
Innovating improved outcomes with robotic gallbladder removal
Patients want to hear they are “in good hands” when choosing a surgeon. A Children’s National Hospital team is investigating whether those hands could be replaced with an autonomous robotic arm during pediatric cholecystectomy procedures.
“The role of autonomous surgery is at a pivot point,” said Anthony Sandler, M.D., senior vice president and surgeon-in-chief at Children’s National and director of the Sheikh Zayed Institute of Pediatric Surgical Innovation (SZI). “Just as it is with autonomously driving cars, we are testing whether a gallbladder removal can be controlled and managed by a robotic arm, rather than a laparoscopic surgeon. In preclinical models, we are evaluating whether we can take the next step forward. We believe we can, and this research will be proof of concept for autonomous surgery.”
The big picture
The rate of cholecystectomy has been on the rise among pediatric patients for the last two decades. It becomes necessary when the gallbladder becomes full of painful gallstones, often caused by obesity and inherited blood disorders like sickle cell disease. Across the country, 99% of gallbladder removals happen without complications.
Yet Children’s National hopes to develop technologies to boost that number even higher. Working with partners, the hospital has embarked on two contracts with the Advanced Research Projects Agency for Health (ARPA-H): a three-year and a two-year contract, worth $3.5 million each (75N91023C00048 & 75N91023C00053, respectively). The Children’s National team is collaborating on solutions with Optosurgical Chief Executive Officer Yoseph Kim, M.S.E., and Axel Krieger, Ph.D., associate professor of mechanical engineering at Johns Hopkins University.
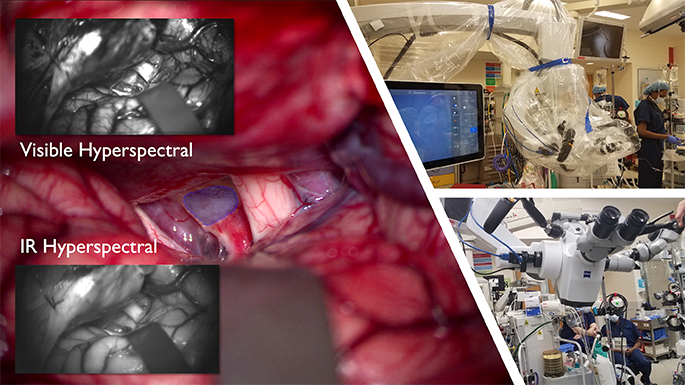
They are tapping into two areas of expertise: robotic surgery and the development of a novel fluorescent dye that – when paired with advanced imaging – can aid surgeons in seeing bleeds during gallbladder removals.
The project also combines the talents of Dr. Sandler and Children’s National optical engineer Richard Cha, Ph.D., principal investigator at SZI, to explore how to integrate these technologies in the operating room.
“Autonomous gallbladder removal involves the identification of the target tissue – the bile duct, the cystic artery and the gallbladder. Our team’s new 3D imaging techniques will help visualize and work through the surgical steps, by locating each target,” Dr. Cha said. “When this technology and related programming come together, it could mark a significant step forward in pediatric surgery.”
The fine print
Given the gallbladder’s small size and accessible location just beneath the liver, cholecystectomy is most often done laparoscopically, using small cameras and incisions. There are three main steps: ligating – or closing off – the cystic artery, ligating the cystic duct while protecting the common bile duct, and removing the gallbladder. Drs. Sandler and Cha believe outcomes will improve if the expertise and delicacy of a robot are incorporated into the procedure.
“If you’re that one patient out of 100 who has significant bleeding post-operatively or, even worse, you are among the 0.5% of patients who have an injury to the bile duct, the impact on your wellbeing is significant after that surgery,” Dr. Sandler said. “Having that extra security of technology and guidance will be an incredible value-add for any patient undergoing this procedure.”
These projects have been funded in whole with federal funds from ARPA-H, National Institutes of Health, Department of Health and Human Services, under Contract No. 75N91023C00053 and Contract No. 75N91023C00048.








 Advanced MRI visualization techniques to follow blood flow in the hearts of cardiac patients. Gene therapy for pediatric patients with Duchenne muscular dystrophy. 3D-printed casts for treating clubfoot. These were among the most popular articles we published on Innovation District in 2023. Read on for our full list.
Advanced MRI visualization techniques to follow blood flow in the hearts of cardiac patients. Gene therapy for pediatric patients with Duchenne muscular dystrophy. 3D-printed casts for treating clubfoot. These were among the most popular articles we published on Innovation District in 2023. Read on for our full list.

 The hospital will advocate for the unique needs of children as part of nationwide network working to accelerate transformative health solutions.
The hospital will advocate for the unique needs of children as part of nationwide network working to accelerate transformative health solutions.
 Children’s National Hospital was awarded nearly $7.5 million in a five-year grant to continue its leadership of an FDA-funded pediatric device consortium. Building upon a decade of previous consortium leadership, the new consortium is Alliance for Pediatric Device Innovation (APDI) and features a new and expanded roster of partners that reflects its added focus on providing pediatric innovators with expert support on evidence generation, including the use of real-world evidence (RWE), for pediatric device development.
Children’s National Hospital was awarded nearly $7.5 million in a five-year grant to continue its leadership of an FDA-funded pediatric device consortium. Building upon a decade of previous consortium leadership, the new consortium is Alliance for Pediatric Device Innovation (APDI) and features a new and expanded roster of partners that reflects its added focus on providing pediatric innovators with expert support on evidence generation, including the use of real-world evidence (RWE), for pediatric device development.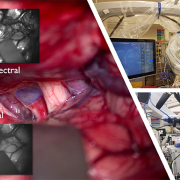



 Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked #5 in the nation on the U.S. News & World Report 2023-24 Best Children’s Hospitals annual rankings. This marks the seventh straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.

