In a cohort retrospective study comparing clinical features of COVID-19 and seasonal flu, researchers found surprisingly little difference in the rates of hospitalization, admission to the intensive care unit and mechanical ventilator use between the two groups.
As the fall approaches, pediatric hospitals will start seeing children with seasonal influenza A and B. At the same time, COVID-19 will be co-circulating in communities with the flu and other respiratory viruses, making it more difficult to identify and prevent the novel coronavirus.
With little published data directly comparing the clinical features of children with COVID-19 to those with seasonal flu, researchers at Children’s National Hospital decided to conduct a retrospective cohort study of patients in the two groups. Their findings — published September 8 in JAMA Network Open — surprised them.
The study — detailed in the article “Comparison of Clinical Features of US Children With COVID-19 vs Seasonal Influenza A and B” — showed no statistically significant differences in the rates of hospitalization, admission to the intensive care unit and mechanical ventilator use between the two groups.
The other unexpected finding was that more patients with COVID-19 than those with seasonal influenza reported fever, cough, diarrhea or vomiting, headache, body ache or chest pain at the time of diagnosis, says Xiaoyan Song, Ph.D., M.Sc., M.B., the study’s principal investigator.
“I didn’t see this coming when I was thinking about doing the study,” says Dr. Song, director of Infection Control and Epidemiology at Children’s National since 2007 and a professor of pediatrics at the George Washington University School of Medicine and Health Sciences. “It took several rounds of thinking and combing through the data to convince myself that this was the conclusion.”
Given that much remains unknown about COVID-19, the researchers’ discovery that children with the disease present with more symptoms at the time of diagnosis is a valuable one.
“It’s a good cue from a prevention and planning perspective,” says Dr. Song. “We always emphasize early recognition and early isolation with COVID. Having a clinical picture in mind will assist clinicians as they diagnose patients with symptoms of the coronavirus.”
The study included 315 children who were diagnosed with a laboratory-confirmed COVID-19 between March 25, 2020, and May 15, 2020, and 1,402 children who were diagnosed with a laboratory-confirmed seasonal influenza between Oct. 1, 2019, and June 6, 2020, at Children’s National. Asymptomatic patients who tested positive for COVID-19 during pre-admission or pre-procedural screening were excluded from the study.
Of the 315 patients who tested positive for COVID-19, 52% were male, with a median age of 8.4 years. Of these patients, 54 (17.1 %) were hospitalized, including 18 (5.7%) who were admitted to the intensive care unit (ICU) and 10 (3.2%) who received mechanical ventilator treatment.
Among the 1,402 patients who tested positive for influenza A or B, 52% were male, with a median age of 3.9 years, and 291 (21.2%) were hospitalized, including 143 for influenza A and 148 for influenza B. Ninety-eight patients (7.0%) were admitted to the ICU, and 27 (1.9%) received mechanical ventilator support.
The study showed a slight difference in the age of children hospitalized with COVID-19 compared to those hospitalized with seasonal influenza. Patients hospitalized with COVID-19 had a median age of 9.7 years vs. those hospitalized with seasonal influenza who had a median age of 4.2 years.
In both groups, fever was the most often reported symptom at the time of diagnosis followed by cough. A greater proportion of patients hospitalized with COVID-19 than those hospitalized with seasonal influenza reported fever (76% vs. 55%), cough (48% vs. 31%), diarrhea or vomiting (26% vs. 12%), headache (11% vs. 3%), body ache/myalgia (22% vs. 7%), and chest pain (11% vs. 3%).
More patients hospitalized with COVID-19 than those with seasonal influenza reported sore throat or congestion (22% vs. 20%) and shortness of breath (30% vs. 20%), but the differences were not statistically significant.
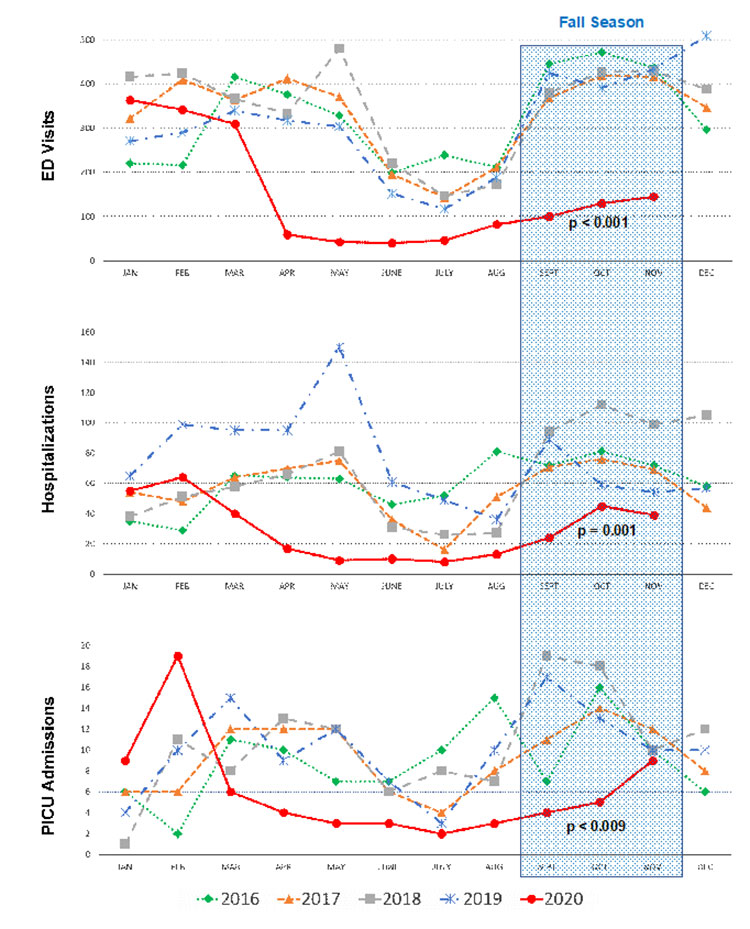
During the study period, the researchers noticed an abrupt decline of influenza cases at Children’s National after local schools closed in mid-March and stay-at-home orders were implemented about two weeks later to combat the community spread of COVID-19. Dr. Song says the impact of school closures on the spread of COVID-19 among children is the next area of study for her research team.
“We want to assess the quantitative impact of school closures so we can determine at what point the cost of closing schools and staying at home outweighs the benefit of reducing transmission of COVID-19 and burdens on the health care system,” she says.
Dr. Song urges members of the community “first and foremost to stay calm and be strong. We’re learning new and valuable things about this virus each day, which in turn improves care. The collision of the flu and COVID-19 this fall could mean an increase in pediatric hospitalizations. That’s why it’s important to get your flu shot, because it can help take at least one respiratory virus out of circulation.”
Other researchers who contributed to this study include Meghan Delaney, D.O.; Rahul K. Shah, M.D.; Joseph M. Campos, Ph.D.; David L. Wessel, M.D.; and Roberta L. DeBiasi, M.D.