Javad Nazarian, Ph.D., has been named scientific director of the Brain Tumor Institute of the Children’s National Health System. Since 2006, Dr. Nazarian has been an active member of the Brain Tumor Institute, contributing to the advancement in understanding pediatric brain tumors.
He has been instrumental in his role as a Principal Investigator in the Center for Cancer and Immunology Research where his laboratory actively investigates the molecular mechanisms of diffuse intrinsic pontine gilomas (DIPGs) and establishes preclinical models of pediatric brain tumors.
Dr. Nazarian has also contributed to the expansion of the comprehensive biorepository at Children’s National, growing from 12 samples six years ago to more than 3,000 specimens donated by more than 900 patients with all types of pediatric brain tumors, including DIPG. Recently he was appointed Scientific Co-chair of the Children’s Brain Tumor Tissue Consortium.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-02-08 11:52:142017-06-01 16:09:27Javad Nazarian named scientific director of the Brain Tumor Institute
As chief research officer, Vittorio Gallo, Ph.D., will be instrumental in developing and realizing Children’s Research Institute’s long-term strategic vision.
Children’s National Health System has appointed the longtime director of its Center for Neuroscience Research, Vittorio Gallo, Ph.D., as Chief Research Officer. Gallo’s appointment comes at a pivotal time for the institution’s research strategic plan, as significant growth and expansion will occur in the next few years. Gallo is a neuroscientist who studies white matter disorders, with particular focus on white matter growth and repair. He is also the Wolf-Pack Chair in Neuroscience at Children’s Research Institute, the academic arm of Children’s National.
As Chief Research Officer, Gallo will be instrumental in developing and realizing Children’s Research Institute’s long-term strategic vision, which includes building out the nearly 12-acre property once occupied by Walter Reed National Military Medical Center to serve as a regional innovation hub and to support Children’s scientists conducting world-class pediatric research in neuroscience, genetics, clinical and translational science, cancer and immunology. He succeeds Mendel Tuchman, M.D., who has had a long and distinguished career as Children’s Chief Research Officer for the past 12 years and who will remain for one year in an emeritus role, continuing federally funded research projects and mentoring junior researchers.
“I am tremendously pleased that Vittorio has agreed to become Chief Research Officer as of July 1, 2017, at such a pivotal time in Children’s history,” says Mark L. Batshaw, M.D., Physician-in-Chief and Chief Academic Officer at Children’s National. “Since Mendel announced plans to retire last summer, I spent a great deal of time talking to Children’s Research Institute investigators and leaders and also asking colleagues around the nation about the type of person and unique skill sets needed to serve as Mendel’s successor. With each conversation, it became increasingly clear that the most outstanding candidate for the Chief Research Officer position already works within Children’s walls,” Dr. Batshaw adds.
“I am deeply honored by being selected as Children’s next Chief Research Officer and am excited about being able to play a leadership role in defining the major areas of research that will be based at the Walter Reed space. The project represents an incredible opportunity to maintain the core nucleus of our research strengths – genetics, immunology, neurodevelopmental disorders and disabilities – and to expand into new, exciting areas of research. What’s more, we have an unprecedented opportunity to form new partnerships with peers in academia and private industry, and forge new community partnerships,” Gallo says. “I am already referring to this as Walter Reed ‘Now,’ so that we are not waiting for construction to begin to establish these important partnerships.”
Gallo’s research focus has been on white matter development and injury, myelin and glial cells – which are involved in the brain’s response to injury. His past and current focus is also on neural stem cells. His work in developmental neuroscience has been seminal in deepening understanding of cerebral palsy and multiple sclerosis. He came to Children’s National from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) intramural program. His intimate knowledge of the workings of the National Institutes of Health (NIH) has helped him to establish meaningful collaborations between both institutions. During his tenure, he has transformed the Center for Neuroscience Research into one of the nation’s premier programs. The Center is home to the prestigious NIH/NICHD-funded District of Columbia Intellectual and Developmental Disabilities Research Center, which Gallo directs.
Children’s research scientists working under the auspices of Children’s Research Institute conduct and promote highly collaborative and multidisciplinary research within the hospital that aims to better understand, treat and, ultimately, prevent pediatric disease. As Chief Research Officer, Gallo will continue to establish and enhance collaborations between research and clinical programs. Such cross-cutting projects will be essential in defining new mechanisms that underlie pediatric disease. “We know, for instance, that various mechanisms contribute to many genetic and neurological pediatric diseases, and that co-morbidities add another layer of complexity. Tapping expertise across disciplines has the potential to unravel current mysteries, as well as to better characterize unknown and rare diseases,” he says.
“Children’s National is among the nation’s top seven pediatric hospitals in NIH research funding, and the extraordinary innovations that have been produced by our clinicians and scientists have been put into practice here and in hospitals around the world,” Dr. Batshaw adds. “Children’s leadership aspires to nudge the organization higher, to rank among the nation’s top five pediatric hospitals in NIH research funding.”
Gallo says the opportunity for Children’s research to expand beyond the existing buildings and the concurrent expansion into new areas of research will trigger more hiring. “We plan to grow our research enterprise through strategic hires and by attracting even more visiting investigators from around the world. By expanding our community of investigators, we aim to strengthen our status as one of the nation’s leading pediatric hospitals,” he says.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/01/Vittorio-Gallo.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-01-12 14:42:342017-06-07 14:19:12Vittorio Gallo named Chief Research Officer
Children’s National Health System and Celsion Corp., a leading oncology drug-development company, will be the first to launch a clinical study in the U.S. that evaluates the use of ThermoDox®, a heat-activated chemotherapy drug, in combination with noninvasive magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) to treat refractory or relapsed solid tumors in children and young adults.
The investigator-sponsored Phase I study, which is partially funded by an NIH R01 grant, will determine a safe and tolerable dose of ThermoDox, a lyso-thermosensitive liposomal doxorubicin (LTLD), which can be administered in combination with MR-HIFU. Under the guidance of an MRI, the high-intensity focused ultrasound directs soundwave energy to heat the tumor and the area around the tumor. When heated, the liposome rapidly changes structure and releases doxorubicin directly into and around the targeted tumor.
“There is currently no known cure for many patients with refractory recurring solid tumors, despite the use of intensive therapy, so we need to identify new, smarter therapies that can improve outcomes,” said AeRang Kim, M.D., Ph.D., oncologist and member of the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National, who is also principal investigator for the study. “Recent advances in the use of noninvasive MR-HIFU coupled with novel therapies, such as LTLD, may provide us with a mechanism to noninvasively administer high concentrations of the drug directly to the site where it is most needed and avoid toxicity to other areas of the body.”
A First to Treat Childhood Cancer
This is the first time LTLD is being combined with MR-HIFU and the first time it is being evaluated in children.
“Celsion’s experience in combining ThermoDox with HIFU, a noninvasive next generation heating technology, supports this very important research in childhood cancers. From a safe dose, ThermoDox’s proven ability to deliver high concentrations of an effective chemotherapy directly to a heated tumor makes it an ideal candidate for a trial involving children and young adults,” said Michael H. Tardugno, Celsion’s chairman, president and CEO. “This study will further elucidate ThermoDox’s potential in combination with ultrasound-induced hyperthermia, and highlight potential applications of ThermoDox in combination with a broad range of heating technologies that could address an even larger population of patients.”
A Multidisciplinary Approach
The study targeting the treatment of childhood sarcomas will be carried out as a multidisciplinary collaboration between Children’s National, Celsion, and Dr. Bradford Wood’s team at the National Institutes of Health.
ThermoDox is currently in late-stage clinical trials in primary liver cancer and recurrent chest wall breast cancer. It is positioned for use with multiple heating technologies, and has the potential for applications in the treatment of other forms of cancer including metastatic liver and nonmuscle invading bladder cancers.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/01/hifu_hp.jpg533800Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-01-06 14:37:182024-05-16 14:49:15Study to evaluate heat-activated chemotherapy drug
Roger Packer, M.D., Senior Vice President for the Center of Neuroscience and Behavioral Medicine and Director of the Brain Tumor Institute at Children’s National Health System, will be speaking at the 21st Annual Meeting and Education Day of the Society for Neuro-Oncology. From November 17-20, 2016, the conference will gather neuro-oncologists, medical oncologists, adult and pediatric neurosurgeons, pediatric neuro-oncologists, neuroradiologists, neuropathologists, radiation oncologists, neuropsychologists, and epidemiologists from across the country to discuss the future of neuro-oncology. Dr. Packer will be sharing his expertise in treating neurofibromatosis and pediatric brain tumors. He also will be part of a working group to discuss guidelines for response assessment in PDCT-13 medulloblastoma and other leptomeningeal seeding tumors.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-11-08 14:35:132018-11-26 16:10:25Brain tumor expert from Children’s National speaks at Society for Neuro-Oncology’s scientific meeting and Education Day
Roger Packer, MD, Senior Vice President for the Center of Neuroscience and Behavioral Medicine and Director of the Brain Tumor Institute at Children’s National Health System, was an invited speaker at the Coalition Against Childhood Cancer meeting at Cold Springs Harbor Laboratory on October 31 and November 1, 2016. This international conference was a unique collaborative effort between multiple foundations, the National Cancer Institute, and industry experts to develop a new path forward for the treatment of childhood cancer. Dr. Packer spoke on “Pediatric Brain Tumors: Where Are We Now” and shared his expertise in treating pediatric brain tumors and what he hopes the future of pediatric brain tumor research will look like. Pediatric brain tumors recently surpassed leukemia as the most deadly form of childhood cancer.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.png00Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-11-08 11:56:222024-03-29 10:31:48Brain Tumor Institute Director Speaks at Coalition against Childhood Cancer Meeting
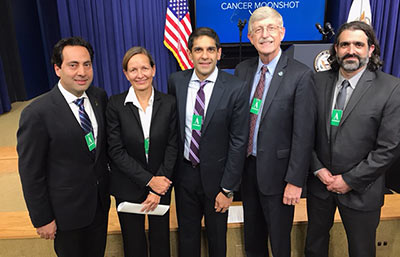
Dr. Nazarian’s lab at Children’s is part of the CBTTC, which has helped in launching CAVATICA. Pictured (from left to right): Dr. Nazarian, Sabine Mueller, M.D., Ph.D. (PNOC Trial Director), Rishi Lulla, M.D. (CBTTC Executive Director), Francis Collins, M.D., Ph.D., (NIH Director), and Adam Resnick, PHD (CBTTC Scientific Director).
Earlier this week, The White House released the Cancer Moonshot report, which calls upon the public and private sectors to transform cancer research and care. Children’s National’s Javad Nazarian, Ph.D., M.S.C., joined peers from prestigious children’s hospitals from around the world at the news conference. Dr. Nazarian is a key player in the initiative, as his lab is part of the Children’s Brain Tumor Tissue Consortium (CBTTC) and is answering the call to action. The CBTTC and the Pacific Pediatric Neuro-Oncology Consortium, in partnership with Seven Bridges, announced the launch of CAVATICA, a data analysis platform that will help researchers to collaboratively access and share data about pediatric cancers, congenital disorders and rare diseases such as epilepsy and autism. More data will be connected than ever before—CAVATICA will interoperate with the Genomic Data Commons and other NIH data repositories. “It’s an exciting time for research,” says Dr. Nazarian.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/10/WH-Cavatica.jpg11261500Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-10-20 13:43:052025-02-28 12:30:17Pediatric research consortia unveil CAVATICA data platform
Children diagnosed with cancer face fear and uncertainty, a series of medical appointments, and multiple diagnostic tests and treatments.
Children diagnosed with cancer face fear and uncertainty, a series of medical appointments, and multiple diagnostic tests and treatments. On top of these challenges, says Children’s National Health System urologist Michael Hsieh, M.D., Ph.D., many patients contend with additional issues: Treatment side effects, discomforts, and dangers that nearly eclipse that of the cancer itself. One of the most common side effects is hemorrhagic cystitis (HC), a problem marked by extreme inflammation in the bladder that can lead to tremendous pain and bleeding.
HC often results from administering two common chemotherapy drugs, cyclophosphamide and ifosfamide, used to treat a wide variety of pediatric cancers, including leukemias and cancers of the eye and nerves. In the United States alone, nearly 400,000 patients of all ages receive these drugs annually. Of these, up to 40 percent develop some form of HC, from symptomatic disease characterized by pain and bloody urine to cellular changes to the bladder detected by microscopic analysis.
“Having to deal with therapy complications makes the cancer ordeal so much worse for our patients,” says Dr. Hsieh, Director of the Clinic for Adolescent and Adult Pediatric Onset Urology at Children’s National. “Being able to eliminate this extremely detrimental side effect once and for all could have an enormous impact on patients at our hospital and around the world.”
Preventing complications with mesna
The severity of side effects from cyclophosphamide and ifosfamide can vary from mild and fleeting to bladder bleeding so extensive that patients require multiple transfusions and surgery to remove blood clots that can obstruct urinary release, says Dr. Hsieh, who frequently treats patients with this condition. But HC isn’t inevitable, he adds. A drug called mesna has the potential to prevent this complication when prescribed before a patient receives chemotherapy.
The problem is for a fraction of patients, mesna simply doesn’t work. For others, mesna can cause its own serious side effects, such as life-threatening malfunctions of the heart’s electrical system or allergic reactions.
“These kids are often already very sick from their cancers and treatments, and then you compound it with these complications,” says Dr. Hsieh. “There’s a desperate need for alternatives to mesna.”
Looking at alternative treatments
In a new review of the scientific literature, published August 24 by Urology, senior author Dr. Hsieh and a colleague detail all the substitutes for this drug that researchers have examined over several years.
One of these is hyperhydration, or delivering extra fluid intravenously to help flush the bladder and keep dangerous chemotherapy drug metabolites from accumulating and causing damage. Hyperhydration, however, isn’t an option for some patients with kidney, lung, or liver problems, who can’t tolerate excess fluid.
Researchers also have invested heavily in antioxidants as alternative treatments. Because much of the damage caused by these chemotherapy agents is thought to result from a cascade of oxidizing free radicals that cyclophosphamide and ifosfamide launch in the bladder, antioxidants might prevent injury by halting the free radical attack. Antioxidants that researchers have explored for this purpose include cytokines, or immune-signaling molecules, known as interleukin-1 and tumor necrosis factor, and a compound called reduced glutathione. Other studies have tested plant-based antioxidants, including a component of red wine known as resveratrol; a compound called diallyl disulfide isolated from garlic oil; and extracts from Uncaria tomentosa, a woody vine commonly known as “cat’s claw” that grows in the jungles of Central and South America.
Researchers also have tested options that focus on reducing the intense inflammation that cyclophosphamide and ifosfamide cause in the bladder, including the corticoid steroid drug dexamethasone as well as another cytokine known as interleukin-4.
However, Dr. Hsieh says, studies have shown that each of these treatments is inferior to mesna. To truly combat HC, researchers not only need to find new drugs and methods that outperform mesna but also new ways to reverse HC after other measures fail—problems he’s working to solve in his own lab.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/07/Michael-Hsieh.jpg400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-10-19 10:00:222018-05-30 11:36:48Finding new ways to fight hemorrhagic cystitis for cancer patients
Mutations in histone-encoding genes are associated with the vast majority of pediatric DIPG cases.
For more than four decades, clinicians around the nation have been giving the parents of pediatric patients diagnosed with diffuse intrinsic pontine glioma (DIPG) the same grim prognosis. In the past five years, there has been an explosion of innovative research at Children’s National Health System and elsewhere that promises to change that narrative. That’s because the black box that is DIPG is beginning to divulge its genetic secrets. The new-found research knowledge comes as a direct result of parents donating specimens, judicious shepherding of these scarce resources by researchers, development of pre-clinical models, and financing from small foundations.
From just 12 samples six years ago, Children’s National has amassed one of the nation’s largest tumor bio banks – 3,000 specimens donated by more than 900 patients with all types of pediatric brain tumors, including DIPG.
Such donated specimens have led to the identification of H3K27M mutations, a groundbreaking finding that has been described as the single-most important discovery in DIPG. Mutations in histone-encoding genes are associated with the vast majority of pediatric DIPG cases.
Histone mutations (also referred to as oncohistones) are sustained in the tumor throughout its molecular evolution, found a research team led by Javad Nazarian, Ph.D. Not only were H3K27M mutations nearly ubiquitous in all samples studied, the driver mutation maintained partnerships with other secondary mutations as DIPG tumor cells spread throughout the developing brain. Children’s National researchers have identified tumor driver mutations and obligate partner mutations in DIPG. They are examining what happens downstream from the histone mutation – changes in the genome that indicate locations they can target in their path toward personalized medicine. The value of that genomic knowledge is akin to emergency responders being told the specific house where their help is needed, rather than a ZIP code or city name, Dr. Nazarian says. While there is currently no effective treatment for DIPG, new research has identified a growing number of genomic targets for future therapeutics.“That changed the dynamic,” says Dr. Nazarian. “In DIPG clinical research, nothing had changed for 45 years. Now we know some of the genomic mutations, how the tumor was evolving – gaining new mutations, losing mutations. With precision medicine, we can target those mutations.”
Another study led by neuro-oncologist Eugene Hwang, M.D., reported the most comprehensive phenotypic analyses comparing multiple sites in a young girl’s primary and metastatic tumors. This study showed that despite being uniform, small molecules (mRNA) could be used to distinguish an evolved tumor from its primary original tumor mass.Key to this multidisciplinary work is collaboration across divisions and departments. Within the research lab, knowledge about DIPG is expanding.
Each member of the DIPG team – neurosurgery, neuro-oncology, immunology, genomics, proteomics – feeds insight back to the rest of the team, accelerating the pace of research discoveries being translated into clinical care. Among the challenges that the team will address in the coming months is outmaneuvering tumors that outsmart T-cells (immune cells).
“What is happening in the checkpoint inhibitor field is exciting,” says Catherine M. Bollard, MBChB, MD, Chief of Allergy and Immunology and Director of the Program for Cell Enhancement of Technologies for Immunotherapy. “The inhibitors work by reversing the ‘off’ switch – releasing the brake that has been placed on the T-cells so they can again attack multiple tumor proteins. The next exciting step, and novel to Children’s National, will be to combine this approach with T-cell therapies specifically designed to attack the DIPG tumors. Unlike the use of combination chemotherapy, which has had a limited impact, we hope that the novel combination of immunotherapeutic approaches will offer the hope of a potential cure.”
Dr. Hwang, another member of the multidisciplinary team, adds: “When you’re looking at the landscape – for me, at least – it starts and ends with how my patients are doing. There are kids for whom we have had great successes in improving survival rates in some cancers, like leukemia, and some where the needle has moved nowhere, like DIPG. We’re still trying to figure out the whole picture of who responds. The immune system is present in all kids. Its ability to attack is present in all kids.”
Children’s National is one of the few hospitals in the nation that conducts brainstem biopsies for DIPG and does so with very little chance of complications. The pons is like a superhighway through which nerves pass, making it instrumental in smooth operation of such vital functions as breathing, heart rate, sleeping, and consciousness. The ability of neurosurgeon Suresh Magge, MD, to perform such sensitive biopsies upends conventional wisdom that these procedures were inherently too dangerous. Within two weeks of diagnosis, genomics analyses are run to better understand the biology of that specific tumor. Within the following weeks, the tumor board occurs, and patients with DIPG are placed on therapy that best targets their tumor’s mutations.
The black box that is diffuse intrinsic pontine glioma is beginning to divulge its genetic secrets.
Despite an increasing number of experimental therapies tested via clinical trials, more than 95 percent of children with DIPG die within two years of diagnoses. Biomarkers that point to DIPG – like the copies of DNA that tumors shed and leave behind in the bloodstream – could enable creation of liquid biopsies, compared with today’s surgical approach.
Children’s also is making a concerted effort to create preclinical models of DIPG. Preclinical models will be used to winnow the field of potential therapeutics to the candidates most likely to help children survive DIPG. The preclinical tumor cells will be labeled with luciferase – enzymes that, like photoproteins, produce bioluminescence – permitting the researcher to visually see the formation, progression, and response of DIPG tumors to treatment in preclinical settings.
These preclinical models could be used to test multiple drug combinations in conjunction with radiation therapy. Molecular signatures and response to treatment could then be assessed to learn how the tumor resists therapy. Due to the obligate partnerships between driver mutations and secondary mutations, the research team already knows that effective DIPG medicines will need more than one target. If there were a single mutation, that would be like having a single master key to open many locks. Multiple mutations imply that more than one key will be needed. Thus, the search for cures for DIPG will necessitate taking a multi-pronged approach.
Combined drug regimens, including those created with proprietary technology, with or without radiation, will be keys to targeting myriad mutations in order to kill tumors where they are. Those drug combinations that demonstrate they can do their jobs – slowing tumor growth, increasing chances of survival, taming toxicity – will be selected for clinical application.
Immunotherapy leverages T-cells, the immune system’s most able fighters, to help in the overall goal of extending patients’ survival. One of the most challenging aspects of pediatric brain tumors is the body does a very good job of shielding the brain from potential pathogens. Precise drug delivery means finding innovative ways for therapeutics to cross the blood-brain barrier in order to reach the tumor. The team has identified one such potential target, the protein NG2, which may represent a good target for immune therapy. The protein is expressed in primitive cells that have not become specialized – meaning there may be an opportunity to intervene before it is driven to become a tumor cell.
June 6, 2016 –Targeting tumors more precisely, with fewer lasting side effects for kids
Pediatric patients with cancer are often treated with a cocktail of therapies to attack the disease through a variety of mechanisms. While this approach has been instrumental in saving children’s lives, the life-saving therapies can be accompanied by acute side effects, and the treatments may have lingering impacts as cancer survivors enter adulthood. Magnetic resonance-guided high-intensity focused ultrasound (MR-HIFU) holds the promise of surgically removing large tumors without exacting the same array of harsh side effects. Ultrasound relies on high-frequency sound waves to make diagnostic images, and those same sound waves can be used therapeutically to destroy tumors. Layering on MR imaging gives clinicians the ability to precisely guide the ultrasound therapy in real time. A study led by Children’s National Health System researchers and clinicians is using MR-HIFU for the first time in children to examine its safety and feasibility.
May 11, 2016 – Quantitative MRI criteria for optic pathway enlargement in neurofibromatosis type 1
Symptoms of neurofibromatosis type 1 (NF1) vary widely, but the condition is characterized by changes in skin pigmentation and growth of tumors along nerves. The research team sought to determine quantitative size thresholds for enlargement of the optic nerve, chiasm, and tract in children aged 0.5 to 18.6 years with NF1. The study, published in Neurology, found that quantitative reference values for anterior visual pathway enlargement will enhance development of objective diagnostic criteria for optic pathway gliomas secondary to NF1.
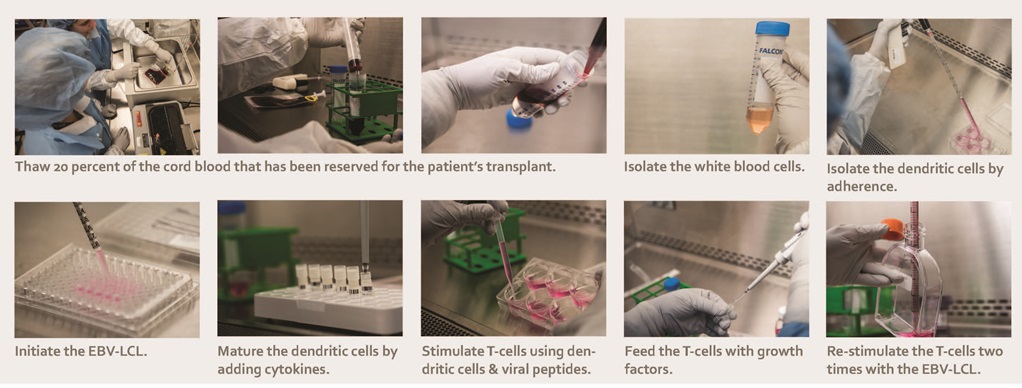
What’s Known Children’s National Health System is the only pediatric hospital in the nation that grows personalized T-cells from naïve cord blood (CB), training these CB-derived cells to simultaneously fight adenovirus, cytomegalovirus, and Epstein-Barr virus to control viral infections after transplantation. Here are a number of the critical steps during that three-month manufacturing process.
Source: P.J. Hanley, J. J. Melenhors, S. Nikiforow, P. Scheinberg, J.W. Blaney, G. Demmler-Harrison, C.R. Cruz, S. Lam, R.A. Krance, K.S. Leung, C.A. Martinez, H. Liu, D.C. Douek, H.E. Heslop, C. M. Rooney, E.J. Shpall, A.J. Barrett, J.R. Rodgers, and C.M. Bollard. “CMV-Specific T-Cells Generated From Naïve T-Cells Recognize Atypical Epitopes and May Be Protective In Vivo.” Published by Science Translational Medicine on April 29, 2015
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GImage_Expanding-Cytotoxic-T-Lymphocytes_sm.jpg401600Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-07-27 10:14:172022-02-28 10:03:28Expanding cytotoxic T lymphocytes from umbilical cord blood to target three viruses
Patients with leukemia, lymphoma, other cancers, and genetic disorders who receive stem cell or cord blood transplants face the post-transplant risk of developing a life-threatening infection with adenovirus, cytomegalovirus (CMV), or Epstein-Barr virus (EBV).
The study reports the results of a head-to-head comparison of two powerful immunotherapeutic strategies to thwart such viral infections. Both therapeutic approaches leverage the power of multivirus-specific, donor-derived T-cells (mCTL), which are highly skilled at recognizing foreign invaders and, in the case of the peripheral blood cells, have long memories of past battles.
The award-winning paper, “Multivirus-Specific T Cells From Both Cord Blood and Bone Marrow Transplant Donors” was presented during the International Society for Cellular Therapy (ISCT) 2016 Annual Meeting, held from May 25 through May 28, in Singapore. The abstract’s lead author, Patrick J. Hanley, PhD, Laboratory Facility Director of Children’s Cellular Therapy and Stem Cell Processing facility, was recognized by ISCT with a Young Investigator award during the meeting.
Nine research scientists and clinicians affiliated with Children’s National Health System are co-authors of a paper, including Michael D. Keller, MD, the lead clinical investigator of the peripheral blood T-cell study, and Catherine M. Bollard, MBChB, MD, the study’s sponsor and Director of Children’s National Program for Cell Enhancement and Technologies for Immunotherapy.
After certain treatments, some cancer patients’ bodies are stripped of their natural ability to fight infection. The stem cell or the cord blood transplant restores the body’s ability to produce a full complement of blood cells, including infection-fighting white blood cells. As a further boost to these patients, the T-cells are trained to spot and neutralize all three potentially lethal viruses (CMV, EBV, and adenovirus) simultaneously. The personalized cell therapy can be accomplished in a single infusion and administered in the outpatient setting.
In the phase I perspective study, the personalized T-cells were grown from peripheral blood (PB) of adult donors who were seropositive for CMV, a relative of the virus that causes chickenpox, and were also coaxed to grow from naïve cord blood (CB). These naïve cells need additional training since they have never been to battle.
Since the mid-1990s, PB has been shown to be effective for such use. Hanley says that fewer than one dozen facilities in the United States perform PB antiviral T-cell infusions. Of that selective group, Children’s National is the only U.S. location that also grows the specialized T-cells from naïve CB, a procedure that takes a bit longer to accomplish but can help patients whose blood type is in short supply.
Thirteen patients were infused with PB mCTL, and 12 patients were infused with the T-cells derived from cord blood. Patients received their transfusions from 35 to 384 days after their stem cell or cord blood transplant. Within four weeks, the research team saw up to a 160-fold increase in virus-specific T-cells, a development that coincided with patients’ response to therapy. “The overall … response rate in both groups was 81 percent,” writes Hanley and colleagues.
Eight patients had a complete response. Five had a partial response. Nine remain free of infection/reactivation. What’s more, the patients’ restored immunity was durable with at least one patient remaining free of infection two years after treatment – without the need for pharmaceuticals administered in a hospital setting, which exacts a higher overall cost to the healthcare system.
“This study demonstrates that mCTL derived from the PB of seropositive donors, as well as the CB of virus naïve donors, expand in vivo and are active against multiple viruses. Furthermore, by restoring immunity to multiple viruses simultaneously, the need for continued prophylaxis with pharmacotherapy is eliminated, thus, improving the efficiency and cost-effectiveness of protecting SCT and CBT recipients from these potentially lethal viruses,” Hanley and co-authors conclude.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/08/TCell.jpg337500Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-07-27 00:50:012017-06-03 14:22:42New research shows success training t-cells to recognize and fight life-threatening viruses
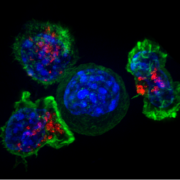
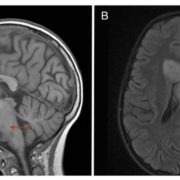
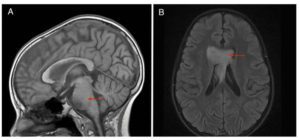
What’s Known Despite multiple clinical trials testing an assortment of new treatments, the survival rate for diffuse intrinsic pontine glioma (DIPG) remains abysmal, with most children succumbing to the pediatric brainstem tumor within 12 months of diagnosis. Focal radiation therapy, the primary treatment approach, has not improved overall survival. While the majority of DIPG tumors grow within the brainstem, metastases can occur elsewhere in the brain. Due to recent availability of tissue, new data are emerging about the biologic behavior of tumors, details that could be instrumental in constructing optimal treatment strategies.
What’s New
An otherwise healthy 9-year-old girl developed weakness in the left side of her face; magnetic resonance imagining revealed T2/FLAIR hyperintensity centered within and expanding the pons. Despite various treatments, her pontine lesion increased in size and new metastases were noted. The team led by Children’s National Health System researchers is the first to report comprehensive phenotypic analyses comparing multiple sites in primary and distant tumors. All tumor sites displayed positive staining for the H3K27M mutation, a mutation described in more than two-thirds of DIPGs that may portend a worse overall survival. Persistence of mutational status across multiple metastatic sites is particularly important since the effectiveness of some therapeutic approaches relies on this occurring. mRNA analyses, by contrast, identified a small number of genes in the primary tumor that differed from one metastatic tumor. This divergence implies that a single biopsy analysis for mRNA expression has the potential to be misleading.
Questions for Future Research Q: Because a small cohort of genes in the girl’s primary tumor were different from genes in portions of the metastatic tumor, would genomic and proteomic analyses provide additional details about this genetic evolution? Q: How do site-specific differences in mRNA expression affect decisions about which therapies to provide and in which order?
Source: “Histological and Molecular Analysis of a Progressive Diffuse Intrinsic Pontine Glioma and Synchronous Metastatic Lesions: A Case Report.” J. Nazarian, G.E. Mason, C.Y. Ho, E. Panditharatna, M. Kambhampati, L.G. Vezina, R.J. Packer, and E.I. Hwang. Published by Oncotarget on June 14, 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@G_Histological-DIPG-image.jpg326700Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-06-14 17:10:192024-02-02 14:39:53Analysis of a progressive diffuse intrinsic pontine glioma: a case report
What’s Known
Following treatment, patients with leukemia, lymphoma, and other cancers may receive a transplant in order to restore their body’s natural ability to fight infection and, sometimes, such transplants are a component of leukemia treatment. (Leukemia is the second most common blood cancer, after lymphoma, and its incidence rate has increased by 0.2 percent annually from 2002 to 2011.) A stem cell or cord blood transplant restores the body’s ability to produce infection-fighting white blood cells. After such transplants, however, patients can face heightened risk of developing a life-threatening infection with such viruses as adenovirus, cytomegalovirus, or Epstein-Barr virus.
What’s New
A head-to-head comparison of two strategies to thwart such viral infections shows that both approaches leverage the power of multivirus-specific, donor-derived T-cells (mCTL), which are highly skilled at recognizing foreign invaders. The research team, made up of nine scientists and clinicians affiliated with Children’s National Health System, grew personalized T-cells from peripheral blood (PB) of adult donors who were seropositive for CMV and also coaxed T-cells to grow from naïve cord blood (CB). PB-derived cells have long memories of past battles; naïve CB-derived cells need additional training to acquire such skills. From 35 to 384 days after their stem cell or cord blood transplant, 13 patients were infused with PB mCTL and 12 patients were infused with CB mCTL. Within four weeks, patients experienced up to a 160-fold increase in virus-specific T-cells, which coincided with their response to therapy. Overall response rate was 81 percent.
Questions for Future Research Q: Could T-cells be personalized to attack other viruses that infect patients post-transplant, such as human parainfluenza virus and BK polyomavirus, providing the potential to target five viruses in a single infusion? Q: Could the proteins that are used to train T-cells to attack certain viruses also be used to create a personalized approach to tumor suppression?
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GImage_Training-T-Cells-Essential-Players_sm.jpg387600Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-05-26 20:53:052024-02-02 14:34:03Training t-cells, essential players in the immune system, to fight a trio of viruses
What’s Known Needle biopsies help to guide diagnosis and targeted therapies for diffuse intrinsic pontine gliomas (DIPGs), which make up 10 percent to 15 percent of all pediatric brain tumors but carry a median survival of 9 to 12 months. This dismal survival rate compares with a 70 percent chance of children surviving other central nervous system tumors five years post diagnosis. In DIPG, tumors appear in the pons, an area of the brain that houses cranial nerve nuclei. Surgical options are limited. Spatial and temporal tumor heterogeneity is a major obstacle to accurate diagnosis and successful targeted therapy.
What’s New
The team sought to better define DIPG heterogeneity. They analyzed 134 specimens from nine patients and found that H3K27M mutations were ubiquitous in all 41 samples with oncogenic content, and always were associated with at least one partner driver mutation: TP53, PPM1D, ACVR1 or PIK3R1. These H3K27M mutations are the initial oncogenic event in DIPG, writes the research team led by Children’s National Health System. “Driver” mutations, such as H3K27M, are essential to begin and sustain tumor formation. This main driver partnership is maintained throughout the course of the disease, in all cells across the tumor, and as tumors spread throughout the brain. Because homogeneity for main driver mutations persists for the duration of illness, efforts to cure DIPG should be directed at the oncohistone partnership, the authors write. Based on early tumor spread, efforts to cure DIPG should aim for early systemic tumor control, rather focused exclusively on the pons.
Questions for Future Research Q: If a larger sample size were analyzed, what would it reveal about the true heterogeneity/homogeneity status of DIPGs? Q: “Accessory” driver mutations are not absolutely essential but do help to further promote and accelerate tumor growth. What is their precise role?
Source: “Spatial and Temporal Homogeneity of Driver Mutations in Diffuse Intrinsic Pontine Glioma.” H. Nikbakht, E. Panditharatna, L.G. Mikael, R. Li, T. Gayden, M. Osmond, C.Y. Ho, M. Kambhampati, E.I. Hwang, D. Faury, A. Siu, S. Papillon-Cavanagh, D. Bechet, K.L. Ligon, B. Ellezam, W.J. Ingram, C. Stinson, A.S. Moore, K.E. Warren, J. Karamchandani, R.J. Packer, N. Jabado, J. Majewski, and J. Nazarian. Published by Nature Communications on April 6, 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/04/R@GSpatialDIPG_Image-1.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-04-06 17:36:362018-07-19 12:56:10Spatial and temporal homogeneity of driver mutations in diffuse intrinsic pontine glioma
What’s Known Neuron glia antigen-2 (NG2) is a protein expressed by many central nervous system cells during development and differentiation. NG2-expressing oligodendrocyte progenitor cells have been identified as the cells of origin in gliomas, tumors that arise from the brain’s gluey supportive tissue. What’s more, NG2 expression also has been associated with childhood diffuse intrinsic pontine glioma (DIPG) an aggressive tumor that accounts for 10 percent to 20 percent of pediatric central nervous system (CNS) tumors. Radiation can prolong survival by a few months, but children diagnosed with DIPG typically survive less than one year.
What’s New
Researchers are searching for appropriate targets and effective drugs that offer some chance of benefit. A team of Children’s National Health System researchers investigated whether NG2 – which plays a critical role in proliferation and development of new blood vessels and promotes tumor infiltration – could be a potential target for cancer treatment. Of the various options, antibody-mediated mechanisms of targeting NG2 are feasible, but the size of antibodies limits their ability to cross the blood-brain barrier. “Due to its role in maintaining a pluripotent pool of tumor cells, and its role in tumor migration and infiltration, NG2 provides multiple avenues for developing therapeutics,” the research team concludes. “Moreover, the large extracellular domain of NG2 provides an excellent antigen repertoire for immunotherapeutic interventions. As such, further research is warranted to define the role and expression regulation of NG2 in CNS cancers.”
Questions for Future Research
Q: Because healthy oligodendrocyte progenitor cells are important for the child’s developing brain, how could further characterization of NG2 isoforms help prevent drugs from damaging those beneficial cells?
Q: Could NG2-binding peptides cross the blood-brain barrier to deliver anti-cancer therapies precisely to tumor sites?
Source: “The Role of NG2 Proteoglycan in Glioma.” S. Yadavilli, E.I. Hwang, R. J. Packer, and J. Nazarian. Published by Translational Oncology on February 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GNG2DIPG-Image-e1496433328865.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-02-21 10:35:162018-05-02 16:57:25The role of NG2 proteoglycan in glioma
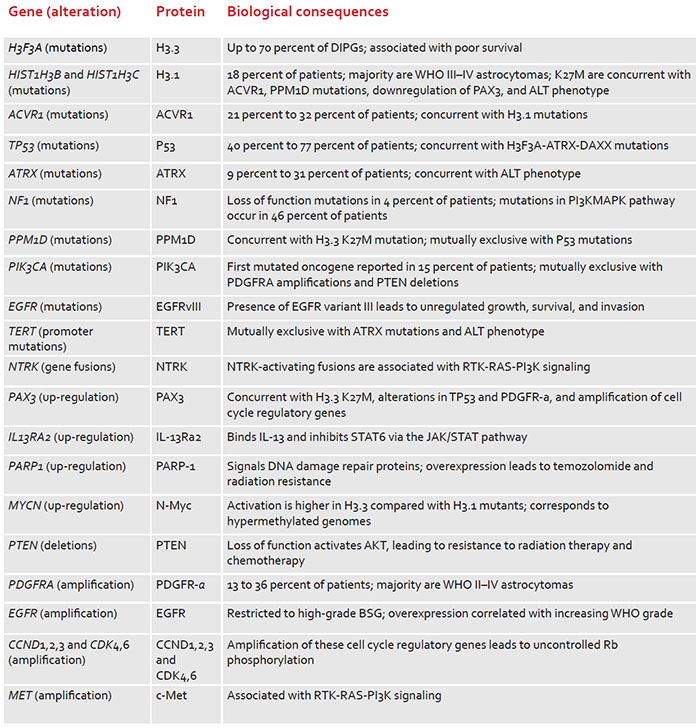
What’s Known Fewer than 150 U.S. children per year are diagnosed with diffuse intrinsic pontine glioma (DIPG), one of the most lethal pediatric central nervous system cancers. Despite an increasing number of experimental therapies tested via clinical trials, more than 95 percent of these children die within two years of diagnosis. Molecular studies have yielded additional insight about DIPG, including that mutations in histone-encoding genes are associated with 70 percent of cases. Understanding mutations that drive tumors and the genomic landscape can help to guide development of targeted therapies.
What’s New: Frequently found genetic alterations prevalent in DIPGs
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GGenomicDIPG_Image-e1496432847469.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2015-05-01 11:21:292018-05-02 16:57:25Clinicopathology of diffuse intrinsic pontine glioma and its redefined genomic and epigenomic landscape