Children’s National to test bionic pancreas
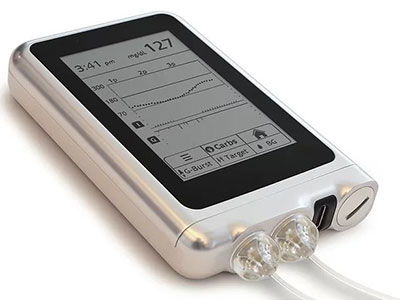
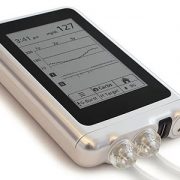
The iLet bionic pancreas helps patients manage their diabetes by both monitoring blood glucose levels and administering insulin and glucagon.
The final results of this clinical trial were published on September 29, 2022 in the New England Journal of Medicine.
Children’s National Hospital has been selected to participate in a multi-center clinical trial to test the efficacy of the iLet bionic pancreas — a device that automatically regulates blood sugar levels in patients with Type 1 diabetes.
Patients generally manage diabetes by constantly monitoring their blood sugar levels and administering insulin when necessary. Unfortunately, too much insulin can cause hypoglycemia, or low blood sugar, which can result in hypoglycemic seizures, coma or rarely, death. Thus, it is extremely important for people with diabetes to regulate their insulin dosages and maintain their blood sugar levels within a range decided by the family and diabetes team.
“The burden of caring for diabetes on a daily basis is grueling,” says Seema Meighan, FNP, a nurse practitioner involved in the upcoming clinical trial. “It is by far one of the most challenging chronic diseases to manage, and requires vigilant participation 100 percent of the time to stay well controlled.”
The iLet bionic pancreas helps patients manage their diabetes by both monitoring blood glucose levels and administering insulin and glucagon — a pancreatic hormone that raises blood sugar levels.
“In a traditional infusion pump, patients only have access to insulin to control glucose levels,” explains Meighan. “This can become problematic when it comes to hypoglycemia. The hope with a bi-hormonal system is that glucagon can be delivered during times that the glucose is low in order to stabilize levels without user interaction.”
Developed at Boston University by Edward Damiano, Ph.D., and Firas El-Khatib, Ph.D., the iLet is a hand-held device about the size of an iPhone but twice as thick, and can easily fit into a pocket. The unit consists of a dual chamber infusion pump that can be configured to deliver only insulin, only glucagon or both hormones. The device uses a wireless glucose sensor on the patient’s body to test blood sugar levels every five minutes. It then determines which hormone is needed and administers it via catheters connected to the patient.
In short-term studies, the iLet was able to maintain blood glucose levels close to normal in both adults and children in carefully controlled environments.
In 2016, the Children’s National Hospital Division of Endocrinology and Diabetes, led by diabetologist Fran Cogen, M.D., C.D.C.E.S., was one of several pediatric sites that were selected to participate in pivotal clinical trials to further test the efficacy of the bionic pancreas. In June 2020, the team at Children’s National began enrolling patients to test iLet devices that only deliver insulin. Once these initial studies are completed, the team will perform an additional trial to test iLet devices configured to deliver both insulin and glucagon.
“This trial is important as it represents the first dual chamber pump to manage glucose levels,” says Meighan. “It could potentially change the way we treat diabetes entirely. It represents a hope to our patients and families that one day this disease will have far less of a daily burden than it currently does.”
Currently, there are 18 patients enrolled in the clinical trial. An initial test run on two patients was successfully completed in November 2020. In early January 2021, the first patient was started on the bionic pancreas to begin the randomized controlled study and three additional patients, who completed the screening process, will join the study shortly. The screening and initiation of the study will continue in the remaining patients.