Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
For the fifteenth straight year, Children’s National ranked in 10 specialty services and is the highest U.S. News ranked children’s hospital in Washington, D.C., Maryland and Virginia. Last year, U.S. News introduced pediatric & adolescent behavioral health as a service line in its rankings. While there are no ordinal rankings for behavioral health, the Children’s National program was named one of the top 50 programs in the country for the second year in a row.
“To be named among the nation’s top children’s hospitals for nine years in a row is a reflection of the extraordinary expertise, innovation and heart that our teams bring to every child and family we serve,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “Our leadership in specialties like neurology, cancer, and diabetes and endocrinology underscores the national impact of our work, and we remain focused on setting new standards in pediatric care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“Being a top-ranked pediatric hospital means more than just excelling in a single specialty — it means being a pillar of outstanding care for your entire region,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Our rankings acknowledge these hospitals for their comprehensive excellence, helping families find the very best care conveniently located within their state and community.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/USNWR_CNBadges_Set2SideBySide_2025-26-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-07 01:00:072026-01-05 17:33:17Children’s National Hospital once again ranked among the nation’s best by U.S. News & World Report
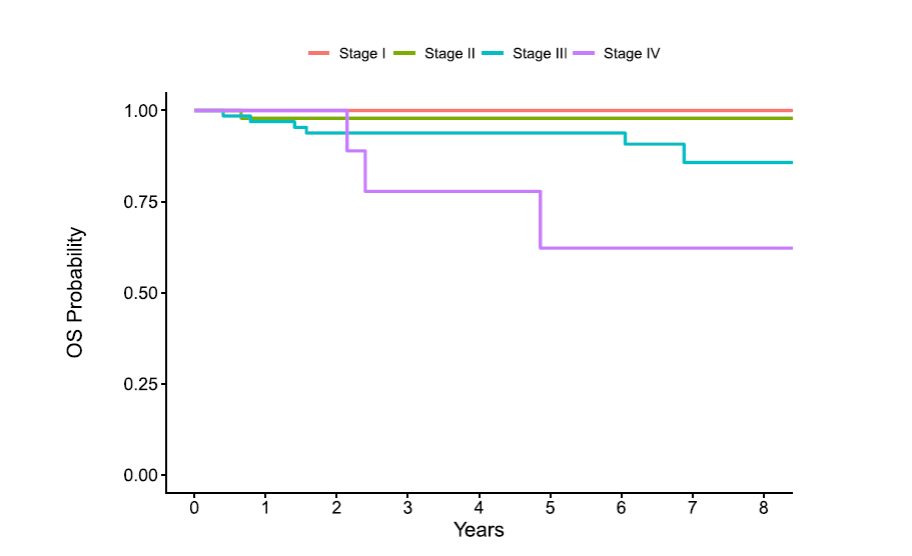
Overall survival by stage in Clear Cell Sarcoma of the Kidney (CCSK). Stage I/II patients demonstrate excellent outcomes, while stage IV shows meaningful improvement compared with historical cohorts, underscoring the need for continued therapeutic advances in high-risk disease.
Recent findings show that children with stage I–II FAWT achieve 100% 4-year overall survival with vincristine/dactinomycin/doxorubicin chemotherapy (DD4A) plus flank radiation, while children with stage IV disease benefited from intensified regimens. These results confirm that therapy can be adjusted to disease stage, balancing survival with long-term side effects.
Clear cell sarcoma of the kidney
For CCSK, new evidence supports omitting radiation in stage I patients when lymph nodes are sampled, reducing treatment burden without sacrificing outcomes. Standard therapy consisting of vincristine/doxorubicin/cyclophosphamide/etoposide (Regimen I) plus flank radiation remains effective for stage II–III disease. For stage IV disease, addition of carboplatin to the standard regimen improves survival, although outcomes remain unsatisfactory, with the brain as the most common site of recurrence.
Malignant rhabdoid tumor
Rhabdoid tumors remain the most aggressive pediatric kidney cancer. Intensified chemotherapy has modestly improved survival, a result driven by patients with Stage I/II disease. Despite this improvement, outcomes for patients with rhabdoid tumor remain unsatisfactory and there is a need for novel therapeutic strategies, such as targeting SMARCB1 gene alterations, and immunotherapy approaches.
Why it matters
Families: Some children can avoid radiation or prolonged chemotherapy, reducing long-term side effects.
Clinicians: Clear guidance on when therapy can be reduced – or intensified.
Researchers: New targets like SMARCB1 highlight the need for precision medicine in rhabdoid tumor, where intensification of chemotherapy has had only modest efficacy
Looking ahead
“These studies show real progress in tailoring treatment,” said Dr. Dome. “But the next leap forward will come from biological therapies that directly target the drivers of these cancers.”
With no active frontline trials currently open, the Children’s Oncology Group is designing the next generation of studies to deliver more effective and less toxic therapies for these rare cancers.
Conclusion
From reducing radiation in CCSK to improving survival in FAWT and setting the stage for precision medicine in rhabdoid tumors, these advances are reshaping the outlook for children with rare kidney cancers. At Children’s National, leaders like Dr. Dome are ensuring that even the rarest diagnoses are met with innovation and hope.
The procedure was successfully performed by team in the Esophageal and Thoracic Surgery Program at Children’s National, including Timothy Kane, MD, and Mikael Petrosyan, MD, MBA, who co-authored a case study.
Pediatric surgeons at Children’s National Hospital successfully removed a pediatric esophageal leiomyoma, a rare, benign tumor of the esophagus, through minimally invasive submucosal tunneling and endoscopic resection (STER) rather than the standard of care endoscopic submucosal dissection (ESD) technique that has traditionally had higher complication rates.
A 13-year-old male presented with dysphagia (difficulty swallowing) and frequent abdominal pain and was diagnosed with a 2-cm distal esophageal mass. The team completed full resection of the mass with no complications. At 1-year post-surgery, the patient continued to show no signs of dysphagia, gastroesophageal reflux, or chest pain.
In the case study, the authors write that the successful application of STER “represents a valuable advancement in the endoscopic management of submucosal tumors (SMTs), offering a less invasive and potentially safer approach for tumor removal.”
They assert that while ESD, the current most common approach, also involves removing lesions endoscopically, “ESD involves direct dissection of the lesion, potentially leading to larger mucosal defects and increased risk of complications. STER, with its tunnel approach, maintains mucosal integrity, potentially leading to better outcomes.”
Children’s National leads the way
The Esophageal and Thoracic Surgery Program at Children’s National is a national leader in pioneering more precise and less invasive procedures for children who have diseases and disorders of the lungs, mediastinum and esophagus.
For example, Children’s National performs more peroral endoscopic myotomy (POEM) procedures as a primary intervention for children with esophageal achalasia and pediatric gastroparesis than any other hospital in the United States.
Minimally invasive procedures for children with these conditions are particularly challenging due to a child’s small anatomy and a lack of right-sized surgical tools. The application of endoscopic procedures such as STER and POEM offer fewer risks of complications and faster recovery times than the current standard approaches for children. Though many of these procedures are readily available for adults, applying them in pediatrics requires technical skill and expertise not available everywhere.
Dr. Dome has authored more than 200 articles, books, letters and chapters on pediatric cancer.
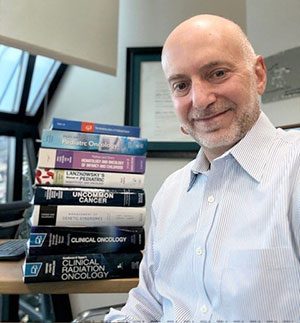
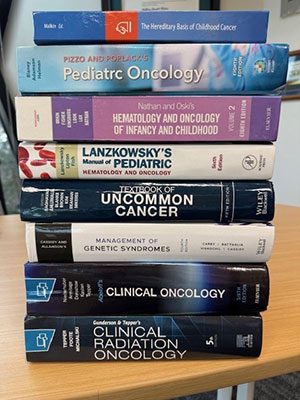
Jeffrey Dome, MD, PhD, senior vice president of the Cancer and Blood Disorders Center at Children’s National Hospital, recently authored chapters for Pizzo and Poplack’s Pediatric Oncology and Abeloff’s Clinical Oncology. These are just two of the internationally recognized oncology textbooks for which Dr. Dome has been invited to serve as senior author, with a focus on Wilms tumor and other pediatric solid tumors.
Contributions to medical textbooks are one of the important avenues for leading oncologists to share their expertise and knowledge with other specialists and medical students.
“Being invited to contribute to these textbooks is both an honor and a responsibility, it’s one way I can give back to the field and help prepare the next generation of physicians,” says Dr. Dome. “I like to tell people that at Children’s National, we don’t just follow the recipes for treatment. We write the cookbooks, or in this case, the textbooks.”
About Dr. Dome
Jeffrey Dome, MD, PhD, is senior vice president of the Cancer and Blood Disorders Center at Children’s National and professor of pediatrics at the George Washington University School of Medicine and Health Sciences. He holds the Thomas Willson and Lenore Williams McKnew professorship of pediatric oncology.
Dr. Dome is an internationally recognized expert on pediatric solid tumors, with an emphasis on kidney tumors and sarcomas. He chaired the Children’s Oncology Group (COG) Renal Tumor Committee for more than a decade. He is presently on the Scientific Council of the COG and is past chair of the American Board of Pediatrics Subboard of Hematology/Oncology. Dr. Dome serves on numerous medical advisory boards for cancer foundations and currently is the North American Continental President of the International Society of Pediatric Oncology (SIOP). He has authored more than 200 articles, books, letters and chapters on pediatric cancer.
Other textbook contributions authored by Dr. Dome include
Lanzkowsky’s Manual of Pediatric Hematology and Oncology
Gunderson & Tepper Clinical Radiation Oncology
Cassidy and Allanson’s Management of Genetic Syndromes
Nathan and Oski’s Hematology and Oncology of Infancy and Childhood
Rudolph’s Pediatrics
Raghavan’s Textbook of Uncommon Cancer, 5th Edition
Malkin’s Hereditary Basis of Childhood Cancer
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/08/Dome-and-books-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-08-08 14:07:452025-08-08 14:08:45Textbook contributions that shape pediatric cancer care
Paclitaxel-containing regimens for patients with recurrent Wilms tumor show promising results in a new multi-institutional retrospective study published in Pediatric Blood and Cancer.
Paclitaxel-containing regimens for patients with recurrent Wilms tumor show promising results in a new multi-institutional retrospective study published in Pediatric Blood and Cancer.
“These findings provide an additional treatment option for pediatric oncologists caring for patients with recurrent Wilms tumor and merit prospective evaluations of paclitaxel-based regimens,” says Jeffrey Dome, MD, PhD, senior vice president of the Cancer and Blood Disorders Center at Children’s National Hospital and corresponding author of the study.
The big picture
The study analyzed 28 patients with recurrent or treatment refractory Wilms tumor from 12 institutions who were treated with paclitaxel or nab-paclitaxel. Out of 26 patients with measurable disease, 42.3% of patients demonstrated a partial response and 15.3% demonstrated stable disease for a clinical benefit rate of 57.6%. Two patients treated adjuvantly without measurable disease were without progression for 12 and 16 months.
Moving the field forward
Over the last two decades, heavily pre-treated patients with Wilms tumor have seen few advances in available therapies. A review of 257 patients with recurrent Wilms tumor who enrolled in 79 phase 1 and 2 studies showed objective responses in only 8.5% of patients. Therefore, the response rate observed in this study is noteworthy. The authors note that the strength of this study is the large case series of a rare patient population, which provides a robust dataset of paclitaxel treatment in patients with refractory or recurrent Wilms tumor.
“Our initial observation that paclitaxel-containing regimens showed meaningful activity in several of our patients here at Children’s National prompted us to reach out to colleagues at other leading institutions,” said Dr. Dome. “That collaboration ultimately enabled this multi-institutional effort.”
Additional authors from Children’s National include Amy Frantz, NP, CPNP-AC, and Alissa Groisser, MD.
Children’s National Hospital named Michael D. Keller, MD, as the inaugural Professor of Precision Medicine.
Dr. Keller, a pediatric immunologist, directs the Translational Research Laboratory within the Center for Cancer and Immunology Research (CCIR). He also leads the Jeffrey Modell Diagnostic and Research Center for Primary Immunodeficiency Disorders.
A generous gift from the Indian Paintbrush Foundation endowed this new professorship.
The big picture
Dr. Keller joins a distinguished group of Children’s National physicians and scientists who hold an endowed chair. Altogether, generous donors have funded 51 professorships at the hospital.
Professorships support groundbreaking work on behalf of children and their families. They foster discoveries and innovations. They honor the recipient’s achievements and the donor’s commitment to advancing knowledge.
Why it matters
Dr. Keller’s research focuses on adoptive T-cell therapies for treating infections in immunocompromised patients. He seeks to improve outcomes for children with primary immunodeficiency disorders and those undergoing bone marrow transplants for cancer. He leads several Phase I-II studies of virus-specific T-cell therapies.
Dr. Keller has authored many peer-reviewed articles and helped shape guidelines on the treatment and diagnosis of primary immunodeficiency disorders. He is a member of the American Academy of Allergy, Asthma and Immunology; the Clinical Immunology Society; the European Society of Immunodeficiency and the Primary Immunodeficiency Treatment Consortium.
“This professorship will amplify Dr. Keller’s pioneering work, which promises to transform care for children with immunodeficiencies,” says Catherine Bollard, MBChB, MD, Senior Vice President and Chief Research Officer. Dr. Bollard leads the Cell Enhancement and Technologies for Immunotherapy (CETI) Program and holds the Dr. Robert J. and Florence T. Bosworth Distinguished Professorship in Cancer and Transplantation Biology Research.
Moving the field forward
The Indian Paintbrush Foundation’s support enabled Children’s National to establish the professorship. Endowment funds will help Dr. Keller and future chairholders launch bold precision medicine initiatives. Targeted diagnostics and therapies will deliver maximum health benefits with minimal side effects.
“The Indian Paintbrush Foundation’s deep commitment to the well-being of children and families will drive our work to personalize treatment and expand access to care,” says Nathan Kuppermann, MD, MPH, Executive Vice President and Chief Academic Officer. Dr. Kuppermann directs the Children’s National Research Institute and holds the Fight For Children Distinguished Chair of Academic Medicine.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/Michael-Keller-CNRI-v2.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-21 09:05:162026-01-05 17:10:59Michael D. Keller, MD, named as Inaugural Professor of Precision Medicine
One of the first and most important steps in fighting brain tumors is to understand exactly where they are and how big they are – using magnetic resonance imaging (MRI) scans.
Brain tumors are the most common cause of cancer-related death in children. These tumors can be very difficult to treat because they often grow in very delicate areas of the brain. One of the first and most important steps in fighting these tumors is to understand exactly where they are and how big they are – using magnetic resonance imaging (MRI) scans.
Traditionally, doctors have had to look at these scans and manually draw outlines around the tumors. This takes a lot of time and can vary from one doctor to another. But what if artificial intelligence (AI) could help make this easier and more efficient?
A recent international research effort called BraTS-PEDs 2023 (short for Brain Tumor Segmentation in Pediatrics) explored exactly that. This challenge co-led by Children’s National Hospital and Children’s Hospital of Philadelphia invited research teams from around the world – including a team led by Marius George Linguraru, DPhil, MA, MSc – to develop the best AI tools for automatically finding and measuring brain tumors in children’s MRIs.
A global AI competition for pediatric care
The BraTS-PEDs 2023 challenge was the first of its kind focused specifically on children. Teams were given MRI scans from 167 pediatric patients with brain tumors collected by leading consortia – the Children’s Brain Tumor Network, DMG/DIPG Registry – and Collaborative Network for Neuro-oncology Clinical Trials and reviewed by volunteer neuroradiologists from the American Society of Neuroradiology. They used these scans to train their AI programs and then tested them on new cases to see how well they performed. Our team’s algorithm was the best at measuring these tumors.
Most teams used a special type of AI network called a “U-Net,” which is great at looking at images and figuring out shapes and boundaries. The challenge showed that AI can do a very good job at finding the tumor and measuring its volume. However, it was more difficult for AI to accurately mark the small, active parts inside the tumor, known as “enhancing tumor” regions.
These results are a huge step forward. Using AI can help doctors make faster, more precise decisions, and reduce differences between hospitals or between individual doctors.
Why this matters
When doctors can accurately map out a brain tumor, they can plan surgery better, target radiation therapy more precisely, and track how well treatments are working over time. This can lead to fewer side effects and better outcomes for children.
In some cases, timely and accurate measurements can even be the difference between life and death. Having advanced AI tools could mean that children get the right treatments faster and with more confidence.
Looking ahead
The research community is now working on including even more data from different hospitals around the world and making the data and algorithm public, like Children’s National has done here. They also plan to study more types of brain tumors and scans taken after surgery and treatments. In the future, AI could become a regular part of how doctors look at brain tumors — like an extra set of smart eyes that never get tired.
At Children’s National, leaders like Dr. Linguraru are helping turn this vision into reality, giving children with brain tumors a better chance at a healthy future. You can read the full study – BraTS-PEDs: Results of the Multi-Consortium International Pediatric Brain Tumor Segmentation Challenge 2023 – in the MELBA Journal.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/brain-scans-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-14 16:57:502026-01-09 16:03:25New advances in AI help doctors understand pediatric brain tumors
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success.
A novel immunotherapy approach that involves training autologous T cells derived from peripheral blood mononuclear cells (PBMCs) has shown early signs of safety and efficacy in a small pre-clinical model. The approach, pioneered by researchers within the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital, may have future implications for the treatment of intractable pediatric solid tumors such as neuroblastoma.
What it means
Pediatric solid tumors like neuroblastoma remain a major cause of illness and death, because traditional treatments effective for other tumor types have had only limited success. There is an urgent need for innovative strategies to effectively target these tumors.
This study presents another approach to cell therapy that collects peripheral blood mononuclear cells from the patient and teaches them to target and eliminate solid tumor cells through exposure to similar tumor cells in a controlled laboratory setting. The cells are then primed to find and attack the solid tumor cells when reintroduced, an approach known as adoptive immunotherapy.
What’s new
The authors note that more well-established modalities such as CAR-T and TCR-T therapies have also made significant advances and demonstrate clinical promise at battling cancers such as neuroblastoma. However, the approach presented in the paper offers early promise of an additional potential strategy, especially in a context “where simplicity, speed and safety are priorities.”
By using small molecule treatments, the authors induce an immunogenic response in neuroblastoma tumor cells, making them more recognizable and attackable by immune cells. Ex vivo training of PBMCs with treated neuroblastoma cells exhibited strong tumor-killing activity.
The authors highlight a few key differences of this approach versus existing adoptive cellular therapies. The method “is technically straightforward, requiring only small tumor samples and peripheral blood mononuclear cells (PBMCs), and avoids the need for the complex genetic engineering intrinsic to CAR-T and TCR-T manufacturing,” the authors write. This method leverages ex vivo tumor cell modification, which may mitigate systemic toxicities. “Additionally, because our approach is not limited to a few surface antigens, it may expand the repertoire of actionable tumor-associated targets.”
Children’s National leads the way
Children’s National is a leader in the development of cell therapies for a wide range of pediatric conditions, including pediatric cancer, HIV/AIDS, sickle cell disease and others.
This research is the latest development in a decade-plus of focused research in adoptive immunotherapy within the Center for Cancer and Immunology Research and the Sheikh Zayed Institute for Pediatric Surgical Innovation.
What’s next
The authors write that there are several critical areas for future research to advance this approach, including a need to understand the specific T cell component and receptors involved in recognizing tumor antigens. They will also need to explore the longevity of the trained T cell response including studies of the memory and persistence of trained PBMCs to ensure lasting anti-tumor effects. Finally, the team will explore the risk of T cell exhaustion, which could reduce the effectiveness of the therapy over time.
Though work remains, the authors note, “Our findings lay the groundwork for developing this approach into a viable therapy for neuroblastoma and possibly other solid tumors as well.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/06/cancer-cells-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-06-09 10:03:082025-06-09 10:05:08Preliminary study points to efficacy of PBMC-based immunotherapy for neuroblastoma
In a new review article published in The CRISPR Journal, researchers from Children’s National Hospital discuss the progress of gene therapies for sickle cell disease – from preclinical studies to clinical trials and FDA approval – along with the many challenges of these treatments.
Over the past few years, the advances of gene therapy for sickle cell disease (SCD) offer a potential cure for a condition previously managed only through symptom relief and limited treatments. SCD is a hereditary blood disorder caused by a mutation in the beta globin gene leading to painful symptoms and complications.
In a new review article published in The CRISPR Journal, researchers from Children’s National Hospital discuss the progress of gene therapies for SCD – from preclinical studies to clinical trials and FDA approval – along with the many challenges of these treatments.
“We are hoping to bring attention to the past, present and future of this topic,” says Henna Butt, MD, pediatric hematology oncology fellow at Children’s National and one of the review authors. “It is exciting to see the technology move forward and see how far we have come in a disease where so little progress has been made historically.”
The hold up in the field
Gene therapy for SCD remains a time- and resource-intensive process, often taking several months from the initial patient consultation to treatment.
“Progress in SCD gene therapy has been slowed by high costs, limited accessibility and safety concerns, such as off-target effects,” says Dr. Butt. “Additionally, long-term efficacy data is still needed to confirm the durability of these treatments. Regulatory hurdles and ethical considerations also contribute to the delays.”
Moving the field forward
“By using cutting-edge techniques like CRISPR and base editing to directly correct the genetic mutation responsible for SCD, these therapies have the potential to offer long-term or even permanent relief,” says Dr. Butt. “Success in this area could revolutionize treatment options, improve patient outcomes and reduce the global burden of SCD — especially as therapies become more accessible and affordable.”
“Advancing gene therapy for sickle cell disease requires not just scientific innovation, but also the clinical expertise and systems to deliver it safely and effectively,” says David Jacobsohn, MD, SCM, MBAD, chief of Bone and Marrow Transplantation at Children’s National. “As access expands, we must ensure these therapies reach the patients who need them most.”
The patient benefit
Gene therapy offers a potential cure for SCD, reducing the need for ongoing treatments and significantly improving quality of life. It can lower the risk of complications and infections, and over time, reduce healthcare costs – especially for patients with limited access to traditional care. Raising awareness of current challenges can help drive advocacy for affordability and access.
Children’s National leads the way
Children’s National was the first hospital in the world to collect stem cells for the LYFGENIA™ treatment and one of the few pediatric hospitals in the country that offers both FDA-approved sickle cell disease gene therapies – CASGEVY™ (exagamglogene autotemcel) and LYFGENIA™ (lovotibeglogene autotemcel).
A new HIV-specific T cell therapy, tested in six adults living with HIV, used specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
An exciting small clinical trial led by the Center for Cancer and Immunology Research at Children’s National Hospital has shown that a new HIV-specific T cell therapy is safe and may help reduce hidden reservoirs of the virus in the body. This approach, tested in six adults living with HIV, uses specially trained immune cells made from each person’s own blood — a personalized therapy designed to target the virus with precision.
The results, published in Nature Communications, represent a step forward in the search for a long-term, drug-free way to control or even cure HIV.
A smarter way to fight HIV
Today, people living with HIV rely on anti-retroviral therapy (ART) to keep the virus under control. These medications are highly effective but must be taken daily and do not eliminate the virus entirely. That is because HIV can hide in a “reservoir” of cells where it remains dormant and invisible to both drugs and the immune system. If ART is stopped, the virus can quickly return.
To change that, scientists at Children’s National and partnering institutions developed a new type of cellular therapy called HST-NEETs — short for “HIV-specific T cells targeting conserved epitopes”. These T cells are trained in the lab to recognize parts of the virus that do not change much, even as HIV mutates. This makes it harder for the virus to escape. The goal is to help the immune system find and destroy the infected cells that are normally hidden.
Safe and promising results
In this phase 1 clinical trial, researchers created personalized HST-NEET therapy from each participant’s own immune cells. After training the cells to recognize HIV, they were infused back into the patients twice over a period of weeks.
The results showed that:
No serious side effects were reported from the infusions.
The treatment was well-tolerated by all six participants.
In two people, the therapy led to stronger HIV-specific immune responses, including more virus-fighting T cells and antibodies.
In two others, researchers saw a drop in the level of HIV hidden in their cells, a sign that the virus reservoir might be shrinking.
In four participants, the infused T cells persisted in the bloodstream for up to 40 weeks, continuing to patrol for signs of HIV.
While not a cure, these findings show early evidence that the therapy may help the body better recognize and fight HIV, even the hidden forms that are hardest to treat.
Building toward a cure
“The fact that we saw HIV-specific T cell responses increase in some participants, even without additional immune-boosting drugs, is very encouraging,” said Catherine Bollard, MBChB, MD, senior author of the study and director of the Center for Cancer and Immunology Research at Children’s National. “It suggests that the immune system can be trained to go after parts of the virus that were previously out of reach.”
Unlike bone marrow transplants, which have led to a cure in a few people with both HIV and cancer but carry high risk, HST-NEET therapy is much safer and more scalable. That is important for the millions of people living with HIV worldwide.
This study also sets the stage for future clinical trials that could combine T cell therapy with other strategies, like latency-reversing drugs that “wake up” hidden HIV, to further shrink the reservoir. It also shows that personalized T cells can be safely made, infused and tracked over time and that they can continue working in the body for many months. Those lessons are valuable not just for HIV but also for developing safer, more targeted cancer immunotherapies in children and adults.
What’s next
The next phase of research will evaluate this therapy in larger groups and under different conditions, including in people undergoing stem cell transplants or with added immune system boosters. Clinical trials are already underway exploring these combinations.
By focusing on preserved parts of the virus, the regions that HIV cannot easily mutate, HST-NEETs could one day become part of a combination approach to eliminate HIV from the body altogether.
“Every step brings us closer to a functional cure,” said Dr. Bollard. “And the lessons we’re learning from HIV may also inform how we treat other chronic viral infections, and even cancer, in the future.”
Authors authors from Children’s National include Danielle K. Sohai, Michael D. Keller, Patrick J. Hanley, Fahmida Hoq, Divyesh Kukadiya, Anushree Datar, Emily Reynolds, Christopher Lazarski, Chase D. McCann, Jay Tanna, Abeer Shibli, Haili Lang, Anqing Zhang, Pamela A. Chansky, Cecilia Motta and Conrad Russell Y. Cruz.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/tube-rack-in-lab-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-05-23 12:34:312025-05-23 12:35:29Personalized T cell therapy for HIV shows safety and early signs of impact
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-04-22 10:31:052026-04-13 10:39:42REI Week 2025 empowers the future in pediatric research and innovation
Nurse Practitioner Sameeya Ahmed-Winston, CPNP, CPHON, was recognized with the APP Lifetime Achievement Award.
Experts from Children’s National Hospital presented and showcased their latest research at the 2025 Tandem Meetings in Hawaii.
This leading global conference on hematopoietic cell transplantation (HCT), cellular therapy and gene therapy brings together top specialists to share groundbreaking discoveries, innovative technologies and the latest scientific advancements shaping the field.
These achievements highlight Children’s National Hospital’s commitment to advancing research and improving treatments for patients with complex conditions. By sharing their expertise on a global stage, these specialists help shape the future of patient care and improve outcomes for children worldwide
Read more highlights from the 2025 Tandem Meetings here.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/03/tandem-attendees-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-03-05 11:26:542025-03-05 11:29:14Children’s National experts at the 2025 Tandem Meetings
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital.
Jo Lynne Rokita, PhD, is the director of the new Bioinformatics Core housed within the Brain Tumor Institute at Children’s National Hospital. Dr. Rokita is a cancer genomics leader with 20 years of combined research experience in academia, industry and the government. She’s also a technical and analytical expert in genomics research using microarrays and high-throughput sequencing.
“We are very excited that we were able to recruit Dr. Rokita as director of the Bioinformatics Core Facility,” says Muller Fabbri, MD, PhD, associate center director for Cancer and Immunology Research at Children’s National. “Her Bioinformatics Core will play a central role in providing the Brain Tumor Institute community with unique expertise spanning biology/genetics/genomics and bioinformatics and will propel Children’s National forward as a national and worldwide leader in pediatric brain tumor research.”
Dr. Rokita is overseeing the core’s creation, including bringing both bioinformatics staff and computing infrastructure to the program, which will support the data analysis needs of the institute’s investigators. She recently answered questions about the new core and also talked a little bit about the focus of her own research that will continue at Children’s National.
Q: Why is the Brain Tumor Institute establishing a Bioinformatics Core?
A: Growing the institute’s bioinformatics capabilities was one of the things that leadership wanted to make sure was built into the plan for the record-setting $96 million gift that was received in 2023. There was a clear need among the principal investigators for this type of research support which includes organization, analysis and interpretation of large-scale genetic sequencing and other “-omics” data.
Q: How did you decide to join Children’s National?
A: I was leading a pediatric brain tumor focused bioinformatics team at Children’s Hospital of Philadelphia (CHOP). As a part of the Children’s Brain Tumor Network (CBTN), I worked closely with a collaborator from Children’s National, Brian Rood, MD, medical director of the Brain Tumor Institute. He told me about the opportunity and I was very excited to apply.
Q: How did your previous work prepare you for this role?
A: I’ve spent the past 10 years in the pediatric cancer field with the last six focused on brain tumor research. In my various roles at CHOP, I led multiple large-scale genomic analysis efforts, comprehensive data and methods for which we then provided openly to the community. During my postdoctoral fellowship, these efforts included a large neuroblastoma patient-derived cell line “ENCODE” as well as a resource led in collaboration with multiple institutes and the National Cancer Institute funded by Alex’s Lemonade Stand Foundation (ALSF). We further scaled these efforts to build open analytical platforms to empower researchers to build upon our work doing their own cancer genomic analysis. In collaboration with the Childhood Cancer Data Lab at ALSF, we built the platform that ultimately ballooned into the OpenPedCan includes large amounts of harmonized genomic, epigenomic and proteomic data for patients with pediatric cancer. What’s unique is that the data is all processed in the same way and easily accessible through multiple mechanisms. Researchers can use these data to ask questions about the cancer type they study or genes of interest. For example, genes over-expressed, absent and/or mutated in a specific tumor subtype may lead to a better understanding of how a patient’s cancer may respond to a treatment.
We’ll be bringing some of the workflows we created previously here to Children’s National, and that will allow us to join newly generated internal data with the thousands of data points we’ve already harmonized using these workflows.
Q: Can you give us some examples of how data harmonization benefits the field of pediatric brain tumor research?
A: Harmonizing across institutions and databases will help us increase the number of data points available for study. This is really important for rare types of tumors and are major foci of institute collaborator Adriana Fonseca, MD, and her International Rare Brain Tumor Registry program. The Bioinformatics Core will support data organization and analysis for this effort, which aims to sequence the rarest brain tumors — those that make up between only 3% and 5% of all brain tumors. If all the data is analyzed the same way, we can combine multiple studies to increase our total dataset, which in turn may reveal new biomarkers and new subtypes of those tumors. It is critical that we continue to build these data resources in a way that they can be accessed by everyone doing this work. Having dedicated support systems for these functions will push the research farther, faster.
Q: As this work gets underway, what is the core’s main function?
A: As this initiative gets underway, the Bioinformatics Core’s primary goal is to empower investigators by streamlining and centralizing data analyses. We help researchers transfer sequencing data into secure cloud storage, organize newly generated records and prepare those datasets for in-depth study. Our bioinformatics scientists then perform downstream analyses to address the specific questions posed by each investigator. On the backend, we collaborate with information technology at Children’s National to develop a robust infrastructure that supports these activities efficiently. By offering these services in-house, we aim to ensure our investigators have seamless, comprehensive support—ultimately driving innovation and accelerating research progress.
Q: What is “open science” and why is it important in bioinformatics?
A: One of our big focus areas is open science, meaning our goal is to push data and code out into the community so that researchers can easily reproduce and build upon our findings. I’m excited to bring the principles of open science, code sharing and data sharing to the Bioinformatics Core.
Making resources open makes it easier for teams to work together across institutions and research programs. It is also going to benefit patients because people can reuse the code and move towards cures faster. For example, we try to package an entire manuscript’s code when we provide our data so it’s clear how the analyses were done.
Q: What is your particular research passion?
A: I work in several research areas and with many brilliant collaborators. One of our focus areas is understanding how RNA splicing can contribute to pediatric brain tumors to create a change in a protein. We have recently identified tumor-specific splice events in some pediatric brain tumor types and will be partnering with Dalia Haydar, PharmD, PhD, to create therapeutic approaches to targeting these. We are also developing a user-friendly application for mining the large amount of splicing data in pediatric brain tumors.
Another focus of our lab is understanding how the patient’s host genome (alterations inherent in their blood DNA) influences the tumor’s genetics. For example, we’ve just preprinted a study connecting inherited variants to tumor genetics and patient outcomes.
Finally, we are interested in how differences in race, ethnicity and social determinants of health influence survival and treatment outcomes for children with brain tumors.
I am passionate about data sharing, code reproducibility and promoting open science in general.
Q: Is there any specific reason you decided to focus your work around brain tumors and pediatric brain tumors?
A: My cousin passed away from a brain tumor when I was in high school. They didn’t have molecular diagnosis then, but he had a brainstem glioma, likely a diffuse midline glioma. In graduate school, I studied addiction genetics and became fascinated with the brain and towards the end, cancer. As an alumna of Penn State, I was actively involved in philanthropic events raising money for their Dance MaraTHON supporting children with cancer. I was lucky to land a postdoc at CHOP and lean into subsequent roles which allowed my passion for this field to grow.
Q: Last question — What do you do with your time when you are not studying pediatric brain tumor data?
A: I enjoy being with my family, observing my children learn and grow, and listening to music.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/bioinformatics-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-02-26 16:09:002026-04-15 16:25:23Q&A with Dr. Rokita: Building bioinformatics infrastructure at the Brain Tumor Institute
The new partnership will advance pediatric health through innovative discoveries and therapies, with an initial focus on pediatric cancers, including brain tumors.
Children’s National Hospital and Virginia Tech are expanding their research partnership, building on a successful collaboration established in 2019. This partnership will advance pediatric health through innovative discoveries and therapies, with an initial focus on pediatric cancers, including brain tumors.
The partnership brings together Children’s National, ranked among the nation’s top pediatric hospitals by U.S. News & World Report, and Virginia Tech, a leading academic research institution. Together, they aim to deliver transformative advancements to enhance outcomes for children facing devastating diagnoses.
The goals of the research-focused partnership include:
Accelerating the understanding of the biology, improvements in prevention and treatment of pediatric cancers and other childhood diseases.
Developing new diagnostic and therapeutic tools to improve care for children.
Training the next generation of scientists and physician-scientists.
What they’re saying
“Over the years, our partnership with Virginia Tech has demonstrated the power of combining top-tier research expertise with a shared commitment to improving pediatric health,” said Catherine Bollard, MBChB, MD, senior vice president and chief research officer and director of the Center for Cancer and Immunology Research. “This expansion underscores our belief that by working together, we can accelerate discoveries and develop life-changing therapies for children with cancer and other rare diseases.”
“Children’s National Hospital has been an important partner for us in biomedical research and innovation,” said Michael Friedlander, PhD, Virginia Tech vice president for health sciences and technology. “Our collaboration deepened with the launch of Children’s National Research & Innovation Campus in Washington, D.C., and now, as our partnership grows even stronger, we’re poised together to take on some of the biggest challenges in cancer research to contribute to the health of children and adults.”
“Partnering with Children’s National connects us to a world-class clinical trial institute that has been a pioneer in treating brain tumors with focused ultrasound technology, and this presents a unique opportunity to help children and families struggling with cancer,” said Cheng-Chia “Fred” Wu, MD, PhD, a member of the Children’s National Brain Tumor Research Institute and a principal investigator in cancer research and faculty member at the Fralin Biomedical Research Institute in Roanoke and in the Virginia Tech Carilion School of Medicine.“I can’t wait to see where this takes us.”
Big picture
The initial focus of the collaboration is pediatric cancers, including brain tumors — among the most challenging childhood diagnoses. By combining Virginia Tech’s leading-edge technology and research infrastructure with Children’s National’s expertise in pediatric care, the organizations aim to make significant strides in understanding these diseases.
An interdisciplinary approach is at the heart of the ongoing strategy. The collaboration first began with the launch of a 12,000-square-foot Virginia Tech biomedical research facility within the Children’s National Research & Innovation Campus, which opened in 2020. Located on a 12-acre portion of the former Walter Reed Army Medical Center in Washington, D.C., the campus was the nation’s first innovation hub focused exclusively on pediatric research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/boy-getting-eye-exam-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-02-04 13:31:522025-02-04 13:32:49Expanded partnership with Virginia Tech accelerates pediatric cancer research
Anesthesia is used in up to 90% of patients, despite repeated propofol exposure being linked to neurocognitive impairment.
Acute leukemia is the most common childhood cancer, with treatment often involving up to 16 routine lumbar punctures (LPs). Anesthesia is used in up to 90% of patients, despite repeated propofol exposure being linked to neurocognitive impairment. In a quality improvement project, researchers from Children’s National Hospital examined variables that could minimize anesthesia time and propofol exposure for patients. The findings, presented at the 56th Congress of the International Society of Paediatric Oncology in Honolulu, HI., found about half of LPs met the goal of 15 minute of anesthetic exposure with significant differences in completion time between anesthesiologists.
The big picture
Researchers analyzed data from 199 LPs performed in the Non-Operating Anesthesia Room (NOAR) over a six-month period from July to December 2023 – including the start to stop time of anesthetic exposure, type of anesthetic, patient age and body mass index (BMI), proceduralist and anesthesiologist. A P-chart established a center line of 52.5% for procedures being completed within 15 minutes.
What’s next
Plan-Do-Study-Act (PDSA) cycles are being performed to align practices between anesthesiologists and identify successful changes with a goal to raise the center line to 75%.
“These findings highlight our commitment to improving care for children with acute leukemia by reducing anesthesia exposure during lumbar punctures,” said Shelby Smith, RN, MSN, CPNP, CPHON, nurse practitioner at Children’s National and the presenting author. “By identifying factors that impact procedure time and implementing targeted improvements, we aim to enhance patient safety and minimize potential risks associated with repeated propofol use.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/propofol-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-28 12:23:042025-01-28 12:24:10Optimizing anesthesia practices for children with acute leukemia undergoing lumbar punctures
Researchers at Children’s National Hospital are developing supervised autonomous robotic surgery to make expert kidney tumor removal accessible in rural areas, combining robotics, AI and surgeon oversight for safer, more precise outcomes.
Imagine a robot capable of planning and executing the intricate removal of a cancerous kidney tumor — a concept that might sound like science fiction. Yet this groundbreaking work is underway at the Sheikh Zayed Institute (SZI) for Pediatric Surgical Innovation at Children’s National Hospital.
Called Supervised Autonomous Robotic Renal Tumor Surgery (SARRTS), the project aims to prove that a supervised autonomous kidney resection is feasible. Its goal is to enable general surgeons in rural hospitals to oversee robots performing complex resections, democratizing access to specialized surgical care. Backed by a $1 million contract from the Advanced Research Projects Agency for Health (ARPA-H), the initiative represents new opportunities in medical innovation.
“The hope is that, someday, patients will no longer have to travel to major oncology centers to get the best possible surgical outcome when faced with renal tumors,” said Kevin Cleary, PhD, associate director of engineering at SZI. “We hope to combine the precision of robotics with a surgeon’s clinical expertise to create consistently high outcomes.”
The patient benefit
Surgery is a cornerstone of cancer treatment, but access to skilled surgeons remains unevenly distributed nationwide. Autonomous robotic surgery could address this disparity by increasing access to expert-level care, enhancing the precision and consistency of procedures and unlocking new surgical possibilities beyond human surgeons’ capabilities.
Under the initial concept, the SARRTS system will use a combination of CT imaging and 3D mapping from a robot’s RGB-depth camera. While the robot independently plans and executes the incision and tumor resection, the supervising surgeon retains full control, with the ability to approve, modify or halt the procedure at any time — an interplay between human expertise and robotic precision to help ensure safety.
Testing will be conducted on realistic kidney models, called phantoms, which are designed to train and test surgical outcomes. The project aims to validate the feasibility of supervised autonomous tumor resection while advancing technologies that could pave the way for broader applications.
“Robotics and medicine have finally reached a point where we can consider projects requiring this level of complexity,” said Anthony Sandler, MD, senior vice president and surgeon-in-chief at Children’s National and executive director of SZI. By combining autonomous robotics, artificial intelligence and surgical expertise, we can profoundly impact the lives of patients facing life-altering cancer diagnoses.”
Children’s National leads the way
In addition to the kidney surgery initiative, the Children’s National team is pursuing other groundbreaking projects. These include a second ARPA-H contract focused on robotic gallbladder removal and a National Institutes of Health grant to explore robotic hip-pinning, a procedure used to repair fractured hips with pins, screws and plates.
Axel Krieger, PhD, an associate professor of mechanical engineering at Johns Hopkins University, is collaborating closely on the kidney resection and gallbladder projects. The interdisciplinary team believes this state-of-the-art care could be tested and developed within the next decade.
“This particular surgery is complex, and a robot may offer advantages to address difficulties created by patient anatomy and visibility within the surgical field,” said Dr. Sandler. “We can imagine a day – in the not too distant future – when a human and a robotic arm could team up to successfully advance this care.”
This project has been funded in whole with federal funds from ARPA-H under cooperative agreement AY1AX000023.
The Children’s National 2023-2024 Academic Annual Report show on a tablet.
Children’s National Hospital has released its 2023-2024 Academic Annual Report, showcasing a year of transformative progress in pediatric medicine. The report highlights achievements across its research centers, institutes and Innovation Ventures, underscoring the hospital’s role as a leader in advancing child health through innovation and collaboration.
“This year’s report reflects the remarkable progress we have made in advancing the frontiers of pediatric medicine,” said Nathan Kuppermann, MD, MPH, Chief Academic Officer and Chair of Pediatrics. “It highlights groundbreaking work across our research centers, institutes, and Innovation Ventures, showcasing the collaborative spirit that drives our mission forward. These achievements underscore our shared commitment to delivering transformative research and the best possible outcomes for children and families.”
Delivering across centers
The report captures the contributions of each of Children’s National’s research centers, each pushing the boundaries of pediatric healthcare:
Center for Cancer & Immunology Research (CCIR): Delivering on the promise of cell and gene therapies, offering innovative treatments for pediatric cancers and immune disorders.
Center for Genetic Medicine Research (CGMR): Advancing pediatric genetic medicine through interdisciplinary efforts, addressing complex genetic conditions with cutting-edge science.
Center for Neuroscience Research (CNR): A year of growth in scientific excellence, advancing the understanding of brain development and neurological conditions.
Center for Prenatal, Neonatal & Maternal Health Research (CPHNMR): Revolutionizing neonatal care with its pioneering infant brain health neuromonitoring program.
Center for Translational Research (CTR): Facilitating groundbreaking work by new K awardees and driving translational research to bridge the gap between discovery and clinical care.
Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI): Leading the way in advanced research projects in pediatric surgery, pushing technological boundaries to improve outcomes for children worldwide.
Taking the lead in innovation through collaboration
Innovation Ventures at Children’s National is advancing pediatric health security, addressing unique challenges with transformative solutions. Meanwhile, the Children’s National Research & Innovation Campus (CNRIC) continues to thrive as a hub for discovery and collaboration, hosting conferences on topics like artificial intelligence in healthcare, cell and gene therapy, and pediatric epilepsy research.
A vision for the future
The report also highlights Children’s National’s focus on integrating cutting-edge technologies like artificial intelligence into its research and clinical practices, as well as addressing global health challenges such as the effects of climate change on children’s health. These efforts reflect the hospital’s commitment to improving outcomes for children everywhere through innovation, teamwork, and forward-thinking leadership.
The 2023-2024 Academic Annual Report serves as a testament to the dedication and expertise of the Children’s National community, showcasing how collaboration and innovation are shaping the future of pediatric healthcare.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/2023-2024-Academic-Annual-Report-cover-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-13 13:51:482025-01-13 13:53:49Children’s National delivers on the promise in 2024
Meet the winners (left to right): Syed M. Anwar, Ph.D., M.S., principal investigator at Children’s National; Daniel Capellan Martin, M.Sc., Polytechnic University of Madrid; Abhijeet Parida, data scientist at Children’s National; and Austin Tapp, Ph.D., postdoctoral research fellow at Children’s National.
Using an award-winning artificial intelligence (AI) algorithm developed at Children’s National Hospital, researchers ranked first in the world in the Brain Tumor Segmentation-Africa (BraTS-Africa) challenge for their approach to identifying different parts of deadly gliomas. The details of their innovative method were recently published on arXiv, a curated research-sharing platform.
“Technology can bridge the gap in healthcare between high- and low-resource countries,” said Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). “By tailoring methods we created at our hospital to fit the needs of specific regions, such as sub-Saharan Africa, our research helps improve medical imaging and diagnosis in challenging environments.”
Dr. Linguraru was the program chair of the International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI) 2024 in Marrakesh, Morocco, the leading global meeting on AI in medical imaging.
Children’s National leads the way
Gliomas are a type of brain tumor with a high death rate and are especially difficult to diagnose in low- and middle-income countries. Given the increased need in Africa, researchers worldwide came together in Morocco to compete over the best way to accurately detect and measure tumors using MRI data and AI.
By applying advanced machine-learning techniques, the researchers adapted tools initially designed for well-resourced settings to work in countries with far fewer.
The study focused on transfer learning, a process in which an AI model is trained in advance on a large number of brain tumor images and then adjusted to work with smaller sets of new data. In this case, the models were adapted to work with local sub-Saharan African data using a strategy to combine different models’ strengths.
When tested, the approach achieved impressive accuracy scores. The Children’s National team, which included a colleague from the Polytechnic University of Madrid, ranked first in the BraTS-Africa 2024 challenge for identifying different parts of gliomas.
“To make the method widely available, the winning algorithm is shared online for others to use and improve upon,” Dr. Linguraru said. “My favorite part of these competitions is how they highlight the way innovation and collaboration can reduce global healthcare inequalities.”
The big picture
Children’s National researchers consistently lead global events using AI and advanced imaging to tackle complex healthcare challenges. In 2023, the team won a global contest to measure pediatric brain tumors at the MICCAI 2023 Conference. This year’s success in the BraTS-Africa challenge builds on this knowledge base and expands its use to adult gliomas.
At the Radiological Society of North America 2024 annual meeting, which drew 50,000 attendees, Zhifan Jiang, Ph.D., a staff scientist in the Precision Medical Imaging Lab at SZI, also won the Cum Laude Award for his scientific poster on applying AI to radiological images to predict severe outcomes for children with brain tumors caused by neurofibromatosis type 1.
“These achievements show how our science is leading the world in using AI for good,” Dr. Linguraru said. “Every day, we’re building on our knowledge of advanced imaging, brain tumors and AI to improve the diagnosis, measurement and treatment of deadly tumors — on a global scale.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/Brats2024-Team-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-10 17:12:152025-01-10 17:17:51AI for good: Children’s National wins global competitions for measuring brain tumors
More than 100,000 Americans have sickle cell disease, an inherited blood disorder that can cause excruciating pain crises and shorter life expectancies.
Children’s National has one of the largest sickle cell programs in the United States. We are pioneering treatments and provide specialized care to about 1,500 patients each year. We participate in clinical trials to improve outcomes, shorten treatment time, reduce complications and minimize the need for opioids and chemotherapy.
Kendric receives care at Children’s National.
In recognition of our clinical and research excellence, Children’s National was one of a few U.S. pediatric hospitals selected to offer two promising new FDA-approved gene therapies.
Hematologist Robert Sheppard Nickel, M.D., leads a study to reduce toxicities in bone marrow transplants. “Years of development led to these curative therapies,” Dr. Nickel says. “I hope in the future we can safely cure more children with sickle cell disease.”
“The future looks promising to revolutionize the lives of our patients and make these therapies accessible worldwide,” says Andrew Campbell, M.D., director of our Comprehensive Sickle Cell Disease Program.
Kendric and Nasir find hope
In May 2024 at Children’s National, 12-year-old Kendric of Clinton, Maryland, became the world’s first patient with sickle cell disease to begin a commercially approved gene therapy that could dramatically reduce or even eliminate his pain. It involved extracting his bone marrow stem cells; genetically modifying them in a specialized lab to reduce the risk of sickling; and then, after chemotherapy, infusing them back into his bloodstream.
Expert, compassionate care empowered Kendric to understand the science behind his treatment and chart a path to recovery. “My care team taught me how to deal with my disease and everything that I need to know for the future,” he says. “They gave me hope that I could be cured.”
Nasir and his care team.
Nasir, age 20, spent his childhood waiting to find a match for a stem cell transplant to address his sickle cell disease. Finally, in 2023, at Children’s National, he found an answer in gene therapy to alter his own cells.
Due to painful episodes and the need for frequent blood transfusions, both Kendric and Nasir missed out on a lot of school, important moments with friends and simply being kids. Now, they can explore a world in which patients like themselves can overcome this disease and reclaim their health.
“I have all of this oxygen and energy that came out of nowhere,” Nasir says. “It’s really a new life. I feel reborn.”
“The network of doctors at Children’s National gave us reassurance and lots of hope,” says Kendric’s mom, Deborah. “They made us feel like family. We are in awe of how quickly things moved and how much compassion they have shown us.”


 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.




 Children’s National Hospital named Michael D. Keller, MD, as the inaugural Professor of Precision Medicine.
Children’s National Hospital named Michael D. Keller, MD, as the inaugural Professor of Precision Medicine.