
Medical device competition announces six winners to share in $250K
Judges award grants for pediatric medical devices that address cardiovascular, NICU, and orthopaedic and spine device innovations.
Judges award grants for pediatric medical devices that address cardiovascular, NICU, and orthopaedic and spine device innovations.
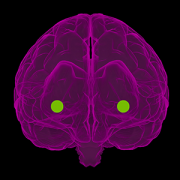
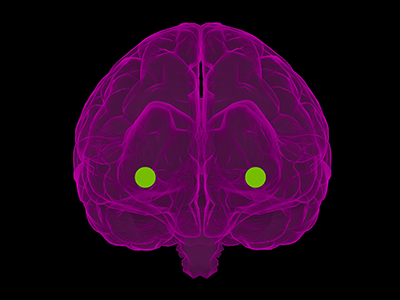
The medial amygdala (MeA) is a region of the brain that modulates innate social and non-social behaviors in several mammals, including humans.
The medial amygdala (MeA) is a region of the brain that modulates innate social and non-social behaviors in several mammals, including humans. Notedly sexually dimorphic, MeA neurons exhibit well-documented sex differences in anatomy, morphology and molecular characteristics. Recently, a pioneer study published in eNeuro from the Children’s National Hospital Center for Neuroscience Research has unveiled new information regarding physiological sex differences in MeA neurons, which, until now, has remained a missing piece in understanding how the MeA codes differently in males and females.
Previous research from Children’s National has shown that two subpopulations of MeA inhibitory output neurons descended from Dbx1 and Foxp2 transcription factors display different responses to innate olfactory cues and in a sex-specific manner. The newest study examines whether these transcription factor defined neurons also possess sex-specific biophysical signatures. The scientists posit that understanding how sex and lineage impact upstream differences at the neuronal level can help illuminate how the MeA processes information and codes for sex-specific behavioral differences.
Using whole-cell patch clamp recording and stepwise current injection, the researchers were able to analyze the intrinsic electrophysiological profiles of the two subclasses of MeA neurons in males and females in a pre-clinical model. Data revealed that the spike frequency of Dbx1-lineage and Foxp2-lineage neurons differed by lineage, sex and stimulus strength. Dbx1-lineage neurons in females discharged more spikes than those in males during high-amplitude current injection, while Foxp2-lineage neurons in females discharged more spikes than those in males during low-amplitude current injection. Across lineage, researchers observed that Dbx1-lineage neurons discharged more spikes than Foxp2-lineage neurons in females, but only at the highest amplitude stimulus, while Dbx1-lineage neurons spiked more than Foxp2-lineage neurons in males during low rather than high-amplitude current injection.
Different spiking patterns are generally indicative of different intrinsic cell properties. However, this study found that the intrinsic properties of the cell – such as membrane potential, resistance, and rheobase – were the same at rest across sex and lineage. The only significant difference was found in capacitance, an electrical measurement that roughly corresponds with cell size. Additionally, the study found that spike frequency adaptation correlated with neuronal lineage and sex, with males having a higher adaptation factor than females and Foxp2-lineage neurons displaying a higher adaptation factor than Dbx1-lineage neurons. In tandem, these results indicated that changes in the intrinsic properties were taking place during stimulation.
The researchers then used waveform phase-plots to visualize phases of the different action potentials and contrived an innovative new method of analyzing these quantitatively instead of solely qualitatively. This allowed them to know that broadly, ion channels that work with repolarization are likely different, and prompted them to focus on the family of ion channels that are known to modify the repolarization phase. From 62 candidate ion channels, the researchers chose 10 to investigate. Experiments ultimately revealed that only one ion channel was found to exhibit statistically significant sex differences in the Foxp2 population. This result indicated that molecular expression of these ion channels are likely driving differences in the physiology of the cells which may be the basis of behavioral expression. Future research topics include how and when sex hormones shape MeA neuronal firing properties and how this relates to network function.
“This is a small piece of contribution to the overall understanding of how the brain as a biological machine codes for different outputs,” says first author Heidi Y. Matos, Ph.D.
By showing sex differences in neural function, this research represents progress in understanding the biological underpinnings of a host of developmental disorders, particularly those diagnosed in different proportions between males and females. Autism spectrum disorders, for example, often have symptoms that manifest through social interaction, and understanding these disorders requires a better understanding of normal MeA physiology.
“In order to get to the why, we have to get to the how of that circuit,” says Dr. Matos.
Just as the brain harnesses the collective power of a diverse range of neurons, the Center for Neuroscience harnesses the aggregate talent of a diverse group of neuroscientists to produce innovative work. This study in particular champions diversity in the sciences, with more than half of the authors coming from underrepresented minorities, including Dr. Matos.
“I think this work is a shining example of the tremendous contributions that are made by neuroscientists from all backgrounds,” says principal investigator Joshua G. Corbin, Ph.D.
“Sex Differences in Biophysical Signatures across Molecularly Defined Medial Amygdala Neuronal Subpopulations” was published in eNeuro. Additional authors include David Hernandez-Pineda, Claire M. Charpentier, Allison Rusk and Kevin S. Jones, Ph.D.


A new review article enumerates some key similarities and differences between MIS-C and Kawasaki disease.
Since May 2020, there has been some attention in the general public and the news media to a specific constellation of symptoms seen in children with COVID-19 or who have been exposed to COVID-19. For a time, headlines even called it a “Kawasaki-like” disease. At first glance, both the symptoms and the effective treatments are remarkably similar. However, a new review published in Trends in Cardiovascular Medicine finds that under closer scrutiny, the two conditions have some interesting differences as well.
“At the beginning of this journey, we thought we might be missing actual cases of Kawasaki disease because we identified a few patients who presented late and developed coronary artery abnormalities,” says Ashraf Harahsheh, M.D., senior author of the review article, “Multisystem inflammatory syndrome in children: Is there a linkage to Kawasaki disease?” and a cardiologist at Children’s National Hospital. “But as time passed, children exposed to COVID-19 started to present with a particular constellation of symptoms that actually had some important similarities and distinctions from Kawasaki.”
Both disease patterns seem to have a common trigger that provokes the inflammatory cascade reaction in genetically susceptible children, the authors write. However, there is also early evidence that children with each disease have different genetic markers, meaning different populations are genetically susceptible to each disease.
Additionally, the authors found that the massive activation of pro-inflammatory cytokines seen in MIS-C, also known as a “cytokine storm,” overlaps with a similar occurrence seen in Kawasaki disease, adult COVID-19 patients, toxic shock syndrome and some other viral infections.
Overall, when compared to Kawasaki disease, children with MIS-C tend to:
Despite noted differences, the authors are also careful to credit the documented similarities between Kawasaki disease and MIS-C as a key to the quick identification of the new syndrome in children. The study of Kawasaki disease also gave clinicians a valid basis to begin developing diagnostic recommendations and treatment protocols.
The review’s first author Yue-Hin Loke, M.D., who is also a cardiologist at Children’s National, says, “The quick recognition of MIS-C is only possible because of meticulous research conducted by Dr. Tomisaku Kawasaki, who recently passed away on June 5th, 2020. Even though some aspects of both are still shrouded in mystery, the previous research and clinical advancements made in Kawasaki disease set the stage for our immediate response to MIS-C.”
“Previous research provided key information for cardiologists facing this new syndrome, including the necessity of routine echocardiograms to watch for coronary artery abnormalities (CAAs) and for use of intravenous immunoglobulin (IVIG) to mitigate the development of CAAs,” says Charles Berul, M.D., chief of Cardiology at Children’s National and a co-author. “Both of these factors have played a key role in reducing the mortality of MIS-C to almost zero.”
The authors note that more research is needed to understand both Kawasaki disease and the specifics of MIS-C, but that what is learned about the mechanisms of one can and should inform study and treatment of the other. And in the meantime, caution and continued surveillance of these patients, especially with respect to coronary artery and myocardial function, will continue to improve the long-term outcomes for both syndromes.


“The more we continue to learn about glioblastoma,” Yuan Zhu, Ph.D., says, “the more hope we can give to these patients who currently have few effective options.”
A pre-clinical model of glioblastoma, an aggressive type of cancer that can occur in the brain, suggests that this recalcitrant cancer originates from a pool of stem cells that can be a significant distance away from the resulting tumors. The findings of a new study, led by Children’s National Hospital researchers and published July 22 in the journal Nature Communications, suggest new ways to fight this deadly disease.
Despite decades of research, glioblastoma remains the most common and lethal primary brain tumor in adults, with a median survival of only 15 months from diagnosis, says study leader Yuan Zhu, Ph.D., the scientific director and endowed professor of the Gilbert Family Neurofibromatosis Institute at Children’s National. Unlike many cancers, which start out as low-grade tumors that are more treatable when they’re caught at an early stage, most glioblastomas are almost universally discovered as high-grade and aggressive lesions that are difficult to treat with the currently available modalities, including surgery, radiation and chemotherapy.
“Once the patient has neurological symptoms like headache, nausea, and vomiting, the tumor is already at an end state, and disease progression is very rapid,” Dr. Zhu says. “We know that the earlier you catch and treat cancers, the better the prognosis will be. But here, there’s no way to catch the disease early.”
However, some recent research in glioblastoma patients shows that the subventricular zone (SVZ) – an area that serves as the largest source of stem cells in the adult brain – contains cells with cancer-driving mutations that are shared with tumors found in other often far-distant brain regions.
To see if the SVZ might be the source for glioblastoma tumors, Dr. Zhu and his colleagues worked with pre-clinical models that carried a single genetic glitch: a mutation in a gene known as p53 that typically suppresses tumors. Mutations in p53 are known to be involved in glioblastoma and many other forms of cancer.
Using genetic tests and an approach akin to those used to study evolution, the researchers traced the cells that spurred both kinds of tumors back to the SVZ. Although both single and multiple tumors had spontaneously acquired mutations in a gene called Pten, another type of tumor suppressor, precursor cells for the single tumors appeared to acquire this mutation before they left the SVZ, while precursor cells for the multiple tumors developed this mutation after they left the stem cell niche. When the researchers genetically altered the animals to shut down the molecular pathway that loss of Pten activates, it didn’t stop cancer cells from forming. However, rather than migrate to distal areas of the brain, these malignant cells remained in the SVZ.
Dr. Zhu notes that these findings could help explain why glioblastoma is so difficult to identify the early precursor lesions and treat. This work may offer potential new options for attacking this cancer. If new glioblastoma tumors are seeded by cells from a repository in the SVZ, he explains, attacking those tumors won’t be enough to eradicate the cancer. Instead, new treatments might focus on this stem cell niche as target for treatment or even a zone for surveillance to prevent glioblastoma from developing in the first place.
Another option might be to silence the Pten-suppressed pathway through drugs, a strategy that’s currently being explored in various clinical trials. Although these agents haven’t shown yet that they can stop or reverse glioblastomas, they might be used to contain cancers in the SVZ as this strategy did in the pre-clinical model — a single location that might be easier to attack than tumors in multiple locations.
“The more we continue to learn about glioblastoma,” Dr. Zhu says, “the more hope we can give to these patients who currently have few effective options.”
Other Children’s National researchers who contributed to this study include Yinghua Li, Ph.D., Wei Li, Ph.D., Yuan Wang, Ph.D., Seckin Akgul, Ph.D., Daniel M. Treisman, Ph.D., Brianna R. Pierce, B.S., Cheng-Ying Ho, M.D. /Ph.D.
This work is supported by grants from the National Institutes of Health (2P01 CA085878-10A1, 1R01 NS053900 and R35CA197701).
“For children who are at risk of losing their vision, this project will bring a window of opportunity for physicians to start treatment earlier and save their vision,” says Marius George Linguraru, DPhil, MA, MSc.
A team from Children’s National Hospital is part of a project receiving a two-year grant of nearly $1,000,000 from the National Institutes of Health (NIH) for the first pediatric project in the Quantitative Imaging Network (QIN) of the National Cancer Institute (NCI). Marius George Linguraru, DPhil, MA, MSc, principal investigator from the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital in Washington, D.C., is one of two principal investigators on the project, which focuses on developing quantitative imaging (QI) tools to improve pediatric tumor measurement, risk predictions and treatment response. Roger Packer, M.D., Senior Vice President of the Center for Neuroscience & Behavioral Health, Director of the Gilbert Neurofibromatosis Institute and Director of the Brain Tumor Institute, is co-investigator.
The project, in collaboration with Children’s Hospital of Philadelphia and Children’s Hospital Colorado, centers on the most common type of brain tumor in children, called a low-grade glioma. This project focuses on a clinically challenging group of children with neurofibromatosis type 1 (NF1), the most common inherited tumor predisposition syndrome. Nearly 20% of children with NF1 will develop a low-grade glioma called optic pathway glioma (OPG). In children with this type of brain tumor, the growth occurs around the optic nerve, chiasm and tracts, also called the optic pathway, which connects the eye to the brain. OPGs can cause vision loss and even blindness. Permanent vision loss usually occurs between one and eight years of age with doctors closely monitoring the tumor with magnetic resonance imaging (MRI) to assess the disease progression.
“Our traditional two-dimensional measures of tumor size are not appropriate to assess the changes in these amorphous tumors over time or how the tumor responds to treatment,” says Linguraru. “This means physicians have difficulty determining the size of the tumor as well as when treatment is working. Research such as this can lead to innovative medical technologies that can improve and possibly change the fate of children’s lives.”
Dr. Linguraru is leading the technical trials on this project, which take place in the first two years, or phase one, starting in June 2020. Phase one focuses on improving the often inaccurate human measurements of tumor size by developing QI tools to make precise and automated measures of tumor volume and shape using machine learning. In this phase, the project will use and homogenize MRI data from multiple centers to develop predictive models of the treatment response based on the tumor volume that are agnostic to the differences in imaging protocols. By doing this, it will allow physicians to make more informed decisions about the treatment’s success and whether the child will recover their vision.
When phase one is complete, Linguraru and the project’s other principal investigator Robert A. Avery, DO, MSCE, neuro-ophthalmologist in the Division of Ophthalmology at Children’s Hospital of Philadelphia, will initiate the second phase, which includes validating the QI application on data from the first ever phase III clinical trial comparing two treatments for NF1-OPGs. Phase two is scheduled to start in the Summer 2022 and continue through Summer 2025.
“For children who are at risk of losing their vision, this project will bring a window of opportunity for physicians to start treatment earlier and save their vision,” says Linguraru. “For those children who won’t benefit from chemotherapy because the tumor poses no threat to their sight, this project will save them from having to go through that difficult treatment unnecessarily. It will be life-changing for the children and their families, which is what excites me about this QI application.”
This project is a collaboration between Children’s Hospital of Philadelphia and Children’s National Hospital in Washington, D.C., in partnership with Children’s Hospital of Colorado and University of Pennsylvania. Upon project completion, the QI application will provide a precision-medicine approach for NF1-OPGs and improve clinical outcomes for pediatric tumors.

Sixteen finalists have been selected in the “Make Your Medical Device Pitch for Kids!” special COVID-19 edition competition presented by the National Capital Consortium for Pediatric Device Innovation (NCC-PDI). Representing innovations in COVID-19-related pediatric medical devices, the finalists will compete in a virtual pitch event held on July 20,2020 where up to $250,000 in awards will be given. Winners will receive grant funding of up to $50,000.
The competition is led by NCC-PDI co-founders the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland and powered by nonprofit accelerator and NCC-PDI member, MedTech Innovator.
This competition focuses on pediatric medical devices that support home health monitoring and telehealth, and improve sustainability, resiliency and readiness in diagnosing and treating children during a pandemic.
“As COVID -19 continues to threaten the health of families and children across the nation, we must continue to seek new and better ways to deliver quality care during a pandemic and offer technology solutions to reopen more safely,” says Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “Competitions like this are vital to get ahead of the healthcare challenge that COVID-19 presents in the world of pediatrics. By supporting innovation, we provide critical breakthroughs that can positively impact the lives of the children and families we serve.”
Along with grant funding, one company from the competition will be selected by Johnson & Johnson Innovation – JLABS to receive a one-year residency at JLABS @ Washington, DC, which will be located on the new Children’s National Research & Innovation Campus currently under construction. In addition to the 2021 JLABS residency, the awardee will have access to the JLABS community and expert mentoring by the Johnson & Johnson family of companies.
The 16 pediatric device innovations that judges selected for the final competition include:
Funding for the competition is made possible by a grant from the Food and Drug Administration (FDA) and a philanthropic gift from Mei Xu, founder of e-commerce platform Yes She May, a site dedicated to women-owned brands.
In addition to this COVID-19 special edition event, NCC-PDI recently revealed the ten finalists in its prestigious 8th annual “Make Your Medical Device Pitch for Kids!” competition. Cardiovascular, NICU, and orthopaedic and spine device innovations are the focus of the fall competition, taking place October 7, 2020 as part of the 8th Annual Symposium on Pediatric Device Innovation, presented by Children’s National and co-located with The MedTech Conference powered by AdvaMed.



Invited commentary by Sarah Mulkey, M.D., Ph.D., prenatal-neonatal neurologist in the Division of Prenatal Pediatrics at Children’s National Hospital, emphasizes importance of studying the Zika population long term.
A simple measuring tape could be the key to identifying which children could develop neurological and developmental abnormalities from Zika virus exposure during gestation. This is according to an invited commentary published July 7, 2020 in JAMA Network Open and written by Sarah Mulkey, M.D., Ph.D., prenatal-neonatal neurologist in the Division of Prenatal Pediatrics at Children’s National Hospital.
Zika virus (ZIKV), first isolated in 1947 in the Zika Forest in Uganda, made headlines in 2015-2016 for causing a widespread epidemic that spread through parts of North and South America, several islands in the Pacific and parts of Southeast Asia. Although previously linked with no or mild symptoms, researchers discovered during this epidemic that Zika can cross from a pregnant woman to her gestating fetus, leading to a syndrome marked by microcephaly (decreased brain growth), abnormal neurologic tone, vision and hearing abnormalities and joint contractures.
“For the 90% to 95% of ZIKV-exposed infants who fortunately were not born with severe abnormalities at birth and were normocephalic, our hope was that these children would have normal neurodevelopmental outcomes,” Dr. Mulkey writes in the commentary. “Unfortunately, this has not been the case.”
Her commentary expands on a study in the same issue entitled “Association between exposure to antenatal Zika virus and anatomic and neurodevelopmental abnormalities in children” by Cranston et al. In this study, the researchers find that head circumference — a simple measure taken regularly at postnatal appointments in the U.S. — can provide insight into which children were most likely to develop neurologic abnormalities. Their findings show that 68% of those whose head circumference was in the “normal” range at birth developed neurologic problems. Those whose head circumference was at the upper end of this range were significantly less likely to have abnormalities than those at the lower end.
Just this single measurement offers considerable insight into the risk of developing neurologic problems after Zika exposure. However, notes Dr. Mulkey, head circumference growth trajectory is also key. Of the 162 infants whose heads were initially in the normocephalic range at birth, about 10.5% went on to develop microcephaly in the months after birth.
“Because early head growth trajectory is associated with cognitive outcomes in early childhood,” Dr. Mulkey writes, “following the head circumference percentile over time can enable recognition of a child with increased risk for poor outcome who could benefit from early intervention therapies.”
This simple assessment could be significantly augmented with neuroimaging, she adds. The study by Cranston et al., as well as others in the field, have shown that brain imaging often reveals problems in ZIKV-exposed children, such as calcifications and cerebral atrophy, even in those with normal head circumferences. This imaging doesn’t necessarily need to take place at birth, Dr. Mulkey says. Postnatal development of microcephaly, failure to thrive or developmental delay can all be triggers for imaging later on.
Together, Dr. Mulkey says, the study by Cranston et al. and others that focus on ZIKV-exposed children support the need for following these patients long term. Children exposed to ZIKV in the epidemic nearly five years ago are now approaching school age, a time fraught with more complicated cognitive and social demands. Through her own research at Children’s National’s Congenital Zika Virus Program and collaboration with colleagues in Colombia, Dr. Mulkey is following multiple cohorts of ZIKV exposed children as they grow. She recently published a study on neurological abnormalities in one of these cohorts in JAMA Pediatrics in January 2020.
“It’s really important to follow these children as long as possible so we’ll really know the outcomes of this virus,” Dr. Mulkey says.


Despite having less overall microbial richness, children with Cystic Fibrosis displayed a greater presence of Staphylococcus species.
Cystic Fibrosis (CF) is a disease that mainly affects the lungs and arises from mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene that encodes for the CFTR membrane protein located on certain secretory cells. CFTR dysfunction leads to complications such as the production of abnormally viscous mucus which causes chronic suppurative lung infections that require antibiotics to treat. New drugs called CFTR modulators can help improve CFTR protein function and some are even FDA-approved for use in children. In addition to CFTR protein function, the lung’s resident microbiota and its richness of diversity, plays an important role in both health and disease, including CF.
In a new study published in Heliyon, scientists from Children’s National Hospital examined the difference in the upper airway microbiome between children with CF and healthy controls. Age-related differences among children with CF and the impact of CFTR modulators on microbial diversity were also assessed. Seventy-five children between 0-6 years of age participated in the study, including 25 children with CF and 50 healthy controls. For CF participants, oropharyngeal swabs and clinical data were obtained from the biorepository, while data for controls were obtained during a single clinical visit.
Analysis revealed that CF patients had less microbial diversity and different composition of the upper airway microbiome compared to age similar controls, a finding that is consistent with research on the lower airways. Despite having less overall microbial richness, children with CF displayed a greater presence of Staphylococcus species, (a main driver of the pulmonary exacerbations characteristic of CF), three Rothia operational taxonomic units (OTUs) and two Streptococcus OTUs. CF patients received a significantly higher number of antibiotics courses within the previous year compared to healthy controls, and further investigation will be necessary to understand the impact of antibiotics on the upper airway microbiome of infants and children with CF.
Longitudinal comparisons to study effects of age and CFTR modulation on the microbiome of children with CF were also undertaken. Younger CF patients (those 0 to <3 years of age at study enrollment), were more likely to have culturally-normal respiratory flora and more stable microbial composition over time than older CF patients (those ≥ 3–6 years of age at study enrollment), with no significant differences in alpha or beta diversity. Older CF patients were significantly more likely to be receiving a CFTR modulator than younger patients. CF patients receiving CFTR modulators had higher microbial diversity measures than those not receiving CFTR modulators and were closer (but still significantly lower) in microbial richness to healthy controls. No significant differences in beta diversity were found between the three groups.
This study adds to the growing body of evidentiary support for the use of CFTR modulators in improving airway microbial diversity in CF patients. Future studies with a larger cohort and greater focus on the impact on early initiation of CFTR modulators on microbial diversity and clinical outcomes is necessary.
The study, “Airway microbial diversity is decreased in young children with cystic fibrosis compared to healthy controls but improved with CFTR modulation,” was recently published in Heliyon. The lead author is Andrea Hahn, M.D., M.S., an investigator at the Children’s National Research Institute. Notable authors include Aszia Burrell; Emily Ansusinha; Hollis Chaney, M.D.; Iman Sami, M.D.; Geovanny F. Perez, M.D.; Anastassios C. Koumbourlis, M.D., M.P.H.; Robert McCarter, Sc.D.; and Robert J. Freishtat, M.D., M.P.H..


Nobuyuki Ishibashi, M.D., is the principal investigator on a $3.2 million NIH R01 to study white matter growth and repair in utero for fetal brains affected by congenital heart disease.
Many of the neurological deficits seen in children with congenital heart disease (CHD) are related to abnormal white matter development early in life caused by reduced oxygen supply to the brain while in utero. Children with immature white matter at birth also commonly sustain additional white matter injuries following cardiac surgery.
The NIH recently awarded a prestigious R01 grant totaling more than $3.2 million to a collaborative project led by the Center for Neuroscience Research, the Sheikh Zayed Institute for Pediatric Surgical Innovation and the Children’s National Heart Institute at Children’s National Hospital as well as MedStar Washington Hospital Center.
The research, titled “White matter protection in the fetus with congenital heart disease,” looks specifically at whether providing a supplemental amount of the naturally occurring tetrahydrobiopterin (BH4) for pregnant women could rescue white matter development of fetuses with congenital heart disease whose brains aren’t receiving enough oxygen – or suffering from hypoxic-ischemic events.
Previous preclinical studies have shown that this lack of oxygen depletes the brain’s natural BH4 level, and the researchers hypothesize that BH4 levels play a critical role in the growth and development of white matter in the fetal brain by triggering key cellular/molecular processes. Specifically, the study will focus on three aims:
This laboratory-based work is the first step to determining if the neurodevelopment of babies born with CHD can be preserved or recovered by addressing key brain development that occurs before the baby is even born. Findings related to congenital heart disease may also translate to other populations where white matter development is affected by hypoxia-ischemia, including premature infants.
The project is led by principal investigator Nobuyuki Ishibashi, M.D., with co-investigators Vittorio Gallo, Ph.D., Joseph Scafidi, D.O., and Mary Donofrio, M.D. as well as colleagues at MedStar Washington Hospital Center.


Physician-scientists from Children’s National Hospital are unlocking new insights into Cystic Fibrosis by studying the type and number of bacteria in the lungs.
Cystic Fibrosis (CF) is a genetic disorder that chiefly affects the lungs and results in the production of abnormally dehydrated, viscous mucus. The inability to adequately clear this mucus leads to bacterial retention and both intermittent and chronic lung infections which require antibiotic therapy to treat. Researchers have used 16S rDNA amplicon sequencing for years in the attempts to characterize the airway microbiomes of CF patients, and more recently have used shotgun whole genome sequencing (WGS) techniques to obtain further details regarding bacterial species and strains. Previous studies on the airway microbiomes of CF patients have revealed that inter-person variability is high and can sometimes exceed intra-person variability. This can preclude generalizations regarding the CF population as a whole, which includes more than 30,000 Americans.
A recently published case study examined a young child with advanced and severely aggressive CF over a 12-month period, during which five pulmonary exacerbations occurred. A total of 14 sputum samples were collected across three clinical periods- baseline, exacerbation, and treatment. Samples were subsequently genetically sequenced (via 16s rDNA sequencing and, in three instances, WGS) and volatile metabolites were analyzed. The researchers hypothesized that if signature microbiome and metabolome characteristics correlated with one other and could be identified for each disease state, this data could serve as conglomerate biomarkers for the continuum of CF clinical states within an individual. In turn, this could inform future study design in a larger cohort.
Across all sputum samples, 109 individual operational taxonomic units (OTUs) and 466 distinct volatile metabolites were identified. 16s rDNA sequencing and WGS revealed that Escherichia coli and Staphylococcus aureus were the predominant bacteria during most baseline and exacerbation samples, despite some significant fluctuations in relative abundances. After the patient’s fifth antibacterial course, however, Achromobacter xylosoxidans became the new dominant bacterium.
Analysis revealed that the phylum Bacteroidetes and the genus Stenotrophomonas were significantly more abundant in treatment periods compared to baseline and exacerbation periods. WGS revealed the presence of bacteriophages as well as antibiotic resistance genes (mostly due to multi-drug resistance mechanisms), which can have important clinical ramifications and adds some dimensionality to the genetic analysis.
Volatile metabolite analysis found that observable fluctuations in metabolome composition coincided with fluctuations in the sputum microbiome. In this case, the microbiome and volatile metabolites produced by these bacteria provided an accurate assessment of the child’s clinical state. More specifically, the authors saw a distinct shift in both the microbiome and volatile metabolites with antibiotic treatment across the five independent pulmonary exacerbations. These additional assessments of the bacteria within the CF airway could provide an additional technique beyond standard bacterial cultures to better understand how the patient is responding to antibiotic treatment. Future studies in a larger group of children with CF may provide further insights into bacteria and volatile metabolite combinations that predict pulmonary exacerbation.
The article, “Longitudinal Associations of the Cystic Fibrosis Airway Microbiome and Volatile Metabolites: A Case Study,” was published in Frontiers in Cellular and Infection Microbiology. The lead author is Andrea Hahn, M.D., M.S., an investigator at the Children’s National Research Institute. Notable authors include Iman Sami, M.D., pulmonologist at Children’s National; Anastassios C. Koumbourlis, M.D., M.P.H, director of the Cystic Fibrosis Center; and Robert J. Freishtat, M.D., M.P.H, senior investigator at the Center for Genetic Medicine Research.


New research, published in AIDS and Behavior, shows the effectiveness of an Advance Care Planning model developed through participatory research with adolescents in improving palliative care among adult people living with HIV (PLWH).
Since the beginning of the COVID-19 pandemic, there has been a dramatic increase in advance care planning (ACP) and the creation of advance directives, also known as living wills, in the United States. New research, published in AIDS and Behavior, shows the effectiveness of an ACP model developed through participatory research with adolescents in improving palliative care among adult people living with HIV (PLWH).
These findings demonstrate that ACP positively contributes to the palliative care of adult PLWH by relieving suffering and maximizing quality of life. The intervention was based on the FAmily CEntered (FACE) Advance Care Model, which was developed and tested by principal investigator Maureen E. Lyon, Ph.D., and her colleagues.
Dr. Lyon’s team used this model successfully with adolescents living with HIV as part of five-year, five-site trial that included Children’s National Hospital. The trial was co-funded by the National Institutes of Health and National Institute of Nursing Research. The success of that study was parlayed into a new five-year study testing a slightly modified ACP intervention in adults, with Children’s National serving as the coordinating center. “The adolescents showed us the way,” says Dr. Lyon.
The paper details the findings of a longitudinal, two arm, randomized controlled clinical trial examining whether an ACP intervention aimed at adult PLWH and their families correlated with higher congruence in treatment preferences, as well as higher congruence over time. Patient-surrogate dyads were randomized to an ACP intervention arm or an active control arm at a 2:1 ratio (86 intervention dyads and 43 control dyads at 18-month follow up), due to prior demonstrated benefit of ACP.
The ACP intervention consisted of two 60-minute, patient-focused sessions. During session 1, Respecting Choices Next Steps® ACP Conversation, both patients and their surrogate decision-makers focused on the patients’ understanding of HIV, experience of symptoms, fears, hopes and worries. Next, a patient’s treatment preferences were explored via the Statement of Treatment Preferences (SoTP), which became a part of the patient’s electronic health record (EHR). Surrogates were questioned on their comprehension and willingness to comply with the patient’s wishes. Session 1 was acknowledged as the beginning of a conversation, and continued conversation between the dyad was encouraged.
Session 2, Five Wishes©, involved a facilitator guiding the dyad through a Five Wishes© advance directive. Session 2 resulted in legal documentation of a patient’s preferences in five specific areas: The patient’s preferred health care decision-maker, the kind of medical treatment the patient wants, how comfortable the patient wants to be, how the patient wants people to treat him/her and what the patient wants loved ones to know. The patient, surrogate and treating physicians all received a copy, and a copy was also submitted to the patient’s EHR.
Dyads in the control arm participated in two 60-minute sessions entitled Developmental or Relationship History (excluding any medical questions) and Nutrition & Exercise.
The researchers then assessed treatment preference congruence for each patient-surrogate dyad by presenting them with five different hypothetical scenarios. After the first session, congruence across all scenarios was significantly higher among ACP intervention dyads compared to control dyads. ACP patients were also significantly more likely to give their surrogates leeway in treatment decision making compared to control patients.
Compared to control dyads, ACP dyads were significantly more likely to maintain High → High congruence transition and significantly less likely to experience Low → Low congruence transition as measured from immediately post-intervention to 12-months post-intervention. The only two cases of Low → High congruence transition occurred in the intervention arm. Of note, ACP surrogates accurately reported on changes in patient preferences over one year, showing the positive impact of early conversation on longitudinal congruence.
Dr. Lyon hopes these results will encourage people to talk to their loved ones as soon as possible about ACP, not only during the current pandemic but into the future. “People can use what’s happening in the news as a trigger to begin these conversations,” she says. “The 1990 Patient Self-Determination Act (PSDA) encourages persons of all ages– including children and their parents– to decide the type and extent of medical care they want to accept or refuse if they become unable to make those decisions due to illness. Our research shows conversations matter.”
The original research paper, “Effect of FAmily CEntered (FACE®)Advance Care Planning on Longitudinal Congruence in End-of-Life Treatment Preferences: A Randomized Clinical Trial,” was recently published in AIDS and Behavior. Dr. Maureen E. Lyon, Ph.D., FABPP, of the Center for Translational Research/Children’s Research Institute, was the principal investigator of the trial and a co-senior of the paper.


Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
You can view the entire Children’s National Research Institute academic annual report online.


Run at the state-level, mandatory newborn screening (NBS) programs detect a host of hereditary disorders so that infants can be treated before further damage, or even death, occurs.
Newborn screening (NBS) programs are critical to public health. Run at the state-level, mandatory NBS programs detect a host of hereditary disorders so that infants can be treated before further damage, or even death, occurs.
While much attention is paid to testing technology, programs must still meet basic minimum requirements to reliably identify and treat all affected individuals including minimum reporting requirements, case surveillance and a dedicated short-term follow-up program. In newborn screening, success is systematic.
A new report “How a baby with classic galactosemia was nearly missed: When the test succeeds but system fails,” published in the American Journal of Medical Genetics, takes a look at an individual case that almost slipped through the cracks of a local NBS program.
One disorder detected by NBS is classic galactosemia (CG), which arises from a deficiency in the galactose-1-phosphate uridyltransferase (GALT) enzyme, leaving infants unable to metabolize galactose-1-phosophate, a monosaccharide abundantly present in milk. CG can result in fatal liver failure, sepsis and coagulopathy if the affected infant is not switched to soy-based formula within the first week of life.
CG can be detected through a combination of enzyme assay, DNA analysis and galactose quantification. However, NBS programs differ in testing protocols for CG by state, and not all NBS programs conduct all of these tests. This is of particular relevance to the Washington, D.C., metropolitan area, a regional nexus where crossing state and district lines for medical care is common.
The report describes how a D.C.-born infant was screened for CG through all three tests. While his galactose levels were normal, his GALT was low and DNA testing revealed homozygosity for a CG mutation known as K285N. In tandem, the latter two indicators constitute a true positive result for CG, and necessitate the proper issuance of referrals, precautions and follow-up, which failed to occur in this case.
The infant breastfed and displayed notable lethargy, and parents were directed to a local emergency department in a neighboring state which does not screen for CG with DNA testing.
The providers there were unfamiliar with the DNA results, and after new labs came back normal, the NBS results were deemed as “likely falsely positive” for CG. Fortunately, a provider at the community hospital forwarded the NBS results to the Children’s National Rare Disease Institute (CNRDI). Upon review, CNRDI metabolic specialists immediately sought to rectify the situation by reaching out to the family with proper instructions and arranging a clinical evaluation, which occurred 10 days after birth.
While this case had a fortunate ending, the report highlights the potential deficiencies in NBS programs, which have historically been among America’s most successful public health initiatives. The proper and timely functioning of NBS systems is contingent upon the functioning of its constituent parts, including testing, diagnosis, follow-up, management and stakeholder education.
While test results were accurate in this case, systemic shortcomings left a patient in danger. As the authors state, “Programs must keep in mind that the true success of newborn screening extends beyond just the test itself…to improve safety and care outcomes we must focus on the system.”
A clinical report by a team of authors, mainly comprised of Children’s National clinicians, was published earlier this month in the American Journal of Medical Genetics. Authors include Sarah Viall, PPCNP, MSN, a pediatric nurse practitioner in the Rare Disease Institute; Nicholas Ah Mew, M.D., director of the Inherited Metabolic Disorders Program; and Beth A. Tarini, M.D., M.S., associate director of the Center for Translational Research.
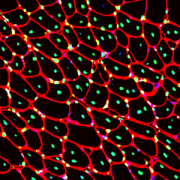
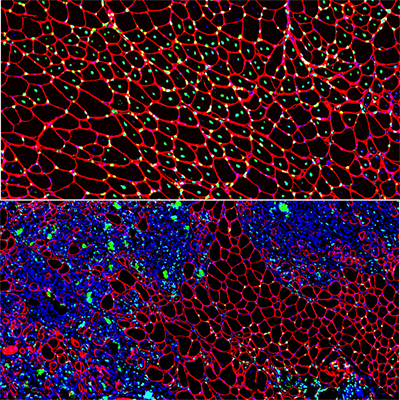
Muscle regeneration marked by incorporation of muscle stem cell nuclei (green) in the myofibers (red) in dystrophic muscles with low TGFβ level (upper image), but not with high TGFβ level (lower image). Inflammatory and other nuclei are labeled blue.
Boys with Duchenne muscular dystrophy (DMD) experience poor muscle regeneration, but the precise reasons for this remain under investigation. An experimental model of severe DMD that experiences a large spike in transforming growth factor-beta (TGFβ) activity after muscle injury shows that high TGFβ activity suppresses muscle regeneration and promotes fibroadipogenic progenitors (FAPs). This leads to replacement of the damaged muscle fibers by calcified and connective tissue, compromising muscle structure and function. While blocking FAP buildup provides a partial solution, a Children’s National Hospital study team identifies correcting the muscle micro-environment caused by high TGFβ as a ripe therapeutic target.
The team’s study was published online March 26, 2020, in JCI Insight.
DMD is a chronic muscle disease that affects 1 in 6,200 young men in the prime of their lives. The disorder, caused by genetic mutations leading to the inability to produce dystrophin protein, leads to ongoing muscle damage, chronic inflammation and poor regeneration of lost muscle tissue. The patients experience progressive muscle wasting, lose the ability to walk by the time they’re teenagers and die prematurely due to cardiorespiratory failure.
The Children’s National team finds for the first time that as early as preadolescence (3 to 4 weeks of age), their experimental model of severe DMD disease showed clear signs of the type of spontaneous muscle damage, regenerative failure and muscle fiber loss seen in preadolescent boys who have DMD.
“In boys, the challenge due to muscle loss exists from early in their lives, but had not been mimicked previously in experimental models,” says Jyoti K. Jaiswal, MSc, Ph.D., principal investigator in the Center for Genetic Medicine Research at Children’s National, and the study’s co-senior author. “TGFβ is widely associated with muscle fibrosis in DMD, when, in fact, our work shows its role in this disease process is far more significant.”
Research teams have searched for experimental models that replicate the sudden onset of symptoms in boys who have DMD as well as its complex progression.
“Our work not only offers insight into the delicate balance needed for regeneration of skeletal muscle, but it also provides quantitative information about muscle stem cell activity when this balanced is disturbed,” says Terence A. Partridge, Ph.D., principal investigator in the Center for Genetic Medicine Research at Children’s National, and the study’s co-senior author.
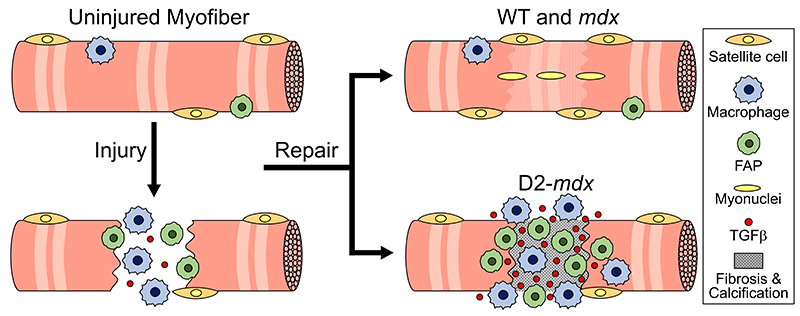
This schematic depicts the fate of injured myofibers in healthy or dystrophic muscle (WT or mdx experimental models) that maintain low TGFβ level, compared with D2-mdx experimental models that experience a large increase in TGFβ level. As the legend shows, various cells are involved in this regenerative response.
“The D2-mdx experimental model is a relevant one to use to investigate the interplay between inflammation and muscle degeneration that is seen in humans with DMD,” adds Davi A.G. Mázala, co-lead study author. “This model faithfully recapitulates many features of the complex disease process seen in humans.”
Between 3 to 4 weeks of age in the experimental models of severe DMD disease, the level of active TGFβ spiked up to 10-fold compared with models with milder disease. Intramuscular injections of an off-the-shelf drug that inhibits TGFβ signaling tamped down the number of FAPs, improving the muscle environment by lowering TGFβ activity.
“This work lays the foundation for studies that could lead to future therapeutic strategies to improve patients’ outcomes and lessen disease severity,” says James S. Novak, Ph.D., principal investigator in Children’s Center for Genetic Medicine Research, and co-lead study author. “Ultimately, our goal is to improve the ability of patients to continue to maintain muscle mass and regenerate muscle.”
In addition to Mázala, Novak, Jaiswal and Partridge, Children’s National study co-authors include Marshall W. Hogarth; Marie Nearing; Prabhat Adusumalli; Christopher B. Tully; Nayab F. Habib; Heather Gordish-Dressman, M.D.; and Yi-Wen Chen, Ph.D.
Financial support for the research described in this post was provided by the National Institutes of Health under award Nos. T32AR056993, R01AR055686 and U54HD090257; Foundation to Eradicate Duchenne; Muscular Dystrophy Association under award Nos. MDA295203, MDA480160 and MDA 477331; Parent Project Muscular Dystrophy; and Duchenne Parent Project – Netherlands.


Investigators from around the world penned manuscripts that were assembled in a special issue of “Neurochemical Research” that honors Vittorio Gallo, Ph.D., for his leadership in the field of neural development and regeneration.
At a pivotal moment early in his career, Vittorio Gallo, Ph.D., was accepted to work with Professor Giulio Levi at the Institute for Cell Biology in Rome, a position that leveraged courses Gallo had taken in neurobiology and neurochemistry, and allowed him to work in the top research institute in Italy directed by the Nobel laureate, Professor Rita Levi-Montalcini.
For four years as a student and later as Levi’s collaborator, Gallo focused on amino acid neurotransmitters in the brain and mechanisms of glutamate and GABA release from nerve terminals. Those early years cemented a research focus on glutamate neurotransmission that would lead to a number of pivotal publications and research collaborations that have spanned decades.
Now, investigators from around the world who have worked most closely with Gallo penned tributes in the form of manuscripts that were assembled in a special issue of “Neurochemical Research” that honors Gallo “for his contributions to our understanding of glutamatergic and GABAergic transmission during brain development and to his leadership in the field of neural development and regeneration,” writes guest editor Arne Schousboe, of the University of Copenhagen in Denmark.

Vittorio Gallo, Ph.D. as a 21-year-old mustachioed graduate student.
“In spite of news headlines about competition in research and many of the negative things we hear about the research world, this shows that research is also able to create a community around us,” says Gallo, chief research officer at Children’s National Hospital and scientific director for the Children’s National Research Institute.
As just one example, he first met Schousboe 44 years ago when Gallo was a 21-year-old mustachioed graduate student.
“Research can really create a sense of community that we carry on from the time we are in training, nurture as we meet our colleagues at periodic conferences, and continue up to the present. Creating community is bi-directional: influencing people and being influenced by people. People were willing to contribute these 17 articles because they value me,” Gallo says. “This is a lot of work for the editor and the people who prepared papers for this special issue.”
In addition to Gallo publishing more than 140 peer-reviewed papers, 30 review articles and book chapters, Schousboe notes a number of Gallo’s accomplishments, including:
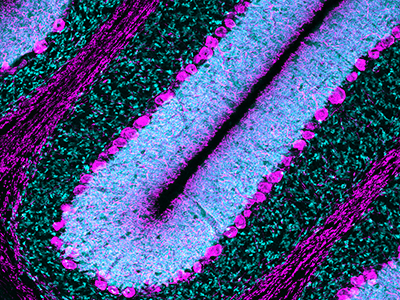
Purkinje cells are large neurons located in the cerebellum that are elaborately branched like interlocking tree limbs and represent the only source of output for the entire cerebellar cortex.
Even the image selected to grace the special issue’s cover continues the theme of continuity and leaving behind a legacy. That image of Purkinje cells was created by a young scientist who works in Gallo’s lab, Aaron Sathyanesan, Ph.D. Gallo began his career working on the cerebellum – a region of the brain important for motor control – and now studies with a team of scientists and clinician-scientists Purkinje cells’ role in locomotor adaptive behavior and how that is disrupted after neonatal brain injury.
“These cells are the main players in cerebellar circuitry,” Gallo says. “It’s a meaningful image because goes back to my roots as a graduate student and is also an image that someone produced in my lab early in his career. It’s very meaningful to me that Aaron agreed to provide this image for the cover of the special issue.”
Children’s National Hospital researchers for the first time have isolated bacterial extracellular vesicles from the blood of healthy donors. The team theorizes that the solar eclipse lookalikes contain important signaling proteins and chromatin, DNA from the human host.
Children’s National Hospital researchers for the first time have isolated bacterial extracellular vesicles from the blood of healthy donors, a critical step to better understanding the way gut bacteria communicate with the rest of the body via the bloodstream.
For decades, researchers considered circulating bacterial extracellular vesicles as bothersome flotsam to be jettisoned as they sought to tease out how bacteria that reside in the gut whisper messages to the brain.
There is a growing appreciation that extracellular vesicles – particles that cells naturally release – actually facilitate intracellular communication.
“In the past, we thought they were garbage or noise,” says Robert J. Freishtat, M.D., MPH, associate director, Center for Genetic Medicine Research at Children’s National Research Institute. “It turns out what we throw away is not trash.”
Kylie Krohmaly, a graduate student in Dr. Freishtat’s laboratory, has isolated from blood, extracellular vesicles from Escherichia coli and Haemophilus influenzae, common bacteria that colonize the gut, and validated the results via electron microscopy.
“The images are interesting because they look like they have a bit of a halo around them or penumbra,” Krohmaly says.
The team theorizes that the solar eclipse lookalikes contain important signaling proteins and chromatin, DNA from the human host.
“It’s the first time anyone has pulled them out of blood. Detecting them is one thing. Pulling them out is a critical step to understanding the language the microbiome uses as it speaks with its human host,” Dr. Freishtat adds.
Krohmaly’s technique is so promising that the Children’s National team filed a provisional patent.
The Children’s research team has devised a way to gum up the cellular works so that bacteria no longer become antibiotic resistant. Targeted bacteria retain the ability to make antibiotic-resistance RNA, but like a relay runner dropping rather than passing a baton, the bacteria are thwarted from advancing beyond that step. And, because that gene is turned off, the bacteria are newly sensitive to antibiotics – instead of resistant bacteria multiplying like clockwork these bacteria get killed.
“Our plan is to hijack this process in order to turn off antibiotic-resistance genes in bacteria,” Dr. Freishtat says. “Ultimately, if a child who has an ear infection can no longer take amoxicillin, the antibiotic would be given in tandem with the bacteria-derived booster to turn off bacteria’s ability to become antibiotic resistant. This one-two punch could become a novel way of addressing the antibiotic resistance process.”
ISEV2020 Annual Meeting presentation
(Timing may be subject to change due to COVID-19 safety precautions)
Oral with poster session 3: Neurological & ID
Saturday May 23, 2020, 5 p.m. to 5:05 p.m. (ET)
“Detection of bacterial extracellular vesicles in blood from healthy volunteers”
Kylie Krohmaly, lead author; Claire Hoptay, co-author; Andrea Hahn, M.D., MS, infectious disease specialist and co-author; Robert J. Freishtat, M.D., MPH, associate director, Center for Genetic Medicine Research at Children’s National Research Institute and senior author.


Factoring in the total number of days that extremely preterm infants require supplemental oxygen and tracking this metric for weeks longer than usual improves clinicians’ ability to predict respiratory outcomes according to bronchopulmonary dysplasia severity.
Factoring in the total number of days that extremely preterm infants require supplemental oxygen and tracking this metric for weeks longer than usual improves clinicians’ ability to predict respiratory outcomes according to bronchopulmonary dysplasia (BPD) severity, a research team led by Children’s National Hospital writes in Scientific Reports. What’s more, the researchers defined a brand-new category (level IV) for newborns who receive supplemental oxygen more than 120 days as a reliable way to predict which infants are at the highest risk of returning to the hospital due to respiratory distress after discharge.
About 1 in 10 U.S. infants is born preterm, before 37 weeks gestation, according to the Centers for Disease Control and Prevention. That includes extremely preterm infants who weigh about 1 lb. at birth. These very low birthweight newborns have paper thin skin, frail hearts and lungs that are not yet mature enough to deliver oxygen throughout the body as needed. Thanks to advances in neocritical care, an increasing number of them survive prematurity, and many develop BPD, a chronic lung disease characterized by abnormal development of the lungs and pulmonary vasculature.
“About half of the babies born prematurely will come back to the hospital within the first year of life with a respiratory infection. The key is identifying them and, potentially, preventing complications in this high-risk population,” says Gustavo Nino, M.D., a Children’s National pulmonologist and the study’s lead author.
For decades, the most common way to stratify BPD risk in these vulnerable newborns has been to see if they require supplemental oxygen at 36 weeks corrected gestational age.
“The problem with this classification is it doesn’t take into account the very premature babies who are on oxygen for much longer than other babies. So, we asked the question: Can we continue risk stratification beyond 36 weeks in order to identify a subset of babies who are at much higher risk of complications,” Dr. Nino says.
The longitudinal cohort study enrolled 188 infants born extremely preterm who were admitted to the neonatal intensive care unit (NICU) at Children’s National and tracked their data for at least 12 months after discharge. The team used a multidimensional approach that tracked duration of supplemental oxygen during the newborns’ NICU stay as well as scoring lung imaging as an independent marker of BPD severity. To validate the findings, these U.S.-born newborns were matched with 130 infants who were born preterm and hospitalized at two NICUs located in Bogotá, Colombia.
“Babies who are born very preterm and require oxygen beyond 120 days should have expanded ventilation of the lungs and cardiovascular pulmonary system before going home,” he notes. “We need to identify these newborns and optimize their management before they are discharged.”
And, the babies with level IV BPD risk need a different type of evaluation because the complications they experience – including pulmonary hypertension – place them at the highest risk of developing sleep apnea and severe respiratory infection, especially during the first year of life.
“The earlier we identify them, the better their outcome is likely to be,” Dr. Nino says. “We really need to change the risk stratification so we don’t call them all ‘severe’ and treat them the same when there is a subset of newborns who clearly are at a much higher risk for experiencing respiratory complications after hospital discharge.”
In addition to Dr. Nino, Children’s National study co-authors include Awais Mansoor, Ph.D., staff scientist at the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI); Geovanny F. Perez, M.D., pediatric pulmonologist; Maria Arroyo, M.D., pulmonologist; Xilei Xu Chen, M.D., postdoctoral fellow; Jered Weinstock, pediatric pulmonary fellow; Kyle Salka, MS, research technician; Mariam Said, M.D., neonatologist, and Marius George Linguraru, DPhil, MA, MSc, SZI principal investigator and senior author. Additional co-authors include Ranniery Acuña-Cordero, Universidad Militar Nueva Granada, Bogotá, Colombia; and Monica P. Sossa-Briceño and Carlos E. Rodríguez-Martínez, both of Universidad Nacional de Colombia.
Funding for research described in this post was provided by the National Institutes of Health (NIH) under award Nos. HL145669, AI130502 and HL141237. In addition, the NIH has awarded Dr. Nino an RO1 grant to continue this research.
Children’s National Hospital collects patients’ blood, extracts T-cells and replicates them in the presence of specific proteins found on cancer cells which, in essence, teaches the T-cells to target specific tumor markers. Training the T-cells, growing them to sufficient quantities and ensuring they are safe for administration takes weeks. But when patients return to the outpatient clinic, their T-cell infusion lasts just a few minutes.
For the third consecutive year, Children’s National was selected to compete in STAT Madness, an annual bracket-style competition that chooses the year’s most impactful biomedical innovation by popular vote. Children’s entry, “Immunotherapy of relapsed and refractory solid tumors with ex vivo expanded multi-tumor associated antigen specific cytotoxic T lymphocytes,” uses the body’s own immune system to attack and eliminate cancer cells in pediatric and adult patients with solid tumor malignancies.
In 2018, Children’s first-ever STAT Madness entry advanced through five brackets in the national competition and, in the championship round, finished second. That innovation, which enables more timely diagnoses of rare diseases and common genetic disorders, helping to improve kids’ health outcomes around the world, also was among four “Editor’s Pick” finalists, entries that spanned a diverse range of scientific disciplines.
An estimated 11,000 new cases of pediatric cancer were diagnosed in children 14 and younger in the U.S. in 2019. And, when it comes to disease, cancer remains the leading cause of death among children, according to the National Institutes of Health. An enterprising research team led by Children’s National faculty leveraged T-cells – essential players in the body’s immune system – to treat pediatric and adult patients with relapsed or refractory solid tumors who had exhausted all other therapeutic options.
“We’re using the patient’s own immune system to fight their cancer, rather than more traditional chemotherapy drugs,” says Catherine M. Bollard, M.D., director of the Center for Cancer & Immunology Research at Children’s National and co-senior author of the study. “It’s more targeted and less toxic to the patient. These T-cells home in on any cancer cells that might be in the body, allowing healthy cells to continue to grow,” Dr. Bollard adds.
That means patients treated in the Phase I, first-in-human trial didn’t lose their hair and weren’t hospitalized for the treatment. After a quick clinical visit for their treatment, they returned to normal activities, like school, with good energy levels.
“With our specially trained T-cell therapy, many patients who previously had rapidly progressing disease experienced prolonged disease stabilization,” says Holly J. Meany, M.D., a Children’s National oncologist and the study’s co-senior author. “Patients treated at the highest dose level showed the best clinical outcomes, with a six-month, progression-free survival of 73% after tumor-associated antigen cytotoxic T-cell (TAA-T) infusion, compared with 38% with their immediate prior therapy.”
The multi-institutional team published their findings from the study online July 29, 2019, in the Journal of Clinical Oncology.
“Our research team and our parents are delighted that some patients treated in our study continue to do well following T-cell therapy without additional treatment. In some cases, two years after treatment, patients do not appear to have active disease and are maintaining an excellent quality of life,” says Amy B. Hont, M.D., the study’s lead author. “One of these was a patient whose parents were told his only other option was palliative care. Our innovation gives these families new hope,” Dr. Hont adds.
The 2020 STAT Madness #Core64 bracket opened March 2, and the champion will be announced April 6.
In addition to Drs. Hont, Meany and Bollard, Children’s National co-authors include C. Russell Cruz, M.D., Ph.D., Robert Ulrey, MS, Barbara O’Brien, BS, Maja Stanojevic, M.D., Anushree Datar, MS, Shuroug Albihani, MS, Devin Saunders, BA, Ryo Hanajiri, M.D., Ph.D., Karuna Panchapakesan, MS, Payal Banerjee, MS, Maria Fernanda Fortiz, BS, Fahmida Hoq, MBBS, MS, Haili Lang, M.D., Yunfei Wang, DrPH, Patrick J. Hanley, Ph.D., and Jeffrey S. Dome, M.D., Ph.D.; and Sam Darko, MS, National Institute of Allergy and Infectious Diseases.
Financial support for the research described in this post was provided by the Children’s National Hospital Heroes Gala, Alex’s Army Foundation, the Children’s National Board of Visitors and Hyundai Hope on Wheels Young Investigator Grant to Support Pediatric Cancer Research, the Children’s National Research Institute Bioinformatics Unit, the Clinical and Translational Science Institute and the National Institutes of Health under award No. UL1-TR001876.
Researchers at Children’s National Hospital are using quantitative imaging and machine intelligence to enhance care for children with a common kidney disease, and their initial results are very promising. Their technique provides an accurate way to predict earlier which children with hydronephrosis will need surgical intervention, simplifying and enhancing their care.
We live in a time of great uncertainty yet great promise, particularly when it comes to harnessing technology to improve lives. Researchers at Children’s National Hospital are using quantitative imaging and machine intelligence to enhance care for children with a common kidney disease, and their initial results are very promising. Their technique provides an accurate way to predict earlier which children with hydronephrosis will need surgical intervention, simplifying and enhancing their care.
Hydronephrosis means “water in the kidney” and is a condition in which a kidney doesn’t empty normally. One of the most frequently detected abnormalities on prenatal ultrasound, hydronephrosis affects up to 4.5% of all pregnancies and is often discovered prenatally or just after birth.
Although hydronephrosis in children sometimes resolves by itself, identifying which kidneys are obstructed and more likely to need intervention isn’t particularly easy. But it is critical. “Children with severe hydronephrosis over long periods of time can start losing kidney function to the point of losing a kidney,” says Marius George Linguraru, DPhil, MA, MSc, principal investigator of the project; director of Precision Medical Imaging Group at the Sheikh Zayed Institute for Pediatric Surgical Innovation; and professor of radiology, pediatrics and biomedical engineering at George Washington University.
Children with hydronephrosis face three levels of examination and intervention: ultrasound, nuclear imaging testing called diuresis renogram and surgery for the critical cases. “What we want to do with this project is stratify kids as early as possible,” Dr. Linguraru says. “The earlier we can predict, the better we can plan the clinical care for these kids.”
Ultrasound is used to see whether there is a blockage and try to determine hydronephrosis severity. “Ultrasound is non-invasive, non-radiating, and does not expose the child to any risk prenatally or postnatally,” Dr. Linguraru says. Ultrasound evaluations require a trained radiologist, but there’s a lot of variability. Radiologists have a grading system based on the ultrasound appearance of the kidney to determine whether the hydronephrosis is mild, moderate or severe, but studies show this isn’t predictive of longer term outcomes.
Children whose ultrasounds show concern will be referred to diuresis renogram. Costly, complex, invasive and irradiating, it tests how well the kidney empties. Although appropriate for good clinical indications, doctors try to minimize its use. “Management of hydronephrosis is complex,” Dr. Linguraru says. “We want to use ultrasound as much as possible and much less diuresis renogram.”
For those patients whose kidney is obstructed and eventually need surgical intervention, the sooner that decision can be made the better. “The more you wait for a kidney that is severely obstructed, the more function may be lost. If intervention is required, it’s preferable to do it early,” Dr. Linguraru says. Of course for the child whose hydronephrosis will likely resolve itself, intervention is not the best option.
“With our technique we are measuring physiological and anatomical changes in the ultrasound image of the kidney,” says Marius George Linguraru, DPhil, MA, MSc. “The human eye may find it difficult to put all this together, but the machine can do it. We use quantitative imaging to do deep phenotyping of the kidney and machine learning to interpret the data.”
Dr. Linguraru and the multidisciplinary team at Children’s National Hospital, including radiology and urology clinicians, are putting the power of computers to work interpreting subtleties in the ultrasound data that humans just can’t see. In their pilot study they found that 60% of the nuclear imaging tests could have been safely avoided without missing any of the critical cases of hydronephrosis. “With our technique we are measuring physiological and anatomical changes in the ultrasound image of the kidney,” Dr. Linguraru says. “The human eye may find it difficult to put all this together, but the machine can do it. We use quantitative imaging to do deep phenotyping of the kidney and machine learning to interpret the data.”
Results of the initial study indicate that kids who have a mild condition can be safely discharged earlier and the model can predict all those kids with obstructions and accelerate their diagnosis by sending them earlier to get further investigation. Dr. Linguraru says. “There are only benefits: some kids will get earlier diagnosis, some earlier discharges.”
The team also has a way to improve the interpretation of diuresis renograms. “We analyze the dynamics of the kidney’s drainage curve in quantifiable way. Using machine learning to interpret those results, we showed we can potentially discharge some kids earlier and accelerate intervention for the most severe cases instead of waiting and repeating the invasive tests,” he says. The framework has 93% accuracy, including 91% sensitivity and 96% specificity, to predict surgical cases, a significant improvement over clinical metrics’ accuracy.
The next step is a study connecting all the protocols. “Right now we have a study on ultrasound, a study on nuclear imaging, but we need to connect them so a child with hydronephrosis immediately benefits,” says Dr. Linguraru. Future work will focus on streamlining and accelerating diagnosis and intervention for kids who need it, both in prospective studies and hopefully clinically as well.
Hydronephrosis is an area in which machine learning can be applied to pediatric health in meaningful ways because of the sheer volume of cases.
“Machine learning algorithms work best when they are trained well on a lot of data,” Dr. Linguraru says. “Often in pediatric conditions, data are sparse because conditions are rare. Hydronephrosis is one of those areas that can really benefit from this new technological development because there is a big volume of patients. We are collecting more data, and we’re becoming smarter with these kinds of algorithms.”
Learn more about the Precision Medical Imaging Laboratory and its work to enhance clinical information in medical images to improve children’s health.
