Nobuyuki Ishibashi, M.D., is the principal investigator on a $3.2 million NIH R01 to study white matter growth and repair in utero for fetal brains affected by congenital heart disease.
Many of the neurological deficits seen in children with congenital heart disease (CHD) are related to abnormal white matter development early in life caused by reduced oxygen supply to the brain while in utero. Children with immature white matter at birth also commonly sustain additional white matter injuries following cardiac surgery.
The research, titled “White matter protection in the fetus with congenital heart disease,” looks specifically at whether providing a supplemental amount of the naturally occurring tetrahydrobiopterin (BH4) for pregnant women could rescue white matter development of fetuses with congenital heart disease whose brains aren’t receiving enough oxygen – or suffering from hypoxic-ischemic events.
Previous preclinical studies have shown that this lack of oxygen depletes the brain’s natural BH4 level, and the researchers hypothesize that BH4 levels play a critical role in the growth and development of white matter in the fetal brain by triggering key cellular/molecular processes. Specifically, the study will focus on three aims:
Establish in a preclinical model the optimal protective regiment for women pregnant with a fetus who has CHD to receive BH4.
Determine the appropriate approach to deliver BH4 to this population
Leverage genetic tools and biochemical techniques in the laboratory to better understand where and how BH4 levels play a role in the growth (or lack thereof) of oligodendrocytes—the primary cells of white matter.
This laboratory-based work is the first step to determining if the neurodevelopment of babies born with CHD can be preserved or recovered by addressing key brain development that occurs before the baby is even born. Findings related to congenital heart disease may also translate to other populations where white matter development is affected by hypoxia-ischemia, including premature infants.
The project is led by principal investigator Nobuyuki Ishibashi, M.D., with co-investigators Vittorio Gallo, Ph.D., Joseph Scafidi, D.O., and Mary Donofrio, M.D. as well as colleagues at MedStar Washington Hospital Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/06/Nobuyuki-Ishibashi.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-06-11 15:34:522023-09-18 11:52:59R01 grant funds white matter protection study for congenital heart disease
Late in pregnancy, the human body carefully prepares fetuses for the rigors of life outside the protection of the womb. Levels of cortisol, a stress hormone, ramp up and spike during labor. Catecholamines, another stress hormone, also rise at birth, helping to kick start the necessary functions that the baby will need to regulate breathing, heartbeat, blood pressure and energy metabolism levels at delivery. Oxytocin surges, promoting contractions for the mother during labor and stimulating milk production after the infant is born.
These processes also can play a role in preparing the fetal brain during the transition to life outside the womb by readying the autonomic nervous system and adapting its cerebral connections. The autonomic nervous system acts like the body’s autopilot, taking in information it needs to ensure that internal organs run steadily without willful action, such as ensuring the heart beats and eyelids blink at steady intervals. Its yin, the sympathetic division, stimulates body processes while its yang, the parasympathetic division, inhibits them.
Infants born preterm have reduced autonomic function compared with their full-term peers and also face possible serious neurodevelopmental impairment later in life. But is there a difference in autonomic nervous system function for full-term babies after undergoing labor compared with infants delivered via cesarean section (C-section)?
A team from the Children’s National Inova Collaborative Research Program (CNICA) – a research collaboration between Children’s National in Washington, D.C., and Inova Women’s and Children’s Hospital in Virginia – set out to answer that question in a paper published online July 30, 2019, in Scientific Reports.
They enrolled newborns who had experienced normal, full-term pregnancies and recorded their brain function and heart performance when they were about 2 days old. Infants whose conditions were fragile enough to require observation in the neonatal intensive care unit were excluded from the study. Of 167 infants recruited for the prospective cohort study, 118 newborns had sufficiently robust data to include them in the research. Of these newborns:
62 (52.5%) were born by vaginal delivery
22 (18.6%) started out with vaginal delivery but ultimately switched to C-section based on failure to progress, failed labor induction or fetal intolerance to labor
And 34 (28.8%) were born by elective C-section.
The CNICA research team swaddled infants for comfort and slipped electrode nets over their tiny heads to simultaneously measure heart rate variability and electrocortical function through non-invasive techniques. The team hypothesized that infants who had been exposed to labor would have enhanced autonomic tone and higher cortical electroencephalogram (EEG) power than babies born via C-section.
“In a low-risk group of babies born full-term, the autonomic nervous system and cortical systems appear to function well regardless of whether infants were exposed to labor prior to birth,” says Sarah B. Mulkey, M.D., Ph.D., a fetal–neonatalneurologist in the Division of Fetal and Transitional Medicine at Children’s National and the study’s lead author.
However, infants born by C-section following a period of labor had significantly increased accelerations in their heart rates. And the infants born by C-section during labor had significantly lower relative gamma frequency EEG at 25.2 hours old compared with the other two groups studied.
“Together these findings point to a possible increased stress response and arousal difference in infants who started with vaginal delivery and finished delivery with C-section,” Dr. Mulkey says. “There is so little published research about the neurologic impacts of the mode of delivery, so our work helps to provide a normal reference point for future studies looking at high-risk infants, including babies born preterm.”
Because the research team saw little differences in autonomic tone or other EEG frequencies when the infants were 1 day old, future research will explore these measures at different points in the newborns’ early life as well as the role of the sleep-wake cycle on heart rate variability.
In addition to Dr. Mulkey, study co-authors include Srinivas Kota, Ph.D., Rathinaswamy B. Govindan, Ph.D., Tareq Al-Shargabi, MSc, Christopher B. Swisher, BS, Laura Hitchings, BScM, Stephanie Russo, BS, Nicole Herrera, MPH, Robert McCarter, ScD, and Senior Author Adré J. du Plessis, M.B.Ch.B., MPH, all of Children’s National; and Augustine Eze Jr., MS, G. Larry Maxwell, M.D., and Robin Baker, M.D., all of Inova Women’s and Children’s Hospital.
Financial support for research described in this post was provided by the National Institutes of Health National Center for Advancing Translational Sciences under award numbers UL1TR001876 and KL2TR001877.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/02/Smiling-baby-boy.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-07-30 15:51:352024-06-05 11:53:17Autonomic nervous system appears to function well regardless of mode of childbirth
Research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that genetic mutations that cause cleft lip and palate also may contribute to neural tube defects, such as spina bifida.
Oral clefts are some of the most common birth defects worldwide, affecting about one in every 700 births. In the U.S., more than 4,000 babies are born each year with cleft lip, with or without cleft palate.
This defect isn’t simply a cosmetic manner: Oral clefts can severely affect feeding, speech and hearing, and they cause about 3,300 deaths annually worldwide.
To better understand these conditions, researchers have isolated a number of genetic mutations that appear to play contributing roles. These include those in a gene known as Interferon Regulatory Factor 6. New research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that these mutations also may contribute to neural tube defects such as spina bifida.
In the first weeks of fetal development, the neural plate curves, creating a neural tube that, once fused shut, becomes the fetal brain and fetal spinal cord. Neural tube defects, which can range from mild to severe, are characterized by incomplete development of the brain, spinal cord or meninges. These defects can potentially result in paralysis or even fetal or neonatal demise. According to the National Institutes of Health, spina bifida, which affects the spinal cord, is the most common neural tube defect in the U.S., affecting up to 2,000 infants each year.
“Despite its high frequency, spina bifida remains among the least understood structural birth defects,” says Brian C. Schutte, an associate professor of Microbiology and Molecular Genetics, Pediatrics and Human Development at Michigan State University and the study’s senior author. “There is strong evidence that genetic factors are a leading cause of such structural birth defects, but in most cases, the cause is unknown. Our team’s study is the first published research to demonstrate that DNA variants in the gene IRF6 can cause spina bifida,” Schutte says.
What’s more, the research team identified a mechanism to explain how altering IRF6 leads to neural tube defects. This mechanism links IRF6 function to two other genes – known as transcription Factor AP2A (TFAP2A) and Grainyhead Like 3 (GRHL3) – that are also known to be required for the development of the neural tube, lip and palate.
“We’re all on the hunt for the reasons when, how and why birth defects happen,” adds Youssef A. Kousa, MS, D.O., Ph.D., a clinical fellow in the Division of Child Neurology at Children’s National Health System and the study’s lead author. “Our main goal is prevention. This paper is a significant development because our team has identified a group of genes that can potentially contribute to very common types of birth defects: craniofacial as well as neural tube defects.”
The scientific odyssey is a wonderful example of serendipity. Kousa, then working in Schutte’s lab, was studying the effects of a new mutant experimental model strain on development of the palate. But one day, he walked into Schutte’s office holding a deformed preclinical embryo and said: “Brian, look at this!”
“Weird things happen in biology,” Schutte replied and counseled him to return if it happened again. Less than two weeks later, Kousa was back with several more of the deformed preclinical embryos, saying: “OK, Brian. It happened again.”
Within hours Kousa had unearthed recently published research that included an image of a similarly affected preclinical embryo. The pair then sketched out possible intersecting genetic pathways, as they brainstormed the myriad ways to end up with that specific phenotype. Initially, they tested their hypotheses in experimental models and eventually corroborated findings through human genetic studies.
The human studies could only be performed by collaborations. Schutte shared their initial observations with human genetics researchers scattered across the country. Those labs then generously agreed to test whether DNA variants in IRF6 were associated with neural tube defects in samples from patients that they had collected over decades of research.
The team found that Tfap2a, Irf6 and Grhl3 are components of a gene regulatory network required for neurulation, a folding process that results in the neural tube bending and then fusing to become the basis of the embryo’s nervous system, from brain to spinal cord.
“Since this network is also required for formation of the lip, palate, limbs and epidermis, which develop at different times and places during embryogenesis, we suggest that the Tfap2a–Irf6–Grhl3 network is a fundamental pathway for multiple morphogenetic processes,” the researchers write.
Interferon Regulatory Factor 6 functions best when there is neither too much expression nor too little. Overexpression of Irf6 suppresses Transcription Factor Activation Protein 2A and Grainyhead Like 3, causing exencephaly, a neural tube defect characterized by the brain being located outside of the skull. Counterintuitively, experimental models that had too little Irf6 also ended up with reduced levels of Tfap2a and Grhl3 that led to a structural birth defect, but at the opposite end of the neural tube.
To test whether the experimental model findings held true in humans, they sequenced samples from people who had spina bifida and anencephaly – the rare birth defect that Kousa spotted in the experimental models – and found IRF6 function was conserved in people. Because of the genetic complexity of these birth defects, and the challenges inherent in collecting samples from cases of severe birth defects, many research teams were invited to participate in the study.
As testament to their collegiality, researchers from Stanford University, University of Texas at Austin, University of Iowa, University of Texas at Houston and Duke University agreed to share precious samples from the California Birth Defects Monitoring Program, from the Hereditary Basis of Neural Tube Defects study and from their own institutional sample collections.
“As we get better at personalized medicine, we could use this information to one day help to counsel families about their own risk and protective factors,” Kousa adds. “If we can identify the genetic pathway, we might also be able to modify it to prevent a birth defect. For example, prenatal supplementation with folic acid has led to a decrease in babies born with neural tube defects, but not all neural tube defects are sensitive to folic acid. This knowledge will help us develop individual-based interventions.”
Financial support for the research covered in this post was provided by the National Institutes of Health under grants DE13513, F31DE022696, DE025060, P01HD067244 and GM072859; startup funding from Michigan State University and the UT-Health School of Dentistry in Houston; and the Centers for Disease Control and Prevention under award number 5U01DD001033.
In addition to Kousa and Schutte, study co-authors include Huiping Zhu, Yunping Lei and Richard H. Finnell, University of Texas at Austin; Walid D. Fakhouri, University of Texas Health Science Center at Houston; Akira Kinoshita, Nagasaki University; Raeuf R. Roushangar, Nicole K. Patel, Tamer Mansour, Arianna L. Smith, and Dhruv B. Sharma, Michigan State University; A.J. Agopian and Laura E. Mitchell, University of Texas School of Public Health; Wei Yang and Gary M. Shaw, Stanford University School of Medicine; Elizabeth J. Leslie, Emory University; Xiao Li, Tamara D. Busch, Alexander G. Bassuk and Brad A. Amendt, University of Iowa; Edward B. Li and Eric C. Liao, Massachusetts General Hospital; Trevor J. Williams, University of Colorado Denver at Anschutz Medical Campus; Yang Chai, University of Southern California; and Simon Gregory and Allison Ashley-Koch, Duke University Medical Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/little-girl-with-spina-bifida.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-25 12:58:112024-12-30 12:46:57Oral clefts may stem from a shared genetic cause as neural tube defects
During the last few weeks of pregnancy, certain regions of the fetal brain experience exponential growth but also are more vulnerable to injury during that high-growth period.
Yao Wu, Ph.D., a research postdoctoral fellow in the Developing Brain Research Laboratory at Children’s National Health System, has received a Thrasher Research Fund early career award to expand knowledge about regions of the fetal brain that are vulnerable to injury from congenital heart disease (CHD) during pregnancy.
CHD, the most common birth defect, can have lasting effects, including overall health issues; difficulty achieving milestones such as crawling, walking or running; and missed days at daycare or school, according to the Centers for Disease Control and Prevention. Brain injury is a major complication for infants born with CHD. Catherine Limperopoulos, Ph.D., director of Children’s brain imaging lab, was the first to provide in vivo evidence that fetal brain growth and metabolism in the third trimester of pregnancy is impaired within the womb.
“It remains unclear which specific regions of the fetal brain are more vulnerable to these insults in utero,” Limperopoulos says. “We first need to identify early brain abnormalities attributed to CHD and understand their impact on infants’ later behavioral and cognitive development in order to better counsel parents and effectively intervene during the prenatal period to safeguard brain health.”
During the last few weeks of pregnancy, certain regions of the fetal brain experience exponential growth but also are more vulnerable to injury during that high-growth period. The grant, $26,749 over two years, will underwrite “Brain Development in Fetuses With Congenital Heart Disease,” research that enables Wu to utilize quantitative, non-invasive magnetic resonance imaging (MRI) to compare fetal brain development in pregnancies complicated by CHD with brain development in healthy fetuses of the same gestational age.Wu will leverage quantitative, in vivo 3-D volumetric MRI to compare overall fetal and neonatal brain growth as well as growth in key regions including cortical grey matter, white matter, deep grey matter, lateral ventricles, external cerebrospinal fluid, cerebellum, brain stem, amygdala and the hippocampus.
The research is an offshoot of a prospective study funded by the National Institutes of Health that uses advanced imaging techniques to record brain growth in 50 fetuses in pregnancies complicated by CHD who need open heart surgery and 50 healthy fetuses. MRI studies are conducted during the second trimester (24 to 28 weeks gestational age), third trimester (33 to 37 weeks gestational age) and shortly after birth but before surgery. In addition, fetal and neonatal MRI measurements will be correlated with validated scales that measure infants’ and toddlers’ overall development, behavior and social/emotional maturity.
“I am humbled to be selected for this prestigious award,” Wu says. “The findings from our ongoing work could be instrumental in identifying strategies for clinicians and care teams managing high-risk pregnancies to optimize fetal brain development and infants’ overall quality of life.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/02/Pregnant-Mom.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-08-01 12:10:422024-06-05 11:26:31Safeguarding fetal brain health in pregnancies complicated by CHD
Blood is the conduit through which our cells receive much of what they need to grow and thrive. The nutrients and oxygen that cells require are transported by this liquid messenger. Getting adequate blood flow is especially important during the rapid growth of gestation and early childhood – particularly for the brain, the weight of which roughly triples during the last 13 weeks of a typical pregnancy. Any disruption to blood flow during this time could dramatically affect the development of this critical organ.
Now, a new study by Children’s National Health System researchers finds that blood flow to key regions of very premature infants’ brains is altered, providing an early warning sign of disturbed brain maturation well before such injury is visible on conventional imaging. The prospective, observational study was published online Dec. 4, 2017 by TheJournal of Pediatrics.
“During the third trimester of pregnancy, the fetal brain undergoes an unprecedented growth spurt. To power that growth, cerebral blood flow increases and delivers the extra oxygen and nutrients needed to nurture normal brain development,” says Catherine Limperopoulos, Ph.D., director of the Developing Brain Research Laboratory at Children’s National and senior author of the study. “In full-term pregnancies, these critical brain structures mature inside the protective womb where the fetus can hear the mother and her heartbeat, which stimulates additional brain maturation. For infants born preterm, however, this essential maturation process happens in settings often stripped of such stimuli.”
The challenge: How to capture what goes right or wrong in the developing brains of these very fragile newborns? The researchers relied on arterial spin labeling (ASL) magnetic resonance (MR) imaging, a noninvasive technique that labels the water portion of blood to map how blood flows through infants’ brains in order to describe which regions do or do not receive adequate blood supply. The imaging work can be done without a contrast agent since water from arterial blood itself illuminates the path traveled by cerebral blood.
“In our study, very preterm infants had greater absolute cortical cerebral blood flow compared with full-term infants. Within regions, however, the insula (a region critical to experiencing emotion), anterior cingulate cortex (a region involved in cognitive processes) and auditory cortex (a region involved in processing sound) for preterm infants received a significantly decreased volume of blood, compared with full-term infants. For preterm infants, parenchymal brain injury and the need for cardiac vasopressor support both were correlated with decreased regional CBF,” Limperopoulos adds.
The team studied 98 preterm infants who were born June 2012 to December 2015, were younger than 32 gestational weeks at birth and who weighed less than 1,500 grams. They matched those preemies by gestational age with 104 infants who had been carried to term. The brain MRIs were performed as the infants slept.
Blood flows where it is needed most with areas of the brain that are used more heavily commandeering more oxygen and nutrients. Thus, during brain development, CBF is a good indicator of functional brain maturation since brain areas that are the most metabolically active need more blood.
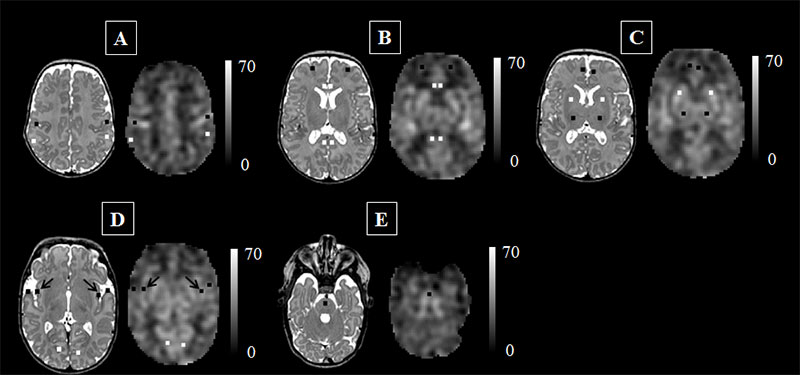
This figure represents the cerebral blood flow (CBF) maps, corresponding anatomical image aligned to the CBF map, and the regions of interest examined. The scale indicates the quantitative value of the CBF map and is expressed in mL/100g/min. The data are from a preterm infant scanned at term age without evidence of brain injury. The insula (see black arrows in panel ‘D’) may be particularly vulnerable to the added stresses of the preterm infant’s life outside the womb. Credit: M. Bouyssi-Kobar, et al., The Journal of Pediatrics.
“The ongoing maturation of the newborn’s brain can be seen in the distribution pattern of cerebral blood flow, with the greatest volume of blood traveling to the brainstem and deep grey matter,” says Marine Bouyssi-Kobar, M.S., the study’s lead author. “Because of the sharp resolution provided by ASL-MR images, our study finds that in addition to the brainstem and deep grey matter, the insula and the areas of the brain responsible for sensory and motor functions are also among the most oxygenated regions. This underscores the critical importance of these brain regions in early brain development. In preterm infants, the insula may be particularly vulnerable to the added stresses of life outside the womb.”
Of note, compromised regional brain structures in adults are implicated in multiple neurodevelopmental disorders. “Altered development of the insula and anterior cingulate cortex in newborns may represent early warning signs of preterm infants at greater risk for long-term neurodevelopmental impairments,” Limperopoulos says.
Research reported in this post was supported by the Canadian Institutes of Health Research, MOP-81116; the SickKids Foundation, XG 06-069; and the National Institutes of Health under award number R01 HL116585-01.
The Children’s National Health System Fetal Medicine Institute hosted the 2nd annual International Symposium on the Fetal Brain in August 2017 in Washington, D.C.
Speakers at this year’s symposium focused on the following four areas:
Brain Development in an Unsupportive In Utero Environment – Diagnosis and Consequences
Supporting Brain Development in the Ex Utero Fetus: How Far Are We From Optimal?
Genomic and Epigenomic Mechanisms Underlying Differences in Brain Development
The Emergence of Consciousness and Pain Sensation
Adré J. du Plessis, M.B.Ch.B., M.P.H., Director of the Fetal Medicine Institute and Division Chief of Fetal and Transitional Medicine hosted the conference. In his opening remarks Dr. du Plessis noted “Our goal has been to gather together a diverse group from across the spectrum of disciplines focused on the well-being of the fetal brain and to engage all disciplines together.”
Diana Bianchi, MD gives her keynote presentation on non-invasive fetal testing at the second annual International Symposium on the Fetal Brain.
Invited, internationally renowned speakers presented on diverse topics, including Diana Bianchi, Director of the Eunice Kennedy Shriver National Institute of Child Health and Human Development who spoke on the “Non-Invasive Fetal Testing Beyond Karyotype: What’s in it for the Fetal Brain?”
A new component to the symposium was the clinically-focused breakfast breakout sessions, created based on feedback from attendees of the 2016 Symposium. Sessions covered varied topics such as “Fetal Ultrasound: the Cornerstone of Fetal Neurodiagnosis,” “The Essentials of Neurogenetic Testing,” “Developing a Transitional Fetal-Neonatal Program” and “Using MRI to Advance Fetal Neurodiagnosis.”
The conference started with an exciting discussion by Alistair Gunn, M.B.Ch.B., Head of the Department of Physiology at the University of Auckland. His presentation “Fetal Heart Rate: What It Does and Does Not Tell Us” explored the considerable body of evidence that essentially all decelerations are mediated by chemoreflex responses to repeated hypoxia and that the parasympathetic autonomic nervous system is the critical regulator of both fetal heart rate and heart rate variation in labor.
For more information about the sessions and speakers at the 2017 Symposium, please visit our website.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/10/Diana-Bianchi-at-ISFB.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-10-17 10:20:372019-05-06 14:11:27Children’s National Fetal Medicine Institute hosts 2nd annual International Symposium on the Fetal Brain
By looking back to the earliest moments of embryonic brain development, Kazue Hashimoto-Torii, Ph.D. and her collaborators sought to explain the molecular and cellular bases for complex congenital brain disorders that can result from exposure to harmful agents.
When the brain is exposed to an environmental stressor all is not immediately lost. Brain cells have mechanisms that protect them against the ravages of alcohol and other toxic substances. One of these is a protein the cells make, known as Heat Shock Factor 1 (Hsf1), which helps to shield them from damage. The fetal brain also can make Hsf1, which protects its particularly vulnerable cells from environmental stressors that pregnant mothers are exposed to during gestation.
However, a new study suggests that this system is not perfect. Research led by Children’s National Health System scientists suggests that when too much Hsf1 is produced, it actually can impair the brain during development. While this finding was made in a preclinical model, it raises questions about neural risks for human infants if their mothers drink alcohol in the first or second trimester of pregnancy.
When fetuses are chronically exposed to harmful agents such as alcohol, ethanol or methyl mercury in utero, the experience can negatively affect fetal brain development in unpredictable ways. Some fetal brains show little or no damage, while others suffer severe damage. By looking at the earliest moments of embryonic brain development, an international research team that includes five Children’s National authors sought to explain the molecular and cellular bases for complex congenital brain disorders that can result from exposure to such harmful agents.
“From a public health perspective, there is ongoing debate about whether there is any level of drinking by pregnant women that is ‘safe,’ ” says Kazue Hashimoto-Torii, Ph.D., principal investigator in the Center for Neuroscience Research at Children’s National and senior author of the paper published May 2 in Nature Communications. “We gave ethanol to pregnant preclinical models and found their offspring’s neural cells experienced widely differing responses to this environmental stress. It remains unclear which precise threshold of stress exposure represents the tipping point, transforming what should be a neuroprotective response into a damaging response. Even at lower levels of alcohol exposure, however, the risk for fetal neural cells is not zero,” Hashimoto-Torii adds.
The cerebral cortex – the thin outer layer of the cerebrum and cerebellum that enables the brain to process information – is particularly vulnerable to disturbances in the womb, the study authors write. To fend off insult, neural cells employ a number of self-preservation strategies, including launching the protective Hsf1-Heat shock protein (Hsp) signaling pathway that is used by a wide range of organisms, from single-cell microbes to humans. Developing fetuses activate Hsf1-Hsp signaling upon exposure to environmental stressors, some to no avail.
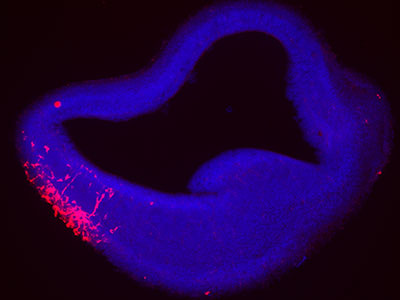
To help unravel the neurological mystery, the researchers used a method that allows a single molecule to fluoresce during stress exposure. They tapped specific environmental stressors, such as ethanol, hydrogen peroxide and methyl mercury – each of which are known to produce oxidative stress at defined concentrations. And, using an experimental model, they examined the Hsf1 activation pattern in the developing cerebral cortex by creating a marker, an encoding gene tagged with a type of fluorescent protein that makes it glow bright red.
“Our results suggest that heterogeneous events of abnormal brain development may occur probabilistically – which explains patterns of cortical malformations that vary with each individual, even when these individuals are exposed to similar levels of environmental stressors,” Hashimoto-Torii adds.
Among the more striking findings, neural cells with excessively high levels of Hsf1-Hsp activation due to ethanol exposure experience disruptions to normal development, with delayed migration by immature cortical neurons. For the fetal brain to develop normally, neurons need to migrate to precise places in the brain at just the right time to enable robust neural connections. When neurons fail to arrive at their destinations or get there too late, there can be gaps in the neural network, compromising efficient and effective communication across the brain’s various regions.
“Even a short period of Hsf1 overactivation during prenatal development causes critical neuronal migration deficiency. The severity of deficiency depends on the duration of Hsf1 overactivation,” Hashimoto-Torii says. “Expression patterns vary, however, across various tissues. Stochastic response within individual cells may be largely responsible for variability seen within tissue and organs.”
The research team found one bright spot: Cortical neurons that stalled due to lack of the microtubule-associated molecule Dcx were able to regain their ability to migrate properly when the gene was replenished after birth. A reduction in Hsf1 activity after birth, however, did not show the same ability to trigger the “reset” button on neural development.
“The finding suggests that genes other than microtubule-associated genes may play pivotal roles in ensuring that migrating neurons reach their assigned destinations in the brain at the right time – despite the added challenge of excessive Hsf1 activation,” according to Hashimoto-Torii.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/05/Kazue-Hashimoto-Torii.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-05-12 09:16:442018-11-05 10:01:01A brain’s protector may also be its enemy
A team led by Children’s National developed a fluorescence reporter system in an experimental model that can single out neurons that have survived prenatal damage but remain vulnerable after birth.
When fetuses are exposed to environmental stressors, such as maternal smoking or alcohol consumption, radiation or too little oxygen, some of these cells can die. A portion of those that survive often have lingering damage and remain more susceptible to further environmental insults than healthy cells; however, researchers haven’t had a way to identify these weakened cells. This lack of knowledge has made it difficult to discover the mechanisms behind pathological brain development thought to arise from these very early environmental exposures, as well as ways to prevent or treat it.
What’s new
A team led by Kazue Hashimoto-Torii, Ph.D., a principal investigator in the Center for Neuroscience Research at Children’s National Health System, developed a marker that makes a protein known as Heat Shock Factor 1 glow red. This protein is produced in cells that become stressed through exposure to a variety of environmental insults. Gestation is a particularly vulnerable time for rapidly dividing nerve cells in the fetal brain. Tests showed that this marker worked not just on cells in petri dishes but also in an experimental model to detect brain cells that were damaged and remained vulnerable after exposure to a variety of different stressors. Tweaks to the system allowed the researchers to follow the progeny of cells that were affected by the initial stressor and track them as they divided and spread throughout the brain. By identifying which neurons are vulnerable, the study authors say, researchers eventually might be able to develop interventions that could slow or stop damage before symptoms arise.
Questions for future research
Q: How do different environmental insults damage brain cells during gestation? Q: How does this damage translate into pathology in organisms as they mature? Q: Do the progeny of damaged brain cells retain the same degree of damage as they divide and spread? Q: Can this new detection system be used to find and track damage in other organs, such as the heart, eye and liver?