppler (TCD) flow velocities—a measure of blood flow in the brain that suggests elevated risk of stroke—to receive hydroxycarbamide instead of transfusions. The research team compared the outcomes for these patients with 61 other patients who received standard prophylactic transfusions. Over the 24-month study period, neither group experienced any strokes, although three transient ischemic attacks (a temporary blockage of blood flow in the brain) occurred in each group. These comparable findings suggest that hydroxycarbamide treatment, also known as hydroxyurea, is on par with transfusions for preventing strokes in patients with sickle cell anemia.
Questions for future research
Q: Does hydroxycarbamide offer a long-term way for patients with sickle cell anemia to avoid transfusions? Q: Could hydroxycarbamide help patients with sickle cell anemia who already have suffered a stroke or who have had severe problems with blood vessels in their brains that impair blood flow? Q: Which other treatments can help patients avoid the myriad complications that accompany sickle cell anemia?
Children’s National Heart Institute Team at American College of Cardiology 66th Annual Scientific Session & Expo.
The world’s leading cardiovascular specialists gathered in Washington, D.C., from March 17-19, 2017, to share the newest discoveries in treatment and prevention at the American College of Cardiology 66th Annual Scientific Session & Expo. Eleven Children’s National pediatric experts presented groundbreaking research and developments from their respective specialties. Gail Pearson, M.D., Sc.D., gave the prestigious Dan G. McNamara Lecture.
In her speech titled “The Future of Congenital Heart Disease Research: Keeping the Patient-Centered Promise,” Dr. Pearson reflected on the progress of congenital heart disease research and shared powerful narratives from patient families, detailing their hopes for the future. She also unveiled what’s on the horizon, including advances in genomics research, a data commons and new approaches for rare diseases. Dr. Pearson is a cardiologist within Children’s National Heart Institute, associate director of the Division of Cardiovascular Sciences, and director of the Office of Clinical Research at the National Heart, Lung, and Blood Institute.
Other highlights from Children’s National presenters include:
The Challenge of Anti-coagulation in the Pregnant Patient with Valvular/Congenital Heart Disease and Update on the Management of Adult Congenital Heart Disease, Anitha John, M.D., Ph.D.
ACC Talk: The IMPACT Registry Can Be Used by Families to Shop for the Best Center, Gerard Martin, M.D.
Atrial Fibrillation in the Young Athlete: Who is at Risk and How do We Manage This?, Elizabeth Sherwin, M.D.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-03-29 14:09:422020-11-23 10:35:17Children’s National experts present at American College of Cardiology 66th Annual Scientific Session
A study led by Chinwe Unegbu, M.D., indicates the benefits of PDE-5 inhibitors to treat pediatric pulmonary hypertension far outweigh potential harmful side effects.
Pulmonary hypertension (PH), when pressure in the blood vessels leading from the heart to the lungs is too high, is primarily a disease of adults: Patient registries suggest that the mean age of diagnosis is around age 50. However, more and more children are developing this condition, says Chinwe Unegbu, M.D., an assistant professor in the Division of Anesthesiology, Pain and Perioperative Medicine at Children’s National Health System.
Although adults with PH have several different effective treatments, Dr. Unegbu adds, children have few options. One of these is a class of medications known as phosphodiesterase type 5 (PDE-5) inhibitors, which act on molecular pathways that can open up constricted blood vessels. However, some studies have raised questions about the safety of this class of medications, particularly with long-term use of high dosages.
In a new study, Dr. Unegbu and colleagues performed a systematic review of available literature on this class of drugs evaluating their effectiveness and safety for pediatric patients. The review showed that like all medications, PDE-5 inhibitors have some risks. However, Dr. Unegbu says, the review showed that their benefits, including improved echocardiography measurements, cardiac catheterization parameters and oxygenation, far outweigh potential harmful side effects.
“Pediatricians across the nation view the rise in pediatric PH cases with growing concern because the disease can worsen, leading to right ventricular failure and death,” says Dr. Unegbu, lead author of the study. “PH can occur in newborns, infants and children who have a number of health conditions, including congenital heart disease, the most common birth defect among newborns. There are few available treatments for the growing population of children affected by this condition, so it is heartening that the evidence supports PDE-5 inhibitors for patients with PH.”
Patients with PH experience increased pressure in the pulmonary arteries, which carry blood from the heart to the lungs where it picks up oxygen that is ferried throughout the body. According to the National Institutes of Health, this leads patients to suffer from shortness of breath while doing routine tasks, chest pain and a racing heartbeat. Changes to the arteries make it progressively harder for the heart to pump blood to the lungs, which forces the heart to work even harder. Despite the heart muscle compensating by growing larger, less blood ultimately flows from the right to the left side of the heart which can compromise the kidney, liver and other organs, Dr. Unegbu says.
The study team included four researchers from Johns Hopkins University: Corina Noje, M.D., John D. Coulson, M.D., Jodi B. Segal, M.D., M.P.H., and study senior author Lewis Romer, M.D. The researchers scoured Medline, Embase, SCOPUS and the Cochrane Central Register of Controlled Trials, looking for studies that examined PDE-5 inhibitor use by pediatric patients with primary and secondary PH. Their goals included describing the nature and scale of the pediatric PH, assessing available pharmacologic therapies and conducting the systematic review of clinical studies of PDE-5 inhibitors, a mainstay of PH therapy.
They identified 1,270 studies. Twenty-one met the criteria to be included in the comprehensive review, including eight randomized controlled trials – the gold standard. The remaining 13 were observational studies in children ranging in age from extremely preterm to adolescence.
“Although there is some risk associated with PDE-5 inhibitor use by pediatric patients with PH, overwhelmingly the data indicate the benefits of using this class of drugs far outweigh the risks. When we looked at specific clinical outcomes, we see definite improvement in a number of measures including oxygenation, hemodynamics and better clinical outcomes: The patients are doing better, feeling better and their exercise capacity rises,” Dr. Unegbu says.
Because of lingering concerns about increased mortality, they also looked at toxicity data associated with this class of drugs. “With the exception of a single trial, the remaining trials included in our review did not demonstrate increased mortality in patients placed on this class of medicines, which was reassuring to us,” she says. Side effects ranged from mild to moderate, such as flushing and headaches. “We can say with a good degree of confidence that providers should feel fairly comfortable prescribing PDE-5 inhibitors.”
Ideally, researchers would like to have access to patient-specific measures that are a good fit for neonates and infants. Unlike adults, infants’ exercise capacity cannot be measured by their ability to climb stairs or use a treadmill. Another limitation, the study authors note, is the dearth of adequately powered clinical trials conducted in kids.
“Most of the studies have been conducted in adults. However, this disease unfolds in a much different fashion in children compared with adults,” Dr. Unegbu says. “We are desperately in need of high-quality studies in the form of randomized controlled trials in pediatric patients and studies that examine the full range of formulations of this class of drugs.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/03/xxMar17PDE5Image-300x400.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-03-08 13:31:172017-06-07 13:44:49PDE-5 inhibitors for pediatric hypertension
A leading researcher at Children’s National says researchers should look closely at the increased risks of obesity and thyroid disease common in patients with Down Syndrome, and determine how these long term comorbidities relate to cardiovascular and metabolic (cardiometabolic) risk, body image, and quality of life.
Over the last several decades, physicians’ improved ability to treat the common comorbidities of Down syndrome, such as congenital heart disease, has dramatically prolonged survival. Today, more than 400,000 people across the country are living with Down syndrome, and life expectancy has increased to 60 years.
New strategies to manage care for patients with Down syndrome must include preventive, evidence-based approaches to address the unique needs of these patients, according to Sheela N. Magge, M.D., M.S.C.E., Director of Research in the Division of Endocrinology and Diabetes at Children’s. She says that these efforts should include looking more closely at the increased risks of obesity and thyroid disease common in this population, and determining how these long term comorbidities relate to cardiovascular and metabolic (cardiometabolic) risk, body image, and quality of life.
An NIH-funded study from Children’s National and the Children’s Hospital of Philadelphia (CHOP), led by Dr. Magge and her colleague from CHOP, Dr. Andrea Kelly, seeks to better understand how the body composition of patients with Down syndrome impacts their likelihood for developing diabetes and obesity-related cardiovascular risks long term.
“We know that individuals with Down syndrome are at increased risk for obesity, but what hasn’t been clear is whether or not they also have the same cardiometabolic risk associated with obesity that we know holds true for other populations,” says Dr. Magge. “In this previously under-studied population, the common assumption based on very limited studies from the 1970’s was that individuals with Down syndrome were protected from the diabetes and cardiovascular risks that can develop in other overweight people. However, more recent epidemiologic studies contradict those early findings.”
The study has enrolled 150 Down syndrome patients and almost 100 controls to date, and the team is currently beginning to analyze the data. Dr. Magge believes that the findings from this study will help to provide new, research-driven evidence to inform the long term clinical management of obesity and cardiometabolic risk in adolescents with Down syndrome.
She concludes, “The goal is for our research to provide the foundation that will advance prevention and treatment strategies for this understudied group, so that individuals with Down syndrome not only have a longer life expectancy, but also a healthier and better quality of life.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/Heartpic-e1496346745489.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-24 11:09:172018-01-03 11:39:08Illuminating cardiometabolic risk in Down syndrome
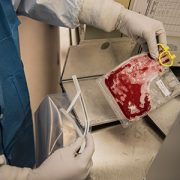
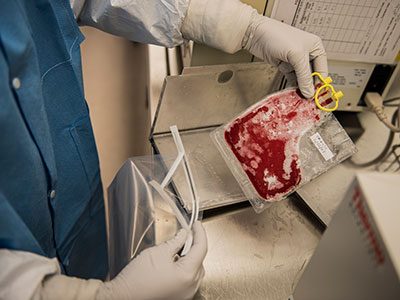
A unique immunotherapeutic approach that expands the pool of donor-derived lymphocytes (T-cells) that react and target three key tumor-associated antigens (TAA) is demonstrating success at reducing or eliminating acute leukemias and lymphomas when these cancers have relapsed following hematopoietic stem cell transplant (HSCT).
“There’s currently a less than 10 percent chance of survival for a child who relapses leukemia or lymphoma after a bone marrow transplant—in part because these patients are in a fragile medical condition and can’t tolerate additional intense therapy,” says Kirsten Williams, M.D., a blood and marrow transplant specialist in the Division of Hematology at Children’s National Health System, and principal investigator of the Research of Expanded multi-antigen Specifically Oriented Lymphocytes for the treatment of VEry High Risk Hematopoietic Malignancies (RESOLVE) clinical trial.
The unique manufactured donor-derived lymphocytes used in this multi-institutional Phase 1 dose-ranging study are receptive to multiple tumor-associated antigens within the cell, including WT1, PRAME, and Survivin, which have been found to be over-expressed in myelodysplastic syndromes (MDS), acute myeloid leukemia (AML), B-cell AML/MDS, B-cell acute lymphoblastic leukemia (ALL), and Hodgkins lymphoma. Modifying the lymphocytes for several antigens, rather than a single target, broadens the ability of the T-cells to accurately target and eradicate cancerous cells.
Preliminary results demonstrate a 78 percent response rate to treatment, and a 44 percent rate of total remission for participating patients. To date, nine evaluable patients with refractory and relapsed AML/MDS, B-cell ALL, or Hodgkins lymphoma have received 1-3 infusions of the expanded T-cells, and of those, seven have responded to the treatment, showing reduction in cancer cells after infusion with little or no toxicity. All of these patients had relapse of their cancer after hematopoietic cell transplantation. The study continues to recruit eligible patients, with the goal of publishing the full study results within the next 12 months.
“Our preliminary data also shows that this new approach has few if any side effects for the patient, in part because the infused T-cells target antigens that are found only in cancer cells and not found in healthy tissues,” Dr. Williams notes.
The approach used to expand existing donor-derived TAA-lymphocytes, rather than using unselected T cells or genetically modified T-cells as in other trials, also seems to reduce the incidence of post infusion graft versus host disease and other severe inflammatory side effects. Those side effects typically occur when the infused lymphocytes recognize healthy tissues as foreign and reject them or when the immune system reacts to the modified elements of the lymphocytes, she adds.
“These results are exciting because they may present a truly viable option for the 30 to 40 percent of children who will relapse post-transplant,” Dr. Williams concludes. “Many of the patients who participated were given two options: palliative care or this trial. To see significant success and fewer side effects gives us, and families with children facing relapsing leukemia, some hope for this new treatment.”
Dr. Williams discussed the early outcomes of the RESOLVE trial during an oral presentation at the American Society for Blood and Marrow Transplantation meeting on February 22, 2017.
“The early indicators are very promising for this patient population,” says Catherine Bollard, M.D., M.B.Ch.B., Chief of the Division of Allergy and Immunology, Director of the Program for Cell Enhancement and Technologies for Immunotherapy (CETI) at Children’s National, and senior author of the study. “If we can achieve this, and continue to see good responses with few side effects, it’s possible these methods could become a viable alternative to HSCT for patients with no donor match or who aren’t likely to tolerate transplant.”
This is one of the first immunotherapeutic approaches to successfully capitalize on the natural ability of human T-cells to kill cancer, though previous research has shown significant success for this approach in reducing the deadly impact of several viruses, including Epstein-Barr virus, adenovirus, and cytomegalovirus, post HSCT. These new findings have led to the development of additional clinical trials to investigate applications of this method of TAA-lymphocyte manufacture and infusion for pre-HSCT MDS/AML, B-cell ALL, Hodgkins Lymphoma, and even some solid tumors.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/Cord-blood.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-24 10:44:072019-08-21 14:00:41T-cell therapy success for relapsing blood cancer
The ICMR team who performed the livestream procedure during the member assembly session. The prestigious invitation came as a result of the innovative partnership between Children’s National and the NHLBI to form the Interventional Cardiac MR Program.
Cardiologists from the Interventional Cardiac Magnetic Resonance (ICMR) Program at Children’s successfully live streamed a right heart catheterization procedure guided by magnetic resonance (MR) imaging during the Member Assembly Session of the Society for Cardiac Magnetic Resonance Scientific Session in early February.
The ICMR program is a first-in-the-nation partnership between Children’s National and the National Heart, Lung, and Blood Institute that features a state-of-the-art dedicated cardiac specific MRI suite for diagnosis, evaluation and intervention for children with heart conditions. The program’s goal is to advance diagnostic and interventional cardiac magnetic resonance imaging techniques in pediatric cardiology and for adults with congenital heart disease. ICMR is cross-disciplinary, connecting researchers, clinicians, engineers and physicists to provide more precise and less invasive diagnostics and treatment options that also reduce radiation exposure for vulnerable patients.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-09 14:10:592018-11-13 09:18:15MR-guided right heart catheterization live streams at SCMR scientific sessions
The cover of Science Translational Medicine features a new study of the cellular-level changes in the brain induced by congenital heart disease. Reprinted with permission from AAAS. Not for download
Disruptions in cerebral oxygen supply caused by congenital heart disease have significant impact on cortical growth, according to a research led by Children’s National Health System. The findings of the research team, which include co-authors from the National Institutes of Health, Boston Children’s Hospital and Johns Hopkins School of Medicine, appear on the cover of Science Translational Medicine. The subventricular zone (SVZ) in normal newborns’ brains is home to the largest stockpile of neural stem/progenitor cells, with newly generated neurons migrating from this zone to specific regions of the frontal cortex and differentiating into interneurons. When newborns experience disruptions in cerebral oxygen supply due to congenital heart disease, essential cellular processes go awry and this contributes to reduced cortical growth.
The preliminary findings point to the importance of restoring these cells’ neurogenic potential, possibly through therapeutics, to lessen children’s long-term neurological deficits.
“We know that congenital heart disease (CHD) reduces cerebral oxygen at a time when the developing fetal brain most needs oxygen. Now, we are beginning to understand the mechanisms of CHD-induced brain injuries at a cellular level, and we have identified a robust supply of cells that have the ability to travel directly to the site of injury and potentially provide help by replacing lost or damaged neurons,” says Nobuyuki Ishibashi, M.D., Director of the Cardiac Surgery Research Laboratory at Children’s National, and co-senior study author.
The third trimester of pregnancy is a time of dramatic growth for the fetal brain, which expands in volume and develops complex structures and network connections that growing children rely on throughout adulthood. According to the National Heart, Lung, and Blood Institute, congenital heart defects are the most common major birth defect, affecting 8 in 1,000 newborns. Infants born with CHD can experience myriad neurological deficits, including behavioral, cognitive, social, motor and attention disorders, the research team adds.
Cardiologists have tapped noninvasive imaging to monitor fetal hearts during gestation in high-risk pregnancies and can then perform corrective surgery in the first weeks of life to fix damaged hearts. Long term neurological deficits due to immature cortical development also have emerged as major challenges in pregnancies complicated by CHD.
“I think this is an enormously important paper for surgeons and for children and families who are affected by CHD. Surgeons have been worried for years that the things we do during corrective heart surgery have the potential to affect the development of the brain. And we’ve learned to improve how we do heart surgery so that the procedure causes minimal damage to the brain. But we still see some kids who have behavioral problems and learning delays,” says Richard A. Jonas, M.D., Chief of the Division of Cardiac Surgery at Children’s National, and co-senior study author. “We’re beginning to understand that there are things about CHD that affect the development of the brain before a baby is even born. What this paper shows is that the low oxygen level that sometimes results from a congenital heart problem might contribute to that and can slow down the growth of the brain. The good news is that it should be possible to reverse that problem using the cells that continue to develop in the neonate’s brain after birth.”
Among preclinical models, the spatiotemporal progression of brain growth in this particular model most closely parallels that of humans. Likewise, the SVZ cytoarchitecture of the neonatal preclinical model exposed to hypoxia mimics that of humans in utero and shortly after birth. The research team leveraged CellTracker Green to follow the path traveled by SVZ derived cells and to illuminate their fate, with postnatal SVZ supplying the developing cortex with newly generated neurons. SVZ derived cells were primarily neuroblasts. Superparamagnetic iron oxide nanoparticles supplied answers about long term SVZ migration, with SVZ derived cells making their way to the prefrontal cortex and the somatosensory cortex of the brain.
“We demonstrated that in the postnatal period, newly generated neurons migrate from the SVZ to specific cortices, with the majority migrating to the prefrontal cortex,” says Vittorio Gallo, Ph.D., Director of the Center for Neuroscience Research at Children’s National, and co-senior study author. “Of note, we revealed that the anterior SVZ is a critical source of newborn neurons destined to populate the upper layers of the cortex. We challenged this process through chronic hypoxia exposure, which severely impaired neurogenesis within the SVZ, depleting this critical source of interneurons.”
In the preclinical model of hypoxia as well as in humans, brains were smaller, weighed significantly less and had a significant reduction in cortical gray matter volume. In the prefrontal cortex, there was a significant reduction in white matter neuroblasts. Taken as a whole, according to the study authors, the findings suggest that impaired neurogenesis within the SVZ represents a cellular mechanism underlying hypoxia induced, region specific reduction in immature neurons in the cortex. The prefrontal cortex, the region of the brain that enables such functions as judgment, decision making and problem solving, is most impacted. Impairments in higher order cognitive functions involving the prefrontal cortex are common in patients with CHD.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/01/CHD-Impaired-Cortical-Growth-HP.jpg248400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-07 14:08:072024-09-06 15:05:20Congenital heart disease and cortical growth
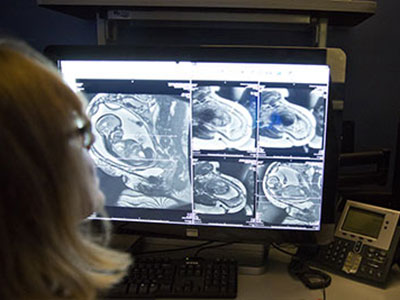
By adding antroduodenal manometry to the cardiovascular tilt table test, doctors in the GI Motility Program are able to collaborate with cardiologists to treat both cardiovascular and gastroenterological symptoms in children with complex orthostatic intolerance.
Physicians treating pediatric patients with complex orthostatic intolerance issues often face a double whammy – the children exhibit symptoms of their cardiovascular condition, but secondary issues relating to gastrointestinal functions are also common. That’s why cardiologists and gastroenterologists at Children’s National Health System have collaborated in recent years to diagnose and find comprehensive treatment solutions for patients with conditions such as neurally mediated hypotension (NMH) and postural orthostatic tachycardia syndrome (POTS).
Their innovative team approach was highlighted in a study of their first 35 patients from age 10-23, published in the Journal of Pediatric Gastroenterology and Nutrition last fall – patients who experienced relief for multiple symptoms thanks to treatment at Children’s National.
The collaboration is possible because of the advancements in gastroenterological diagnostics here – specifically related to the comprehensive GI Motility testing. While patients with POTS can exhibit an abnormal heart rate, low blood pressure, headaches, fatigue or weight loss, their gastroenterological symptoms like nausea and constipation are often under recognized, says Children’s Director of the Comprehensive GI Motility Program Anil Darbari, M.D., MBA, who co-authored the study with a team including Jeffrey Moak, M.D., Director of the Electrophysiology Program at Children’s.
Through antroduodenal manometry of the stomach and upper small intestine, in combination with the cardiovascular tilt table test, the team has been able to more accurately diagnose and treat these patients.
“We have the ability to do them together, thereby making the connection between these two conditions and providing a path for management or treatment,” Dr. Darbari said.
Typically, by the time he sees these patients, those with complex medical issues have often seen several other gastroenterologists at multiple centers, and have been through a lot. The study found that overall, antroduodenal manometry was abnormal in 26 of 35 (74%) patients either at baseline or during tilt table testing in subjects with orthostatic intolerance. Darbari and his colleagues concluded that upper GI motility studies should always be part of the comprehensive evaluation for this population of patients, because treating the autonomic condition improved their gastroenterological symptoms as well.
What does the future look like for this double-whammy approach?
“We have a cohort of over 100 patients with these issues who have been evaluated using this combined diagnostic approach,” Dr. Darbari said. “This gives the team the knowledge and opportunity to help even more kids, which is very rewarding.”
In addition to comprehensive assessment and medical approaches, Children’s National is home to leaders in minimally invasive laparoscopic and endoscopic diagnostic and corrective procedures that have enabled Children’s GI motility specialists and the teams they collaborate with to offer the next level of comprehensive pediatric medical care.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/GI-Motility-e1492005416682.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-07 10:37:202024-09-06 15:10:38Cardiovascular and GI symptom relief
Although recent advances have greatly improved the survival of children with congenital heart disease, up to 55 percent will be left with injury to their brain’s white matter – an area that is critical for aiding connection and communication between various regions in the brain.
What’s known
Eight of every 1,000 children born each year have congenital heart disease (CHD). Although recent advances have greatly improved the survival of these children, up to 55 percent will be left with injury to their brain’s white matter – an area that is critical for aiding connection and communication between various regions in the brain. The resulting spectrum of neurological deficits can have significant costs for the individual, their family and society. Although studies have demonstrated that white matter injuries due to CHD have many contributing factors, including abnormal blood flow to the fetal brain, many questions remain about the mechanisms that cause these injuries and the best interventions.
What’s new
A Children’s National Health System research team combed existing literature, reviewing studies from Children’s as well as other research groups, to develop an article detailing the current state of knowledge on CHD and white matter injury. The scientists write that advances in neuroimaging – including magnetic resonance imaging, magnetic resonance spectroscopy, Doppler ultrasound and diffusion tensor imaging – have provided a wealth of knowledge about brain development in patients who have CHD. Unfortunately, these techniques alone are unable to provide pivotal insights into how CHD affects cells and molecules in the brain. However, by integrating animal models with findings in human subjects and in postmortem human tissue, the scientists believe that it will be possible to find novel therapeutic targets and new standards of care to prevent developmental delay associated with cardiac abnormalities.
For example, using a porcine model, the Children’s team was able to define a strategy for white matter protection in congenital heart surgery through cellular and developmental analysis of different white matter regions. Another study from Children’s combined rodent hypoxia with a brain slice model to replicate the unique brain conditions in neonates with severe and complex congenital heart disease. This innovative animal model provided novel insights into the possible additive effect of preoperative hypoxia on brain insults due to cardiopulmonary bypass and deep hypothermic circulatory arrest.
The Children’s research team also recently published an additional review article describing the key windows of development during which the immature brain is most vulnerable to CHD-related injury.
Questions for future research
Q: Can we create an animal model that recapitulates the morphogenic and developmental aspects of CHD without directly affecting other organs or developmental processes?
Q: What are the prenatal and neonatal cellular responses to CHD in the developing brain?
Q: What are the molecular mechanisms underlying white matter immaturity and vulnerability to CHD, and how can we intervene?
Q: How can we accurately assess the dynamic neurological outcomes of CHD and/or corrective surgery in animal models?
Q: Prenatal or postnatal insults to the developing brain: which is most devastating in regards to developmental and behavioral disabilities?
Q: How can we best extrapolate from, and integrate, neuroimaging findings/correlations in human patients with cellular/molecular approaches in animal models?
Source: Reprinted from Trends in Neurosciences, Vol. 38/Ed. 6, Paul D. Morton, Nobuyuki Ishibashi, Richard A. Jonas and Vittorio Gallo, “Congenital cardiac anomalies and white matter injury,” pp. 353-363, Copyright 2015, with permission from Elsevier.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/CHD_White_Matter_article-1.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-06 07:39:392017-06-07 14:12:46Congenital heart disease and white matter injury
















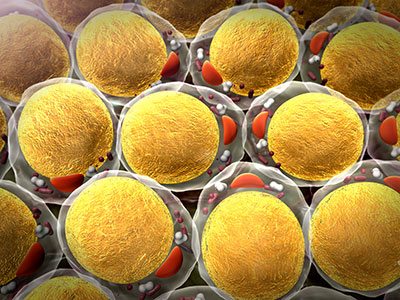
 Dr. Yerebakan comes to Children’s National from the prestigious Pediatric Heart Center in Giessen, Germany, where he was appointed as an Associate Professor of Cardiac Surgery at the Justus-Liebig-University and performed hybrid treatment of hypoplastic left heart syndrome (HLHS). He was deeply involved in mechanical circulatory support and pediatric heart transplantation in Giessen – a leading center for pediatric heart transplantation in Europe. He also served as Chief of Clinical and Experimental Research in the Department of Congenital Cardiac Surgery at Justus-Liebig-University of Giessen, where he acquired several research grants and contributed to more than 20 abstract presentations at national and international meetings and 20 papers in peer-reviewed journals. . Dr. Yerebakan has published approximately 70 scientific papers with more than 160 impact points in three different languages. He is an active reviewer for journals such as the Journal of Thoracic and Cardiovascular Surgery, European Journal of Cardiothoracic Surgery and serves as assistant editor of the Interactive Cardiovascular and Thoracic Surgery journal and Multimedia Manual Cardiothoracic Surgery journal, both of which are official journals of the European Association of Cardiothoracic Surgery. He has had a distinguished academic career and is internationally recognized for his contributions to the field of congenital cardiac surgery, particularly in the treatment of HLHS and novel surgical treatments for heart failure in the pediatric population. Prior to his tenure at Pediatric Heart Center, Dr. Yerebakan completed his fellowship at Children’s in 2011.
Dr. Yerebakan comes to Children’s National from the prestigious Pediatric Heart Center in Giessen, Germany, where he was appointed as an Associate Professor of Cardiac Surgery at the Justus-Liebig-University and performed hybrid treatment of hypoplastic left heart syndrome (HLHS). He was deeply involved in mechanical circulatory support and pediatric heart transplantation in Giessen – a leading center for pediatric heart transplantation in Europe. He also served as Chief of Clinical and Experimental Research in the Department of Congenital Cardiac Surgery at Justus-Liebig-University of Giessen, where he acquired several research grants and contributed to more than 20 abstract presentations at national and international meetings and 20 papers in peer-reviewed journals. . Dr. Yerebakan has published approximately 70 scientific papers with more than 160 impact points in three different languages. He is an active reviewer for journals such as the Journal of Thoracic and Cardiovascular Surgery, European Journal of Cardiothoracic Surgery and serves as assistant editor of the Interactive Cardiovascular and Thoracic Surgery journal and Multimedia Manual Cardiothoracic Surgery journal, both of which are official journals of the European Association of Cardiothoracic Surgery. He has had a distinguished academic career and is internationally recognized for his contributions to the field of congenital cardiac surgery, particularly in the treatment of HLHS and novel surgical treatments for heart failure in the pediatric population. Prior to his tenure at Pediatric Heart Center, Dr. Yerebakan completed his fellowship at Children’s in 2011. Dr. Ramakrishnan joined Children’s National as a fellow in 2014 after completing his fellowship in congenital cardiac surgery at two major centers in Australia. After his two-year fellowship at Children’s, he joined the faculty. Dr. Ramakrishnan has extensive experience in managing children with congenital heart disease. Apart from routine open heart procedures, he has a special expertise in extracorporeal membrane oxygenation (ECMO) procedures and patent ductus arteriosus (PDA) ligation in extremely premature babies. He also has a keen interest in studying clinical outcomes after pediatric heart surgery. His research projects have included analysis of the United Network of Organ Sharing (UNOS) and the Pediatric Health Information System® (PHIS) databases, and his research has resulted in numerous presentations at national and international meetings. Dr. Ramakrishnan is currently the principal investigator at Children’s National for the Pediatric Heart Transplant Study (PHTS) group and the study coordinator for the Congenital Heart Surgeons’ Society (CHSS) studies. He also is a member of the PHTS working group on the surveillance and diagnosis of cellular rejection, and his clinical studies have resulted in several publications in top peer-reviewed journals.
Dr. Ramakrishnan joined Children’s National as a fellow in 2014 after completing his fellowship in congenital cardiac surgery at two major centers in Australia. After his two-year fellowship at Children’s, he joined the faculty. Dr. Ramakrishnan has extensive experience in managing children with congenital heart disease. Apart from routine open heart procedures, he has a special expertise in extracorporeal membrane oxygenation (ECMO) procedures and patent ductus arteriosus (PDA) ligation in extremely premature babies. He also has a keen interest in studying clinical outcomes after pediatric heart surgery. His research projects have included analysis of the United Network of Organ Sharing (UNOS) and the Pediatric Health Information System® (PHIS) databases, and his research has resulted in numerous presentations at national and international meetings. Dr. Ramakrishnan is currently the principal investigator at Children’s National for the Pediatric Heart Transplant Study (PHTS) group and the study coordinator for the Congenital Heart Surgeons’ Society (CHSS) studies. He also is a member of the PHTS working group on the surveillance and diagnosis of cellular rejection, and his clinical studies have resulted in several publications in top peer-reviewed journals.