We are thrilled to announce that the Children’s National Spina Bifida Program has received official accreditation from the Spina Bifida Association (SBA).
We are thrilled to announce that the Children’s National Spina Bifida Program has received official accreditation from the Spina Bifida Association (SBA). This is a significant milestone that underscores our commitment to delivering the highest standards of clinical care and reflects the dedication of our entire team.
To gain a deeper understanding of what this accreditation means, we spoke with Christina Ho, M.D., Co-Director of the Children’s National Spina Bifida Program. Dr. Ho provided valuable insights into the significance of this achievement and its impact on the team and Spina Bifida Program.
Q: What does this accreditation mean to you and our program?
A: Achieving accreditation from the SBA signifies that our program is aligned with the best clinical practices and standards for spina bifida care. Over the past few years, we have made substantial strides, particularly in enhancing our adolescent transition program, implementing quality improvement projects and expanding community outreach.
This accreditation is a testament to the relentless efforts of our multidisciplinary team, each member of whom is committed to providing exceptional patient care. It acknowledges the hard work and dedication we invest daily to ensure the highest quality outcomes for our patients.
Q: How will this affect patient care?
A: As an accredited clinical care partner, we will have increased opportunities to collaborate on research projects with the SBA and other clinical care sites. This partnership will enable us to continue pushing the envelope on research-focused practices and cutting-edge care for all our patients. Our passion for excellence in patient care remains unwavering, and this accreditation will help us expand the breadth and quality of services and support we provide.
Q: What does this mean for patient families?
A: For families seeking comprehensive spina bifida care, this accreditation is a mark of assurance. By visiting the SBA website, families can now see that Children’s National Hospital is a recognized clinical care partner. This means they can access specialized, state-of-the-art spina bifida care right here in the Washington DC, Maryland and Virginia area. We are excited about the prospect of reaching more families in our region and welcoming those who seek the very best in spina bifida care.
A note on our team
Our program’s success is a direct result of the passion and dedication of our team members. Each individual brings an unwavering commitment to improving the lives of families living with spina bifida. It is this collective enthusiasm and expertise that truly distinguishes our program.
We look forward to continuing our mission of providing exceptional care and making a positive impact on the lives of those we serve. Thank you for your ongoing support and dedication.
Laura Tosi, M.D., was one of four inductees nominated into the Pediatric Orthopaedic Society of North America (POSNA) Hall of Fame, which honors members who have displayed dedication to teaching and mentoring, studying musculoskeletal conditions in children and caring for children with musculoskeletal conditions.
“I was particularly pleased to be recognized because my contributions have not been typical,” said Dr. Tosi. “I have never developed a new surgical technique or made a scientific breakthrough. Rather, I have come to recognize the importance of maintaining good bone health to support the quality of life of our patient population.”
Dr. Tosi began her career at Children’s National Hospital in 1984, focused on the care of children with disabilities such as spina bifida, cerebral palsy and arthrogryposis. Over the course of her tenure, she noted that children with these conditions were surviving at increasingly higher rates, but their quality of life was often derailed by disuse osteoporosis and pathologic fractures.
Her work on secondary fragility fracture prevention ultimately led her to develop the Children’s National Bone Health Program, which launched in 2003. She has since leveraged this program to expand interest in rare bone disease, thanks in part, to her collaborative work with the National Institutes of Health and Osteogenesis Imperfecta Foundation.
“We are all so proud of Dr. Tosi for this amazing recognition,” said Matthew Oetgen, M.D., M.B.A., chief of orthopaedic surgery and sports medicine at Children’s National. The POSNA Hall of Fame is a BIG DEAL! There really is no more powerful recognition than that of colleagues, and this award shows how much of an impact Dr. Tosi has had worldwide. She is a true leader in pediatric orthopaedic surgery and pediatric bone health, and this award is well deserved. Her dedication to Children’s National, the children of the region and us, her partners, has been unwavering, and we thank her for it.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/07/TOSI-POSNA-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2024-08-05 14:02:312024-08-05 14:02:31Laura Tosi, M.D., celebrated as a 2024 POSNA Hall of Fame inductee
Providers from the Department of Urology at Children’s National Hospital attended the Societies for Pediatric Urology Fall Congress in October 2022 and shared a series of abstracts.
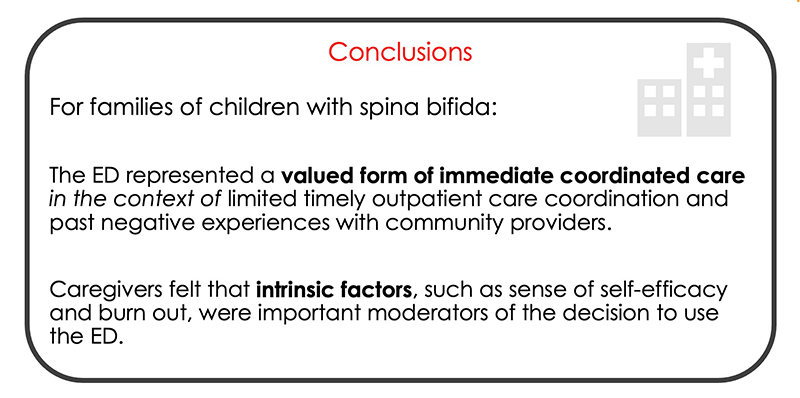
The abstracts look at unplanned healthcare use and missed visits among children with spina bifida, as well as factors associated with these outcomes. The team collected data from chart review and patient interviews to complete these projects. They considered clinical information, as well as demographic information and the childhood opportunity index, which is a composite measure that proxies social determinants of health, while accounting for how far a family lives from the emergency department.
Clinically, patients with more complex spina bifida (e.g., ventricular shunt or wheelchair use) were more likely to use the emergency department. Genitourinary and gastrointestinal problems were the most common reasons for emergency department use. Within the Spina Bifida Program at Children’s National, our providers are aggressively trying to reduce gastrointestinal complaints with a nurse practitioner dedicated to bowel management and working collaboratively with the Division of Colorectal and Pelvic Reconstruction.
A sobering finding from this research was that non-white patients with spina bifida at Children’s National were more likely to have had an emergency department visit between 2016-2020 after accounting for all other variables. This indicates a clear need for improving access, communication and quality of care for minority patients with spina bifida. We are increasingly developing our community partnerships with pediatricians and school nurses, and we are accessible by a direct phone line and email to allow for prompt support. We have also established clinics in Prince George’s County in Maryland which will bring the program closer to some minority communities.
The team also found that families of children with spina bifida scheduled for telemedicine visits were much more likely to miss a visit than a child without spina bifida or if the visit was in-person. This has led to changes in how we deploy telemedicine in this population, while still remaining nimble with the option of telemedicine or in-person visits. By screening the family’s ability and desire to use this modality, we hope to reduce missed visits overall.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2022/12/Societies-for-Pediatric-Urology-logo.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2022-12-19 09:27:402022-12-19 10:05:13Children’s National at the Societies for Pediatric Urology Fall Congress
The Spina Bifida Program at Children’s National Hospital, led by co-directors, Christina Ho, M.D., and Briony Varda, M.D., has seen impressive growth and there are plans to continue expanding the program. Drs. Ho and Varda share insights on the multidisciplinary care being provided, along with their plans for the future of the program.
Q: How would you describe the growth of the program?
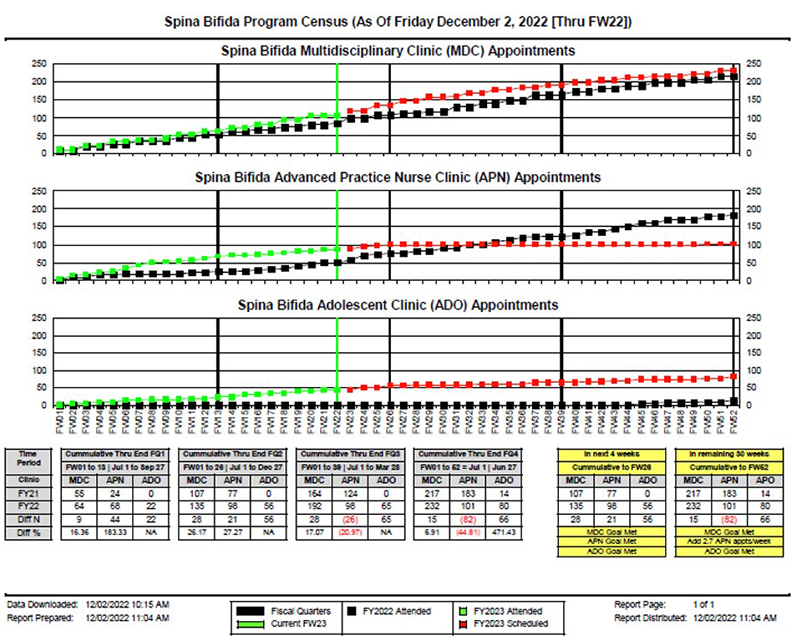
A: The growth of the Spina Bifida Program has been remarkable! The graph below really shows it all (more than a 25% increase in patient visits in the past year). We currently hold multidisciplinary programs including providers from neurosurgery (Robert Keating, M.D.), orthopaedic surgery (Matthew Oetgen, M.D.), physical medicine and rehabilitation (Mi Ran Shin, M.D.), urology (Briony Varda, M.D. and Christina Ho, M.D.), and expanded to include bowel management (Celicia Little, N.P.), gynecology (Allison Mayhew, M.D.) for our adolescent patients, as well as a dedicated nurse, Nicole Allentuck, R.N., and program associate, Christine Scott.
We are extremely proud of how the program has grown, particularly through the past two years, with the advent of our adolescent clinic and having a dedicated supportive team that ensures we have significant re-engagement of patients who had previously been lost to care. We are also working with the Prenatal Pediatrics Institute at Children’s National to enhance our prenatal care for patients diagnosed with spina bifida.
Q: What advancements is the spina bifida program making that benefit patients?
A: We have developed a transition clinic for our adolescent spina bifida patients to help address goals of care, independence with care and readiness for transition to adult providers. Our program coordinator, Celicia Little, N.P., also oversees our bowel management program to provide specialized bowel management care for our patients. We have been working on educational information specific to different areas within spina bifida, including how to catheterize, common medications, bowel management and anticipatory guidance. This helps to provide longevity for our patients as well. We are evaluating ways to decrease visits to the emergency department and ensure appropriate antibiotic usage with proper diagnoses of urinary infections in patients who perform CIC. To further our goal of providing longitudinal care within our program, we have engaged gynecology colleagues to see patients within our adolescent clinic and begin promoting independence through perpetuated discussions (e.g., are they able to schedule their own physician appointments or grocery shop for themselves?) in preparation for adult transitional care. Additionally, we readily offer telehealth visits for convenience and in hopes of easing access to care.
Q:Looking ahead, what’s next for the Spina Bifida Program? How will we continue to measure success?
A: We are excited to continue expanding our Spina Bifida Program. We currently care for more than 500 patients within the Washington, D.C., Maryland and Virginia areas. We want to continue to include patient narratives through our research initiatives to inform quality of care, including decreasing E.D. utilization and needless antibiotic use. We also want to expand our adolescent program to include sexual healthcare as they transition to adult care with our adult collaborators within MedStar and GWU. We would like to provide more comprehensive care, improve access to care, and ensure patients and families have utilization of the armamentaria of medical resources available at Children’s National.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2022/12/growth-of-spina-bifida-program-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2022-12-19 09:07:172022-12-19 09:08:58A look at the Children’s National Spina Bifida Program
Briony Varda, M.D., M.P.H., is fellowship trained in pediatric genitourinary reconstructive surgery and her subspecialty interests include the care of patients with spina bifida and the neurogenic bladder, cloacal anomalies, hydronephrosis, vesicoureteral reflux and posterior urethral valves, among others.
Children’s National Hospital recognizes many urologic disorders and illnesses that are unique to children. As such, we pride ourselves in working with top urology experts, including Briony Varda, M.D., M.P.H., pediatric urologist, who recently joined the Urology Division at Children’s National.
Dr. Varda is fellowship trained in pediatric genitourinary reconstructive surgery and her subspecialty interests include the care of patients with spina bifida and the neurogenic bladder, cloacal anomalies, hydronephrosis, vesicoureteral reflux and posterior urethral valves, among others.
Here, Dr. Varda tells us more about her work and what it means for the future of pediatric urology patients at Children’s National.
Q: Why did you decide to work in this field?
I have always thoroughly enjoyed working with children. They keep you on your toes, tell it straight, make you laugh and demonstrate unique resilience. At the same time, surgery allows me to work with my hands, while being creative and helping others. Finally, I had great mentors within pediatric urology who strongly influenced me in a positive way.
In sum, the kids, the surgery and the people led me here.
Q: What is the importance of urology care?
We have three goals in pediatric urology: protect the kidneys and bladder, prevent infection and help our patients stay dry.
Although it’s usually clear when kids have urinary tract infections or trouble with urinary accidents, it’s not always visible when there is a problem with the kidney or bladder. Urologic care is therefore important because it prevents long-term damage that might otherwise go unnoticed until it is too late. This is particularly true for patients with abnormal functioning of the bladder related to a neurologic cause, such as spina bifida or a tethered spinal cord.
Q: How has the program expanded and what are some of the most valuable changes you hope to see in the next couple of years?
Our Spina Bifida Program currently includes physicians from physical medicine and rehabilitation (PMNR), orthopedics, neurosurgery and urology. Our newest additions include a full-time nurse practitioner who facilitates care coordination and has a clinical expertise in bowel management, two new urologists (myself and Christina Ho, M.D.), and Mi Ran Shin, M.D., who is our new PMNR physician.
We are also collaborating closely with the new Pediatric Colorectal & Pelvic Reconstruction Division for patients who need advanced bowel management. These additions will go a long way to helping improve the day-to-day living of our patients and help improve their long-term medical outcomes.
In the coming year, we are anticipating welcoming another full-time nurse to our program, offering more patient-facing resources including a webpage focused on urodynamics and an array of new patient education materials. We are also hoping to establish a regional transitional care network for our adolescent and young-adult patients.
Q: The Colorectal Program at Children’s National includes three urologists. How does this collaboration allow for the care of more complex cases at this hospital?
We are fortunate to be part of the Colorectal Program here at Children’s National Hospital. We provide subspecialty expertise for patients born with anorectal malformations, including cloacal anomalies and cloacal exstrophy. Although historically considered a general surgery problem, patients with anorectal malformations have a high rate of concomitant conditions affecting their genitourinary anatomy and function. By coordinating clinical care and surgery within a multidisciplinary team, we provide comprehensive care for even the most complex patients – nothing goes unnoticed and each subspecialist provides a unique perspective on management as it relates to their field. Along with ourselves and the colorectal surgeons, we regularly collaborate with gynecology, gastroenterology, interventional radiology and anesthesia.
Q: What is some of the research you’re working on now that you’re looking forward to the most?
We are currently designing a set of research projects aimed at investigating low-value healthcare utilization (for example, emergency room use and inappropriate testing) among patients with spina bifida. I plan to investigate institutional patterns and then expand out to the Washington, D.C., Maryland, Virginia area and the national setting. By identifying patterns in low-value healthcare utilization and their associated factors, we can ideally improve care delivery for this special healthcare needs population.
We are also working on institutional protocols to enact recently published guidelines by the Spina Bifida Association and the CDC so that we can eventually contribute our own data to national registries. This will pave the way for increasingly rigorous spina bifida research in the future.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/12/Briony-Varda.png400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-12-22 10:00:332020-12-22 10:01:55Q&A with urologist Briony Varda
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/03/child-writing-question-marks-on-chalkboard-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-03-13 16:07:512020-03-16 13:44:11Test your knowledge of pediatric colorectal and pelvic reconstructive surgery!
“With the broad range of expertise at Children’s National, including the nation’s best NICU, I’m confident that colorectal patients will get better, integrated care faster and more effectively here than anywhere else in the world,” says Marc Levitt, M.D.
World-renowned surgeon opens first program for care and treatment of colorectal conditions in the mid-Atlantic.
A new, highly-specialized surgical program at Children’s National Hospital is expected to draw patients from around the world. The colorectal surgery program is the first in the mid-Atlantic region to fully integrate surgery, urology, gynecology and gastroenterology into one cohesive program for children. The program is led by Marc Levitt, M.D., an internationally recognized expert in the surgical care and treatment of pediatric colorectal disorders who has performed over 10,000 surgeries to address a wide spectrum of problems involving the colon and rectum – more than any other full time practicing pediatric surgeon in the world.
“In the 25 years that I’ve been passionate about helping children with colorectal and pelvic conditions, I’ve learned that collaborative and integrated programs are the best way to care for them,” says Dr. Levitt. “With the broad range of expertise at Children’s National, including the nation’s best NICU, I’m confident that colorectal patients will get better, integrated care faster and more effectively here than anywhere else in the world.”
The program provides diagnosis and treatment for every type of colorectal disorder occurring in infants, children and adolescents, from the most common to the most complex. Every necessary specialty is integrated into the program in one convenient location to provide seamless care for all colon and rectum conditions, with particular expertise in:
Anorectal malformations
Cloacal malformations
Chronic constipation and fecal incontinence
Fecal and urinary incontinence related to spinal conditions such as spina bifida
Hirschsprung disease
Motility disorders
“Every child receives a customized treatment plan to address his or her unique needs,” Dr. Levitt says about the program. “Additionally, our surgeons often combine complex procedures across specialties to reduce the number of surgeries a child requires. It isn’t unusual for us to include urology, gynecology, and gastroenterology teams in the operating room alongside the colorectal surgeons so multiple issues can be addressed in a single procedure – we know that when possible, fewer surgeries is always better for the child.”
Dr. Levitt has cared for children from 50 states and 76 countries. He is the founder of Colorectal Team Overseas (CTO), a group of international providers who travel to the developing world to provide care for patients and teaching of their physicians and nurses. He co-founded the Pediatric Colorectal and Pelvic Learning Consortium (PCPLC), an organization of collaborating colorectal centers across the globe.
“We’re absolutely thrilled to welcome Marc Levitt and launch the comprehensive colorectal program under his expert leadership,” adds Anthony Sandler, M.D., surgeon-in-chief and vice president of the Joseph E. Robert, Jr., Center for Surgical Care at Children’s National. “There are few in the world who can provide the expertise and leadership in colorectal diagnoses and treatment that Marc brings with him to Children’s. Many children and families from the region and from around the world will benefit from his expertise and from the program in general.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/01/Marc-Levitt.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-01-29 12:53:262020-04-30 16:40:43Premier pediatric colorectal program opens doors at Children’s National
Research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that genetic mutations that cause cleft lip and palate also may contribute to neural tube defects, such as spina bifida.
Oral clefts are some of the most common birth defects worldwide, affecting about one in every 700 births. In the U.S., more than 4,000 babies are born each year with cleft lip, with or without cleft palate.
This defect isn’t simply a cosmetic manner: Oral clefts can severely affect feeding, speech and hearing, and they cause about 3,300 deaths annually worldwide.
To better understand these conditions, researchers have isolated a number of genetic mutations that appear to play contributing roles. These include those in a gene known as Interferon Regulatory Factor 6. New research by an international team that includes Children’s National faculty, published online Jan. 25, 2019 in Human Molecular Genetics, suggests that these mutations also may contribute to neural tube defects such as spina bifida.
In the first weeks of fetal development, the neural plate curves, creating a neural tube that, once fused shut, becomes the fetal brain and fetal spinal cord. Neural tube defects, which can range from mild to severe, are characterized by incomplete development of the brain, spinal cord or meninges. These defects can potentially result in paralysis or even fetal or neonatal demise. According to the National Institutes of Health, spina bifida, which affects the spinal cord, is the most common neural tube defect in the U.S., affecting up to 2,000 infants each year.
“Despite its high frequency, spina bifida remains among the least understood structural birth defects,” says Brian C. Schutte, an associate professor of Microbiology and Molecular Genetics, Pediatrics and Human Development at Michigan State University and the study’s senior author. “There is strong evidence that genetic factors are a leading cause of such structural birth defects, but in most cases, the cause is unknown. Our team’s study is the first published research to demonstrate that DNA variants in the gene IRF6 can cause spina bifida,” Schutte says.
What’s more, the research team identified a mechanism to explain how altering IRF6 leads to neural tube defects. This mechanism links IRF6 function to two other genes – known as transcription Factor AP2A (TFAP2A) and Grainyhead Like 3 (GRHL3) – that are also known to be required for the development of the neural tube, lip and palate.
“We’re all on the hunt for the reasons when, how and why birth defects happen,” adds Youssef A. Kousa, MS, D.O., Ph.D., a clinical fellow in the Division of Child Neurology at Children’s National Health System and the study’s lead author. “Our main goal is prevention. This paper is a significant development because our team has identified a group of genes that can potentially contribute to very common types of birth defects: craniofacial as well as neural tube defects.”
The scientific odyssey is a wonderful example of serendipity. Kousa, then working in Schutte’s lab, was studying the effects of a new mutant experimental model strain on development of the palate. But one day, he walked into Schutte’s office holding a deformed preclinical embryo and said: “Brian, look at this!”
“Weird things happen in biology,” Schutte replied and counseled him to return if it happened again. Less than two weeks later, Kousa was back with several more of the deformed preclinical embryos, saying: “OK, Brian. It happened again.”
Within hours Kousa had unearthed recently published research that included an image of a similarly affected preclinical embryo. The pair then sketched out possible intersecting genetic pathways, as they brainstormed the myriad ways to end up with that specific phenotype. Initially, they tested their hypotheses in experimental models and eventually corroborated findings through human genetic studies.
The human studies could only be performed by collaborations. Schutte shared their initial observations with human genetics researchers scattered across the country. Those labs then generously agreed to test whether DNA variants in IRF6 were associated with neural tube defects in samples from patients that they had collected over decades of research.
The team found that Tfap2a, Irf6 and Grhl3 are components of a gene regulatory network required for neurulation, a folding process that results in the neural tube bending and then fusing to become the basis of the embryo’s nervous system, from brain to spinal cord.
“Since this network is also required for formation of the lip, palate, limbs and epidermis, which develop at different times and places during embryogenesis, we suggest that the Tfap2a–Irf6–Grhl3 network is a fundamental pathway for multiple morphogenetic processes,” the researchers write.
Interferon Regulatory Factor 6 functions best when there is neither too much expression nor too little. Overexpression of Irf6 suppresses Transcription Factor Activation Protein 2A and Grainyhead Like 3, causing exencephaly, a neural tube defect characterized by the brain being located outside of the skull. Counterintuitively, experimental models that had too little Irf6 also ended up with reduced levels of Tfap2a and Grhl3 that led to a structural birth defect, but at the opposite end of the neural tube.
To test whether the experimental model findings held true in humans, they sequenced samples from people who had spina bifida and anencephaly – the rare birth defect that Kousa spotted in the experimental models – and found IRF6 function was conserved in people. Because of the genetic complexity of these birth defects, and the challenges inherent in collecting samples from cases of severe birth defects, many research teams were invited to participate in the study.
As testament to their collegiality, researchers from Stanford University, University of Texas at Austin, University of Iowa, University of Texas at Houston and Duke University agreed to share precious samples from the California Birth Defects Monitoring Program, from the Hereditary Basis of Neural Tube Defects study and from their own institutional sample collections.
“As we get better at personalized medicine, we could use this information to one day help to counsel families about their own risk and protective factors,” Kousa adds. “If we can identify the genetic pathway, we might also be able to modify it to prevent a birth defect. For example, prenatal supplementation with folic acid has led to a decrease in babies born with neural tube defects, but not all neural tube defects are sensitive to folic acid. This knowledge will help us develop individual-based interventions.”
Financial support for the research covered in this post was provided by the National Institutes of Health under grants DE13513, F31DE022696, DE025060, P01HD067244 and GM072859; startup funding from Michigan State University and the UT-Health School of Dentistry in Houston; and the Centers for Disease Control and Prevention under award number 5U01DD001033.
In addition to Kousa and Schutte, study co-authors include Huiping Zhu, Yunping Lei and Richard H. Finnell, University of Texas at Austin; Walid D. Fakhouri, University of Texas Health Science Center at Houston; Akira Kinoshita, Nagasaki University; Raeuf R. Roushangar, Nicole K. Patel, Tamer Mansour, Arianna L. Smith, and Dhruv B. Sharma, Michigan State University; A.J. Agopian and Laura E. Mitchell, University of Texas School of Public Health; Wei Yang and Gary M. Shaw, Stanford University School of Medicine; Elizabeth J. Leslie, Emory University; Xiao Li, Tamara D. Busch, Alexander G. Bassuk and Brad A. Amendt, University of Iowa; Edward B. Li and Eric C. Liao, Massachusetts General Hospital; Trevor J. Williams, University of Colorado Denver at Anschutz Medical Campus; Yang Chai, University of Southern California; and Simon Gregory and Allison Ashley-Koch, Duke University Medical Center.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/01/little-girl-with-spina-bifida.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-01-25 12:58:112024-12-30 12:46:57Oral clefts may stem from a shared genetic cause as neural tube defects
Decades ago, researchers thought that the native bacteria scattered throughout the human body—such as in the gut, the oral cavity and the skin—served little useful purpose. This microbiota, whose numbers at least match those of the cells in the body they live on and in, were considered mostly harmless hitchhikers.
More recently, research has revealed that these natural flora play key roles in maintaining and promoting health. In addition, studies have shown that understanding what a “typical” microbiome looks like and how it might change over time can provide an early warning system for some health conditions, including cancer.
Now, a small, multi-institutional study conducted in experimental models suggests that as bladder cancer progresses, it appears to be associated with a unique bacterial fingerprint within the bladder—a place thought to be bacteria-free except in the case of infection until just a few years ago. The finding opens the possibility of a new way to spot the disease earlier.
Bladder cancer is the fourth-most common malignancy among U.S. men but, despite its prevalence, mortality rates have remained stubbornly high. Patients often are diagnosed late, after bladder cancer has advanced. And, it remains difficult to discern which patients with non-invasive bladder cancer will go on to develop muscle-invasive disease.
New technological advances have led to identification of a diverse community of bacteria within the bladder, the urinary microbiome. Leveraging these tools, a research team that includes Children’s National Health System investigators studied whether an experimental model’s urinary bacterial community changed as bladder cancer progressed, evolving from a microbiome into a urinary “oncobiome.”
To test the hypothesis, the research team led by Michael H. Hsieh, M.D., Ph.D., a Children’s urologist, exposed an experimental model of bladder cancer to a bladder-specific cancer-causing agent, n-butyl-n-(4-hydroxybutyl) nitrosamine (BBN). Bladder cancers induced by BBN closely resemble human cancers in tissue structure at the microscopic level and by gene expression analyses. Ten of the preclinical models received a .05 percent concentration of BBN in their drinking water over five months and were housed together. Ten other experimental models received regular tap water and shared a separate, adjacent cage.
Researchers collected urine samples ranging from 10 to 100 microliters at the beginning of the longitudinal study, one week after it began, then once monthly. They isolated microbial DNA from the urine and quantified it to determine how much DNA was microbial. All of the bladders from experimental models exposed to BBN and two bladders from the control group were analyzed by a pathologist trained in bladder biology.
According to the study published online July 5, 2018, by the biology preprint server Biorxiv, they found a range of pathologies:
Five of the experimental models that received BBN did not develop cancer but had histology consistent with inflammation. Three had precancer on histology: urothelial dysplasia, hyperplasia or carcinoma in situ. Two developed cancer: invasive urothelial carcinomas, one of which had features of a squamous cell carcinoma.
The experimental model that developed invasive carcinoma had markedly different urinary bacteria at baseline, with Rubellimicrobium, a gram negative organism found in soil that has not been associated with disease previously, Escherichia and Kaistobacter, also found in soil, as the most prominent bacteria. By contrast, in the other experimental models the most common urinary bacteria were Escherichia, Prevotella, Veillonella, Streptococcus, Staphylococcus and Neisseria.
By month four, the majority of experimental models exposed to BBN had significantly higher proportion of Gardnerella and Bifidobacterium compared with their control group counterparts.
“Closely analyzing the urinary bacterial community among experimental models exposed to BBN, we saw distinct differences in microbial profiles by month four that were not present in earlier months,” Dr. Hsieh says. “While Gardnerella is associated with the development of cancer, Bifidobacterium has been shown to exert antitumor immunity, and its increasing abundance points to the need for additional research to understand its precise role in oncogenesis.”
Dr. Hsieh adds that although the study is small, its findings are of significance to children who are prone to developing urinary tract infections (UTIs), including children with spina bifida, due to the association between UTIs and bladder cancer. “This work is important because it not only suggests that the urinary microbiome could be used to diagnose bladder cancer, but that it could also perhaps predict cancer outcomes. If the urinary microbiome contributes to bladder carcinogenesis, it may be possible to favorably change the microbiome through antibiotics and/or probiotics in order to treat bladder cancer.”
In addition to Dr. Hsieh, co-authors include Catherine S. Forster, M.D., M.S., and Crystal Stroud, of Children’s National; James J. Cody, Nirad Banskota, Yi-Ju Hsieh and Olivia Lamanna, of the Biomedical Research Institute; Dannah Farah and Ljubica Caldovic, of The George Washington University; and Olfat Hammam, of Theodor Bilharz Research Institute.
Research reported in this news release was supported by the National Institutes of Health under award number R01 DK113504 and the Margaret A. Stirewalt Endowment.
As part of Research and Education Week 2018, two Presidential awardees were recognized for their research contributions, Catherine “Katie” Forster, M.D., M.S., and Nathan Anthony Smith, Ph.D.
Catherine “Katie” Forster, M.D., M.S., and Nathan Anthony Smith, Ph.D., received the President’s Award for Innovation in Research honoring their respective research efforts to explore an understudied part of the microbiome and to shed light on an underappreciated player in nerve cell communication.
Drs. Forster and Smith received their awards April 19, 2018, the penultimate day of Research and Education Week 2018, an annual celebration of the excellence in research, education, innovation and scholarship that takes place at Children’s National Health System. This year marks the fifth time the President’s Award honor has been bestowed to Children’s faculty.
Dr. Forster’s work focuses on preventing pediatric urinary tract infections (UTIs). Frequently, children diagnosed with illnesses like spina bifida have difficulty urinating on their own, and they often develop UTIs. These repeated infections are frequently treated with antibiotics which, in turn, can lead to the child developing antibiotic-resistant organisms.
“The majority of the time if you culture these children, you’ll grow something. In a healthy child, that culture would indicate a UTI,” Dr. Forster says. “Children with neurogenic bladder, however, may test positive for bacteria that simply look suspect but are not causing infection. Ultimately, we’re looking for better ways to diagnose UTI at the point of care to better personalize antibiotic treatment and limit prescriptions for children who do not truly need them.”
Powered by new sequencing techniques, a research group that includes Dr. Forster discovered that the human bladder hosts a significant microbiome, a diverse bacterial community unique to the bladder. Dr. Forster’s research will continue to characterize that microbiome to determine how that bacterial community evolves over time and whether those changes are predictable enough to intervene and prevent UTIs.
“Which genes are upregulated in Escherichia coli and the epithelium, and which genes are upregulated by both in response to each other? That can help us understand whether genes being upregulated are pathogenic,” she adds. “It’s a novel and exciting research area with significant public health implications.”
Smith’s work focuses on the role of astrocytes, specialized star-shaped glial cells, in modulating synaptic plasticity via norepinephrine. Conventional thinking describes astrocytes as support cells but, according to Smith, astrocytes are turning out to be more instrumental.
Norepinephrine, a neurotransmitter that plays an essential role in attention and focus, is released by a process known as volume transmission, which is a widespread release of a neurotransmitter at once, says Smith, a principal investigator in Children’s Center for Neuroscience Research. Astrocytes, which outnumber neurons in the brain, are strategically and anatomically located to receive this diffuse input and translate it into action to modulate neural networks.
“We hypothesize that astrocytes are integral, functional partners with norepinephrine in modulating cortical networks,” Smith adds. “Since astrocytes and norepinephrine have been implicated in many central nervous system functions, including learning and attention, it is critical to define mechanistically how astrocytes and norepinephrine work together to influence neural networks. This knowledge also will be important for the development of novel therapeutics to treat diseases such as attention deficit hyperactivity disorder and epilepsy.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/04/Presidents-Award-for-Innovation-in-Research_2018.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-04-19 16:08:212024-11-27 09:34:25President’s Award highlights innovative work by early-career researchers
Researchers have known for decades that folate, a vitamin enriched in dark, leafy vegetables; fruit; nuts; and other food sources, plays a key role in preventing neural tube defects.
Every year, about 3,000 pregnancies in the U.S. are affected by neural tube defects (NTDs) – birth defects of the brain, spine and spinal cord. These include anencephaly, in which a major part of the brain, skull and scalp is missing; and spina bifida, in which the backbone and membranes around the spinal cord don’t close properly during fetal development. These structural birth defects can have devastating effects: In the best cases, they might lead to mild but lifelong disability; in the worst cases, babies don’t survive.
Researchers have known for decades that folate, a vitamin enriched in dark, leafy vegetables; fruit; nuts; and other food sources, plays a key role in preventing NTDs. To help get more folate into pregnant women’s diets, wheat flour in the U.S. and many other countries is often fortified with folic acid, a synthetic version of this vitamin, as part of an intervention credited with significantly reducing the incidence of NTDs.
But folic acid supplementation isn’t enough, says Irene E. Zohn, Ph.D., a principal investigator at the Center for Neuroscience Research at Children’s National Health System who studies how genes and the environment interact during development. A significant number of NTDs still occur, suggesting that other approaches – potentially, other nutrients in the maternal diet – might provide further protection.
That’s why Zohn and colleagues decided to investigate iron. Iron deficiency is one of the most common micronutrient deficiencies in women of childbearing age, Zohn explains. Additionally, iron and folate deficiencies often overlap and signal overall poor maternal diets.
The idea that iron deficiency might play a role in NTDs came from studies by Zohn and colleagues of the flatiron mutant line of experimental models. This experimental model line has a mutation in a gene that transports iron across cell membranes, including the cells that supply embryos with this critical micronutrient.
To determine if NTDs develop in these mutant experimental models because of reduced iron transport, the researchers devised a simple experiment: They took female adult experimental models with the mutation and separated them into four groups. For several weeks, one group ate a diet that was high in folic acid. Another group ate a diet high in iron. The third group ate a diet high in both folic acid and iron. The fourth group ate standard chow. All of these experimental models then became pregnant with embryos that harbored the flatiron mutation, and the researchers assessed the offspring for the presence of NTDs.
“We were hoping that iron supplements would be the next folic acid, but it did not turn out that way,” says Irene E. Zohn, Ph.D. “Even though our results demonstrate that iron is important for proper neural tube development, giving extra iron definitely has its downsides.”
As they reported in Birth Defects Research, the dietary interventions successfully increased iron stores: Experimental model mothers whose diets were supplemented with iron, folic acid or both had increased concentrations of these micronutrients in their blood.
The dietary interventions also affected their offspring. While about 80 percent of flatiron mutant embryos fed a standard diet during pregnancy had NTDs, feeding a diet high in iron prevented NTDs in half of the offspring. This lower rate was similar in the offspring of mothers fed a diet high in both folic acid and iron, but not for those whose mothers ate just a diet high in folic acid. Those embryos had NTD rates as high as those who ate just the standard chow, suggesting that low iron was the cause of the high rates, not low folic acid.
Together, Zohn says, these experiments show that iron plays an important role in the development of the neural tube and that deficits in iron might cause some cases of NTDs. However, she notes, reducing NTDs isn’t nearly as simple as supplementing pregnant women’s diets with iron. In the same study, the researchers found that when they gave normal experimental models that didn’t have the flatiron mutation concentrated iron supplements – amounts akin to what doctors might prescribe for human patients with very severe iron-deficiency anemia – folate stores dropped.
That’s because these two micronutrients interact in the body with similar sites for absorption and storage in the intestines and liver, Zohn explains. At either the intestines or liver or at both locations, an iron overload might interfere with the body’s ability to absorb or use folate.
At this point, she says, giving high doses of iron routinely during pregnancy doesn’t look like a feasible way to prevent NTDs.
“We were hoping that iron supplements would be the next folic acid, but it did not turn out that way,” Zohn says. “Even though our results demonstrate that iron is important for proper neural tube development, giving extra iron definitely has its downsides.”
Zohn’s team plans to continue to investigate the role of iron, as well as the role of other micronutrients that might influence neural tube development.
Zohn’s coauthors include Bethany A. Stokes, The George Washington University, and Julia A. Sabatino, Children’s National.
Research reported in this story was supported by a grant from the Board of Visitors, Eunice Kennedy Shriver National Institute of Child Health & Human Development under award number R21-HD076202, the National Center for Research Resources under award number UL1RR031988, Children’s Research Institute and the National Institutes of Health under grant P30HD040677.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/03/foods-rich-in-folate.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-03-01 12:57:352024-05-29 09:01:44An ironclad way to prevent neural tube defects? Not yet
A hot topic at national urology meetings is how to transition patients with pediatric-onset urologic conditions as they grow into adults. Michael Hsieh, MD, PhD, is leading the way in the U.S. by serving as a bridge for patients at the first dedicated transitional urology program in the mid-Atlantic region. The Clinic for Adolescent and Adult PedIatric OnseT UroLogy (CAPITUL) is a joint venture between Children’s National and George Washington University Hospital that started two years ago.
What’s most unique about the clinic is that Dr. Hsieh has a foot in both the pediatric world of urology and one in the adult world, with clinical privileges at both institutions. He sees the full span of pediatric urology patients, including expectant moms with fetuses that have suspected urologic anomalies to adults who may have congenital conditions that require follow-up. However, he sees more teenagers and young adults than his urology colleagues both at hospitals.
The clinic’s patients have included a 19-year-old man with multiple urethrocutaneous fistulas after failed hypospadias repairs, a 25-year-old woman with cloacal exstrophy and continent urinary diversion with a urinary tract infection and stones, and a 25-year-old man with spina bifida with incontinence urethral erosion from an indwelling catheter.
A number of significant urological conditions until recently led to premature death because of medical complications, Dr. Hsieh says. Today, 90 percent of spina bifida patients live past the age of 30. “There’s a synchronized wave of patients who are all now young adults with spina bifida, and they are facing issues of reproduction and sexuality,” Dr. Hsieh says. “These are issues that pediatric urologists generally speaking are not comfortable in managing. It makes sense: It’s been many, many years since they did that type of urology.”
The program is specifically following this transitional group on conditions that are long term and that may affect fertility, such as cancer and varicoceles.
One in five teenage boys have varicoceles, or varicose veins on the scrotum. “The relationship between having varicocele as a teenager and infertility as an adult is not clear, so we felt it important to include this diagnosis in the transitional program so we can follow these patients long term and monitor their testicular growth,” Dr. Hsieh says.
Proof that the program’s working
Dr. Hsieh tracks the messages from colleagues referring patients from one institution to the other. “Unfortunately, some patients and families—for a range of issues—fall through the cracks, so it is really important to have that direct link. If we didn’t have the program set up as it is, there would be fewer successful transitions between institutions,” he says.
Another way Dr. Hsieh knows the program is working is because of the uptick in adolescent and young adult patients in his practices at Children’s and at GW.
Dr. Hsieh says the optimal time to begin transition is at age 12, when the team makes the patient and family aware of the transition policy. From ages 14-16, it’s time to initiate the health care transition plan and begin discussing the adult model of care. By age 18, Dr. Hsieh recommends the transition to adult care, and by ages 23-26, patients are integrated into adult care.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/10/bridge-e1495654508580.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-10-05 11:38:002018-09-24 14:02:38Transitional urology bridges care for those with pediatric-onset conditions