Brain food for preemies

Babies born prematurely – before 37 weeks of pregnancy – often have a lot of catching up to do. Not just in size. Preterm infants typically lag behind their term peers in a variety of areas as they grow up, including motor development, behavior and school performance.
New research suggests one way to combat this problem. The study, led by Children’s researchers and presented during the Pediatric Academic Societies 2018 annual meeting, suggests that the volume of carbohydrates, proteins, lipids and calories consumed by very vulnerable premature infants significantly contributes to increased brain volume and white matter development, even though additional research is needed to determine specific nutritional approaches that best support these infants’ developing brains.
During the final weeks of pregnancy, the fetal brain undergoes an unprecedented growth spurt, dramatically increasing in volume as well as structural complexity as the fetus approaches full term.
One in 10 infants born in the U.S. in 2016 was born before 37 weeks of gestation, according to the Centers for Disease Control and Prevention. Within this group, very low birthweight preemies are at significant risk for growth failure and neurocognitive impairment. Nutritional support in the neonatal intensive care unit (NICU) helps to encourage optimal brain development among preterm infants. However, their brain growth rates still lag behind those seen in full-term newborns.
“Few studies have investigated the impact of early macronutrient and caloric intake on microstructural brain development in vulnerable preterm infants,” says Katherine Ottolini, lead author of the Children’s-led study. “Advanced quantitative magnetic resonance imaging (MRI) techniques may help to fill that data gap in order to better direct targeted interventions to newborns who are most in need.”
The research team at Children’s National Health System enrolled 69 infants who were born younger than 32 gestational weeks and weighed less than 1,500 grams. The infants’ mean birth weight was 970 grams and their mean gestational age at birth was 27.6 weeks.
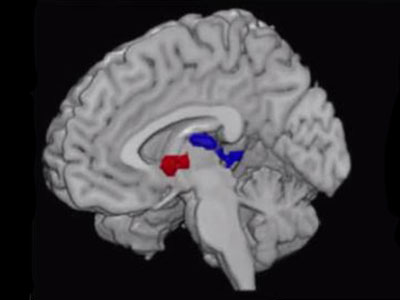
The newborns underwent MRI at their term-equivalent age, 40 weeks gestation. Parametric maps were generated for fractional anisotropy in regions of the cerebrum and cerebellum for diffusion tensor imaging analyses, which measures brain connectivity and white matter tract integrity. The research team also tracked nutritional data: Grams per kilogram of carbohydrates, proteins, lipids and overall caloric intake.
“We found a significantly negative association between fractional anisotropy and cumulative macronutrient/caloric intake,” says Catherine Limperopoulos, Ph.D., director of Children’s Developing Brain Research Laboratory and senior author of the research. “Curiously, we also find significantly negative association between macronutrient/caloric intake and regional brain volume in the cortical and deep gray matter, cerebellum and brainstem.”
Because the nutritional support does contribute to cerebral volumes and white matter microstructural development in very vulnerable newborns, Limperopoulos says the significant negative associations seen in this study may reflect the longer period of time these infants relied on nutritional support in the NICU.
In addition to Ottolini and Limperopoulos, study co-authors include Nickie Andescavage, M.D., Attending, Children’s Neonatal-Perinatal Medicine; and Kushal Kapse.