A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.
Preliminary results from a phase II clinical trial at Children’s National Hospital showed that a new drug, vosoritide, can increase growth in children with certain growth disorders. This was the first clinical trial in the world testing vosoritide in children with certain genetic causes of short stature. (2 min. read)
Children’s National Hospital successfully performed the first ever high-intensity focused ultrasound (HIFU) non-invasive procedure on a pediatric patient with neurofibromatosis. This was the youngest patient to undergo HIFU treatment in the world. (3 min. read)
Using a single injection of a low dose gene therapy vector, researchers at Children’s National restored the ability of injured muscle fibers to repair in a way that reduced muscle degeneration and enhanced the functioning of the diseased muscle. (3 min. read)
A world-class team of researchers co-led by Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research at Children’s National, was selected to receive a $25m Cancer Grand Challenges award to tackle solid tumors in children. (4 min. read)
Children’s National opened a new telehealth command center that uses cutting-edge technology to keep continuous watch over children with critical heart disease. The center offers improved collaborative communication to better help predict and prevent major events, like cardiac arrest. (2 min. read)
Children’s National named Monika Goyal, M.D., M.S.C.E., associate chief of Emergency Medicine, as the first endowed chair of Women in Science and Health (WISH) for her outstanding contributions in biomedical research. (2 min. read)
A team at Children’s National performed the first treatment with sonodynamic therapy utilizing low intensity focused ultrasound (LIFU) and 5-aminolevulinic acid (5-ALA) medication on a pediatric patient. The treatment was done noninvasively through an intact skull. (3 min. read)
In an editorial, Roberta L. DeBiasi, M.D., M.S., provided a comprehensive review of what is known about the harmful effects of SARS-CoV-2 infection in pregnant women themselves, the effects on their newborns, the negative impact on the placenta and what still is unknown amid the rapidly evolving field. (2 min. read)
Doctors at Children’s National used a staged, hybrid cardiac surgical strategy to care for a patient who was born with hypoplastic left heart syndrome (HLHS) at 28-weeks-old. Hybrid heart procedures blend traditional surgery and a minimally invasive interventional, or catheter-based, procedure. (4 min. read)
In a review article in Seminars in Pediatric Surgery, Marc Levitt, M.D., chief of the Division of Colorectal and Pelvic Reconstruction at Children’s National, discussed the history of pediatric colorectal and pelvic reconstructive surgery and described the key advances that have improved patients’ lives. (11 min. read)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2023/01/2022-innovation-Feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2023-01-06 13:15:252023-01-09 13:41:05The best of 2022 from Innovation District
The ultrasound waves activate the drug selectively within the tumor, causing tumor cell death. Credit: Image provided by Insightec.
A multidisciplinary brain tumor team at Children’s National Hospital successfully performed the first treatment with sonodynamic therapy utilizing low intensity focused ultrasound (LIFU) and 5-aminolevulinic acid (5-ALA) medication on a pediatric patient. The treatment, performed on a 5-year-old child diagnosed with a diffuse intrinsic pontine glioma (DIPG), was done noninvasively through an intact skull. The child was discharged from the hospital one day later.
What happened?
Shortly after announcing the use of LIFU, the brain tumor team at Children’s National treated the patient as part of a cutting-edge trial using LIFU combined with a novel medication.
The ultrasound waves – which are given while the child is asleep through an intact skull and does not require an invasive neurosurgical procedure – activate the drug selectively within the tumor, causing tumor cell death.
“This treatment is currently being trialed in adults diagnosed with recurrent glioblastoma tumors, but has never been attempted in pediatric patients,” said Hasan Syed, M.D., co-director of the Focused Ultrasound Program at Children’s National. “Similar to the adult trial, our protocol involves using a medication that is taken up by tumor cells and then targeting those cells with LIFU to induce tumor cell death, and hopefully leading to tumor control.”
The launch and use of LIFU was possible thanks to the efforts of a multidisciplinary team from various departments that understood if too high a dose of ultrasound was utilized, there could be associated brain swelling and even death.
“Our efforts show great teamwork and a commitment from the hospital and our clinical teams to develop innovative means to treat a tumor that kills 90% of those children afflicted within 18 months of diagnosis,” Dr. Syed said.
The work shows expertise of the brain tumor team, as well as radiology, anesthesiology and intensive care units.
“Despite the risks involved, the use of focused ultrasound is a novel way to try to treat these very deep-seated lesions that have been highly resistant to all forms of therapy and is potentially the greatest breakthrough we’ve had in this disease in the past 50 years,” Dr. Packer said.
What has limited therapy in the past?
DIPGs are deep-seated in critical areas of brain, controlling breathing and heart rate and cannot be removed. The brain has an intrinsic system called a blood brain barrier which blocks drugs from getting to the tumor.
Focused ultrasound is a new way to overcome the brain’s ability to stop the drugs from getting there. It can also be used to activate a drug as it passes through the brain stem.
“We are extremely excited to have taken the first step in developing this novel and non-invasive approach to treating one of our most deadly brain tumors,” Dr. Kilburn said. “This is the first step of numerous steps toward evaluating the many potential uses of LIFU as part of combination therapies to treat children with DIPGs and eventually other pediatric brain tumors.”
Children’s National is partnering with other institutions across the world to perform these studies. But because of the commitment of its team and its expertise, it is the first to use this technique in a child.
“I think we’re in a unique position thanks to the collaborations possible at Children’s National and the expertise of those caring for children with brain tumors,” Dr. Packer added.
Why we’re excited
The Brain Tumor Institute at Children’s National is excited about making this a potential treatment option for DIPG patients, which currently have really no surgical options or alternatives. It’s a way to deliver the ultrasound and therapies in a potentially less toxic way, not requiring surgery.
This trial and subsequently others will give doctors more options for children with DIPGs and other malignant tumors.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2022/09/Patient-undergoing-MRI-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2022-09-19 16:58:392022-12-22 09:15:35Brain tumor team performs first ever LIFU procedure on pediatric DIPG patient
Spearheaded by Javad Nazarian, Ph.D., MSC, Scientific Director of the Children’s National Brain Tumor Institute, the focused DIPG Round Table Discussion brought investigators, neurosurgeons and clinicians from North America, Europe and Australia to Children’s National in Washington, D.C.
Over 40 experts involved in the study and treatment of diffuse intrinsic pontine gliomas (DIPG) convened at the inaugural DIPG Round Table Discussion at Children’s National Health System Sept. 30-Oct. 2.
Spearheaded by Javad Nazarian, Ph.D., MSC, Scientific Director of the Children’s National Brain Tumor Institute, the focused DIPG Round Table Discussion brought investigators, neurosurgeons and clinicians from North America, Europe and Australia to Children’s National in Washington, D.C., to engage in dialogue and learn about the changing landscape of DIPG tumor biology and therapeutics. Attendees discussed the recent discoveries in DIPG research, precision medicine, preclinical modeling, immunotherapy, data sharing and the design of next generation clinical trials.
Families affected by DIPG also had an opportunity to participate in day 2 of the event. Many voiced the necessity of data sharing to ensure progress in the field. Dr. Nazarian seconded that point of view: “It is critical to get raw data and have it harmonized and integrated so that the end users (researchers) can utilize and do cross-data analysis…We need to break down the silos.” The highlight of the data sharing session was the Open DIPG Initiative that is spearheaded by Dr. Nazarian and the Children’s Brian Tumor Tissue Consortium (CBTTC).
Eshini Panditharatna, Ph.D., Madhuri Kambhampati, Sridevi Yadavilli, M.D., Ph.D., and Erin Bonner of Children’s National at the DIPG Round Table.
As recent technological and molecular advances in DIPG biology have pushed the field forward, focus groups have become essential to share data, ideas and resources with the overarching goal of expediting effective treatments for children diagnosed with DIPG. An extremely aggressive form of pediatric brain cancer, DIPG accounts for roughly 10 to 15 percent of all brain tumors in children. Between 300 and 400 children in the United States are diagnosed with DIPG each year, but the 5-year survival for the brain tumor is less than 5 percent, a strikingly low number in comparison with other types of childhood cancer. DIPG research and clinical initiatives have changed in the past years mainly due to the generous support of families for basic research. The DIPG Open Table meeting was designed to coalesce a team of experts to expedite the first crack at curing this devastating childhood cancer.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/10/Javad-Nazarian.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-10-16 13:52:232018-11-26 15:30:47Meeting of the minds: Children’s National hosts first DIPG Round Table Discussion
Javad Nazarian, Ph.D., MSC, has played an important role in establishing the Open DIPG Initiative. He hopes that the Open DIPG Initiative will serve as a model for centralized disease-specific efforts that will bring research findings one step closer to clinical translation.
A collaborative team of doctors and researchers at Children’s National Health System today announced the launch of the Open DIPG Initiative through the Children’s Brain Tumor Tissue Consortium (CBTTC).
The primary goals for the project will be to generate DIPG Omics which will help decipher major molecular characteristics of diffuse intrinsic pontine glioma (DIPG). Specifically, these will include genomics, proteomics, transcriptomics and epigenomics for primary analyses, centralize all DIPG Omics for secondary analyses, integrate the new DIPG data and unify DIPG expertise (data scientists, researchers, new talent, etc.) to analyze the DIPG genomic data.
CBTTC Scientific Co-Chairs Javad Nazarian, Ph.D., MSC, principal investigator, and Adam Resnick, Ph.D., have played important roles in establishing the Open DIPG Initiative. They hope that the Open DIPG Initiative will serve as a model for centralized disease-specific efforts that will bring research findings one step closer to clinical translation.
Pediatric brain tumors are the leading cause of disease-related death in children. Unlike many adult cancers, the causes of pediatric brain tumors remain largely unknown, and common therapies have remained mostly unchanged over the last four decades. To address these challenges, clinicians and researchers have embraced the emergence of sequencing technologies and deep molecular characterization of tumors to define novel, targeted approaches and individualized therapies.
However, harnessing such data-driven approaches has been a challenge due to limited accessibility to datasets and shared discovery platforms that can empower large-scale integration of datasets for worldwide access and cross-disease analyses.
As a part of this initiative, the Open DIPG Initiative has collected, generated and annotated the largest cohort of DIPG genome data to date. Specifically, these datasets contain more than 1,000 genomes associated with pediatric high-grade gliomas, with over 500 DIPG cases. The Open DIPG has been a part of a larger effort known as the Pediatric Brain Tumor Atlas, which aims to uncover the molecular basis of childhood cancers.
Committed to accelerated discovery, the CBTTC is partnering with the Kids First Data Resource Center (DRC) and the newly developed Kids First Data Resource Portal, which was also launched today.
“The combination of consortia-based initiatives, partnerships with foundations and new discovery platforms being announced today, with the support of the National Institutes of Health (NIH), provides for entirely new and transformative ways of doing science on behalf of children with brain tumors,” said Adam Resnick, Ph.D., principal investigator of the Kids First DRC.
The Open DIPG initiative will be launched as a part of the Pediatric Brain Tumor Atlas and has been funded by families as well as the NIH Gabriella Miller Kids First Act fund. The fund was launched in 2015 and named after Gabriella Miller, a former patient at Children’s National who lost her life to DIPG.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/JNazarian.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-09-11 10:43:442018-09-11 10:49:58Children’s National launches Open DIPG Initiative
Researchers nationally and internally stand the best chance of fulfilling Gabriella Miller’s dream of curing childhood cancers by effectively working together, says Javad Nazarian, Ph.D.
“Thank you for helping me reach my goal.” The handwritten note was penned by Gabriella Miller, a patient treated at Children’s National Health System who ultimately succumbed to an aggressive form of pediatric brain cancer.
Gabriella, then 9 years old, dreamed of curing childhood cancer, including diffuse intrinsic pontine glioma (DIPG), the aggressive pediatric brain tumor that took her life.
Attendees will gather April 14, 2018, for an annual gala held by the Smashing Walnuts Foundation – a group Gabriella started – to celebrate their progress on achieving her goal and to chart future strategic approaches.
“While this foundation was the brainchild of a single person, researchers nationally and internally stand the best chance of fulfilling her dream by working together more effectively,” says Javad Nazarian, Ph.D., M.S.C., the gala’s main speaker. Nazarian is scientific director of Children’s Brain Tumor Institute and is scientific co-chair of the Children’s Brain Tumor Tissue Consortium.
To that end, Children’s National was named a member of a public-private research collective awarded up to $14.8 million by the National Institutes of Health (NIH) to launch a data resource center that cancer sleuths around the world can tap into to accelerate discovery of novel treatments for childhood tumors.
This April, the NIH announced that researchers it funded had completed PanCancer Atlas, a detailed genomic analysis on a data set of molecular and clinical information from more than 10,000 tumors representing 33 types of cancer, including DIPG.
And this January, the NIH announced that it would accept applications from researchers performing whole-genome sequencing studies at one of its Gabriella Miller Kids First research program sequencing facilities. The centers will produce genome, exome and transcriptome sequencing.
Expanding access to these growing troves of data requires a close eye on nuts-and-bolts issues, such as securing sufficient physical data storage space to house the data, Nazarian adds. It’s essential for research teams around the world to have streamlined access to data sets they can analyze as well as contribute to.
“In addition to facilitating researchers’ access to this compiled data, we want to ensure that patients and families feel they are partners in this enterprise by also offering opportunities for them to share meaningful clinical data,” Nazarian says.
Nazarian has been instrumental in expanding the comprehensive biorepository at Children’s National, growing it from just a dozen samples six years ago to thousands of specimens donated by patients with all types of pediatric brain tumors, including DIPG.
“We are so grateful to our patients and families. They share our passion for finding cures and validating innovative treatments for pediatric cancers that defy current treatment. They provide funding through their foundations. Families touched by tragedy offer samples to help the next family avoid reliving their experience,” Nazarian says. “It is in their names – and in Gabriella’s name – that we continue to push ourselves to ‘crack the cure’ for childhood brain cancer.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/JNazarian.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2018-04-10 10:17:272020-03-16 11:30:30Private foundation and researchers partner to cure childhood cancers
“This is a tremendous opportunity for children and families whose lives have been forever altered by pediatric cancers,” says Javad Nazarian, Ph.D., M.S.C., principal investigator in the Center for Genetic Medicine Research and scientific director of the Brain Tumor Institute at Children’s National.
Speeding research into pediatric cancers and other diseases relies not only on collecting good data, but making them accessible to research teams around the world to analyze and build on. Both efforts take time, hard work and a significant amount of financial resources – the latter which can often be difficult to attain.
In a move that could considerably advance the field of pediatric cancer, the National Institutes of Health (NIH), a body that funds biomedical research in the United States, recently awarded a public-private research collective that includes Children’s National Health System up to $14.8 million to launch a data resource center for cancer researchers around the world in order to accelerate the discovery of novel treatments for childhood tumors. Contingent on available funds, five years of funding will be provided by the NIH Common Fund Gabriella Miller Kids First Pediatric Research Program, named after Gabriella Miller, a 10-year-old child treated at Children’s National.
As principal investigators, researchers at Children’s Hospital of Philadelphia will lead the joint effort to build out the “Kids First” Data Resource Center. Children’s National in Washington, D.C., will spearhead specific projects, including the Open DIPG project, and as project ambassador will cultivate additional partnerships with public and private foundations and related research consortia to expand a growing trove of data about pediatric cancers and birth defects.
“This is a tremendous opportunity for children and families whose lives have been forever altered by pediatric cancers,” says Javad Nazarian, Ph.D., M.S.C., principal investigator in the Center for Genetic Medicine Research and scientific director of the Brain Tumor Institute at Children’s National. “From just a dozen samples seven years ago, Children’s National has amassed one of the nation’s largest tumor biorepositories funded, in large part, by small foundations. Meanwhile, research teams have been sequencing data from samples here and around the world. With this infusion of federal funding, we are poised to turn these data into insights and to translate those research findings into effective treatments.”
Today’s NIH grant builds on previous funding that Congress provided to the NIH Common Fund to underwrite research into structural birth defects and pediatric cancers. In the first phase, so-called X01 grantees—including Eric Vilain, M.D., Ph.D., newly named director of the Center for Genetic Medicine Research at Children’s National—received funding to sequence genetic data from thousands of patients and families affected by childhood cancer and structural birth defects.
This new phase of funding is aimed at opening access to those genetic sequences to a broader group of investigators around the globe by making hard-to-access data easily available on the cloud. The first project funded will be Open DIPG, run by Nazarian, a single disease prototype demonstrating how the new data resource center would work for multiple ailments.
DIPG stands for diffuse intrinsic pontine glioma, aggressive pediatric brain tumors that defy treatment and are almost always fatal. Just as crowd sourcing can unleash the collective brainpower of a large group to untangle a problem swiftly, open data sharing could accomplish the same for childhood cancers, including DIPG. In addition to teasing out molecular alterations responsible for making such cancers particularly lethal, pooling data that now sits in silos could help to identify beneficial mutations that allow some children to survive months or years longer than others.
“It’s a question of numbers,” Dr. Vilain says. “The bottom line is that making sense of the genomic information is significantly increased by working through large consortia because they provide access to many more patients with the disease. What is complicated about genetics is we all have genetic variations. The challenge we face is teasing apart regular genetic variations from those genetic variations that actually cause childhood cancers, including DIPG.”
Nazarian predicts some of the early steps for the research consortium will be deciding nuts-and-bolts questions faced by such a start-up venture, such as the best methods to provide data access, corralling the resources needed to store massive amounts of data, and providing data access and cross correlation.
“One of the major challenges that the data resource center will face is to rapidly establish physical data storage space to store all of the data,” Nazarian says. “We’re talking about several petabytes—1,000 terabytes— of data. The second challenge to address will be data dissemination and, specifically, correlation of data across platforms representing different molecular profiles (genome versus proteome, for example). This is just the beginning, and it is fantastic to see a combination of public and private resources in answering these challenges.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2017/02/JNazarian.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2017-08-23 14:34:292021-09-20 09:38:15Advancing pediatric cancer research by easing access to data
Mutations in histone-encoding genes are associated with the vast majority of pediatric DIPG cases.
For more than four decades, clinicians around the nation have been giving the parents of pediatric patients diagnosed with diffuse intrinsic pontine glioma (DIPG) the same grim prognosis. In the past five years, there has been an explosion of innovative research at Children’s National Health System and elsewhere that promises to change that narrative. That’s because the black box that is DIPG is beginning to divulge its genetic secrets. The new-found research knowledge comes as a direct result of parents donating specimens, judicious shepherding of these scarce resources by researchers, development of pre-clinical models, and financing from small foundations.
From just 12 samples six years ago, Children’s National has amassed one of the nation’s largest tumor bio banks – 3,000 specimens donated by more than 900 patients with all types of pediatric brain tumors, including DIPG.
Such donated specimens have led to the identification of H3K27M mutations, a groundbreaking finding that has been described as the single-most important discovery in DIPG. Mutations in histone-encoding genes are associated with the vast majority of pediatric DIPG cases.
Histone mutations (also referred to as oncohistones) are sustained in the tumor throughout its molecular evolution, found a research team led by Javad Nazarian, Ph.D. Not only were H3K27M mutations nearly ubiquitous in all samples studied, the driver mutation maintained partnerships with other secondary mutations as DIPG tumor cells spread throughout the developing brain. Children’s National researchers have identified tumor driver mutations and obligate partner mutations in DIPG. They are examining what happens downstream from the histone mutation – changes in the genome that indicate locations they can target in their path toward personalized medicine. The value of that genomic knowledge is akin to emergency responders being told the specific house where their help is needed, rather than a ZIP code or city name, Dr. Nazarian says. While there is currently no effective treatment for DIPG, new research has identified a growing number of genomic targets for future therapeutics.“That changed the dynamic,” says Dr. Nazarian. “In DIPG clinical research, nothing had changed for 45 years. Now we know some of the genomic mutations, how the tumor was evolving – gaining new mutations, losing mutations. With precision medicine, we can target those mutations.”
Another study led by neuro-oncologist Eugene Hwang, M.D., reported the most comprehensive phenotypic analyses comparing multiple sites in a young girl’s primary and metastatic tumors. This study showed that despite being uniform, small molecules (mRNA) could be used to distinguish an evolved tumor from its primary original tumor mass.Key to this multidisciplinary work is collaboration across divisions and departments. Within the research lab, knowledge about DIPG is expanding.
Each member of the DIPG team – neurosurgery, neuro-oncology, immunology, genomics, proteomics – feeds insight back to the rest of the team, accelerating the pace of research discoveries being translated into clinical care. Among the challenges that the team will address in the coming months is outmaneuvering tumors that outsmart T-cells (immune cells).
“What is happening in the checkpoint inhibitor field is exciting,” says Catherine M. Bollard, MBChB, MD, Chief of Allergy and Immunology and Director of the Program for Cell Enhancement of Technologies for Immunotherapy. “The inhibitors work by reversing the ‘off’ switch – releasing the brake that has been placed on the T-cells so they can again attack multiple tumor proteins. The next exciting step, and novel to Children’s National, will be to combine this approach with T-cell therapies specifically designed to attack the DIPG tumors. Unlike the use of combination chemotherapy, which has had a limited impact, we hope that the novel combination of immunotherapeutic approaches will offer the hope of a potential cure.”
Dr. Hwang, another member of the multidisciplinary team, adds: “When you’re looking at the landscape – for me, at least – it starts and ends with how my patients are doing. There are kids for whom we have had great successes in improving survival rates in some cancers, like leukemia, and some where the needle has moved nowhere, like DIPG. We’re still trying to figure out the whole picture of who responds. The immune system is present in all kids. Its ability to attack is present in all kids.”
Children’s National is one of the few hospitals in the nation that conducts brainstem biopsies for DIPG and does so with very little chance of complications. The pons is like a superhighway through which nerves pass, making it instrumental in smooth operation of such vital functions as breathing, heart rate, sleeping, and consciousness. The ability of neurosurgeon Suresh Magge, MD, to perform such sensitive biopsies upends conventional wisdom that these procedures were inherently too dangerous. Within two weeks of diagnosis, genomics analyses are run to better understand the biology of that specific tumor. Within the following weeks, the tumor board occurs, and patients with DIPG are placed on therapy that best targets their tumor’s mutations.
The black box that is diffuse intrinsic pontine glioma is beginning to divulge its genetic secrets.
Despite an increasing number of experimental therapies tested via clinical trials, more than 95 percent of children with DIPG die within two years of diagnoses. Biomarkers that point to DIPG – like the copies of DNA that tumors shed and leave behind in the bloodstream – could enable creation of liquid biopsies, compared with today’s surgical approach.
Children’s also is making a concerted effort to create preclinical models of DIPG. Preclinical models will be used to winnow the field of potential therapeutics to the candidates most likely to help children survive DIPG. The preclinical tumor cells will be labeled with luciferase – enzymes that, like photoproteins, produce bioluminescence – permitting the researcher to visually see the formation, progression, and response of DIPG tumors to treatment in preclinical settings.
These preclinical models could be used to test multiple drug combinations in conjunction with radiation therapy. Molecular signatures and response to treatment could then be assessed to learn how the tumor resists therapy. Due to the obligate partnerships between driver mutations and secondary mutations, the research team already knows that effective DIPG medicines will need more than one target. If there were a single mutation, that would be like having a single master key to open many locks. Multiple mutations imply that more than one key will be needed. Thus, the search for cures for DIPG will necessitate taking a multi-pronged approach.
Combined drug regimens, including those created with proprietary technology, with or without radiation, will be keys to targeting myriad mutations in order to kill tumors where they are. Those drug combinations that demonstrate they can do their jobs – slowing tumor growth, increasing chances of survival, taming toxicity – will be selected for clinical application.
Immunotherapy leverages T-cells, the immune system’s most able fighters, to help in the overall goal of extending patients’ survival. One of the most challenging aspects of pediatric brain tumors is the body does a very good job of shielding the brain from potential pathogens. Precise drug delivery means finding innovative ways for therapeutics to cross the blood-brain barrier in order to reach the tumor. The team has identified one such potential target, the protein NG2, which may represent a good target for immune therapy. The protein is expressed in primitive cells that have not become specialized – meaning there may be an opportunity to intervene before it is driven to become a tumor cell.
What’s Known Despite multiple clinical trials testing an assortment of new treatments, the survival rate for diffuse intrinsic pontine glioma (DIPG) remains abysmal, with most children succumbing to the pediatric brainstem tumor within 12 months of diagnosis. Focal radiation therapy, the primary treatment approach, has not improved overall survival. While the majority of DIPG tumors grow within the brainstem, metastases can occur elsewhere in the brain. Due to recent availability of tissue, new data are emerging about the biologic behavior of tumors, details that could be instrumental in constructing optimal treatment strategies.
What’s New
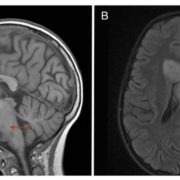
An otherwise healthy 9-year-old girl developed weakness in the left side of her face; magnetic resonance imagining revealed T2/FLAIR hyperintensity centered within and expanding the pons. Despite various treatments, her pontine lesion increased in size and new metastases were noted. The team led by Children’s National Health System researchers is the first to report comprehensive phenotypic analyses comparing multiple sites in primary and distant tumors. All tumor sites displayed positive staining for the H3K27M mutation, a mutation described in more than two-thirds of DIPGs that may portend a worse overall survival. Persistence of mutational status across multiple metastatic sites is particularly important since the effectiveness of some therapeutic approaches relies on this occurring. mRNA analyses, by contrast, identified a small number of genes in the primary tumor that differed from one metastatic tumor. This divergence implies that a single biopsy analysis for mRNA expression has the potential to be misleading.
Questions for Future Research Q: Because a small cohort of genes in the girl’s primary tumor were different from genes in portions of the metastatic tumor, would genomic and proteomic analyses provide additional details about this genetic evolution? Q: How do site-specific differences in mRNA expression affect decisions about which therapies to provide and in which order?
Source: “Histological and Molecular Analysis of a Progressive Diffuse Intrinsic Pontine Glioma and Synchronous Metastatic Lesions: A Case Report.” J. Nazarian, G.E. Mason, C.Y. Ho, E. Panditharatna, M. Kambhampati, L.G. Vezina, R.J. Packer, and E.I. Hwang. Published by Oncotarget on June 14, 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@G_Histological-DIPG-image.jpg326700Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-06-14 17:10:192024-02-02 14:39:53Analysis of a progressive diffuse intrinsic pontine glioma: a case report
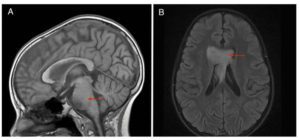
What’s Known Needle biopsies help to guide diagnosis and targeted therapies for diffuse intrinsic pontine gliomas (DIPGs), which make up 10 percent to 15 percent of all pediatric brain tumors but carry a median survival of 9 to 12 months. This dismal survival rate compares with a 70 percent chance of children surviving other central nervous system tumors five years post diagnosis. In DIPG, tumors appear in the pons, an area of the brain that houses cranial nerve nuclei. Surgical options are limited. Spatial and temporal tumor heterogeneity is a major obstacle to accurate diagnosis and successful targeted therapy.
What’s New
The team sought to better define DIPG heterogeneity. They analyzed 134 specimens from nine patients and found that H3K27M mutations were ubiquitous in all 41 samples with oncogenic content, and always were associated with at least one partner driver mutation: TP53, PPM1D, ACVR1 or PIK3R1. These H3K27M mutations are the initial oncogenic event in DIPG, writes the research team led by Children’s National Health System. “Driver” mutations, such as H3K27M, are essential to begin and sustain tumor formation. This main driver partnership is maintained throughout the course of the disease, in all cells across the tumor, and as tumors spread throughout the brain. Because homogeneity for main driver mutations persists for the duration of illness, efforts to cure DIPG should be directed at the oncohistone partnership, the authors write. Based on early tumor spread, efforts to cure DIPG should aim for early systemic tumor control, rather focused exclusively on the pons.
Questions for Future Research Q: If a larger sample size were analyzed, what would it reveal about the true heterogeneity/homogeneity status of DIPGs? Q: “Accessory” driver mutations are not absolutely essential but do help to further promote and accelerate tumor growth. What is their precise role?
Source: “Spatial and Temporal Homogeneity of Driver Mutations in Diffuse Intrinsic Pontine Glioma.” H. Nikbakht, E. Panditharatna, L.G. Mikael, R. Li, T. Gayden, M. Osmond, C.Y. Ho, M. Kambhampati, E.I. Hwang, D. Faury, A. Siu, S. Papillon-Cavanagh, D. Bechet, K.L. Ligon, B. Ellezam, W.J. Ingram, C. Stinson, A.S. Moore, K.E. Warren, J. Karamchandani, R.J. Packer, N. Jabado, J. Majewski, and J. Nazarian. Published by Nature Communications on April 6, 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/04/R@GSpatialDIPG_Image-1.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-04-06 17:36:362018-07-19 12:56:10Spatial and temporal homogeneity of driver mutations in diffuse intrinsic pontine glioma
What’s Known Neuron glia antigen-2 (NG2) is a protein expressed by many central nervous system cells during development and differentiation. NG2-expressing oligodendrocyte progenitor cells have been identified as the cells of origin in gliomas, tumors that arise from the brain’s gluey supportive tissue. What’s more, NG2 expression also has been associated with childhood diffuse intrinsic pontine glioma (DIPG) an aggressive tumor that accounts for 10 percent to 20 percent of pediatric central nervous system (CNS) tumors. Radiation can prolong survival by a few months, but children diagnosed with DIPG typically survive less than one year.
What’s New
Researchers are searching for appropriate targets and effective drugs that offer some chance of benefit. A team of Children’s National Health System researchers investigated whether NG2 – which plays a critical role in proliferation and development of new blood vessels and promotes tumor infiltration – could be a potential target for cancer treatment. Of the various options, antibody-mediated mechanisms of targeting NG2 are feasible, but the size of antibodies limits their ability to cross the blood-brain barrier. “Due to its role in maintaining a pluripotent pool of tumor cells, and its role in tumor migration and infiltration, NG2 provides multiple avenues for developing therapeutics,” the research team concludes. “Moreover, the large extracellular domain of NG2 provides an excellent antigen repertoire for immunotherapeutic interventions. As such, further research is warranted to define the role and expression regulation of NG2 in CNS cancers.”
Questions for Future Research
Q: Because healthy oligodendrocyte progenitor cells are important for the child’s developing brain, how could further characterization of NG2 isoforms help prevent drugs from damaging those beneficial cells?
Q: Could NG2-binding peptides cross the blood-brain barrier to deliver anti-cancer therapies precisely to tumor sites?
Source: “The Role of NG2 Proteoglycan in Glioma.” S. Yadavilli, E.I. Hwang, R. J. Packer, and J. Nazarian. Published by Translational Oncology on February 2016.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GNG2DIPG-Image-e1496433328865.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2016-02-21 10:35:162018-05-02 16:57:25The role of NG2 proteoglycan in glioma
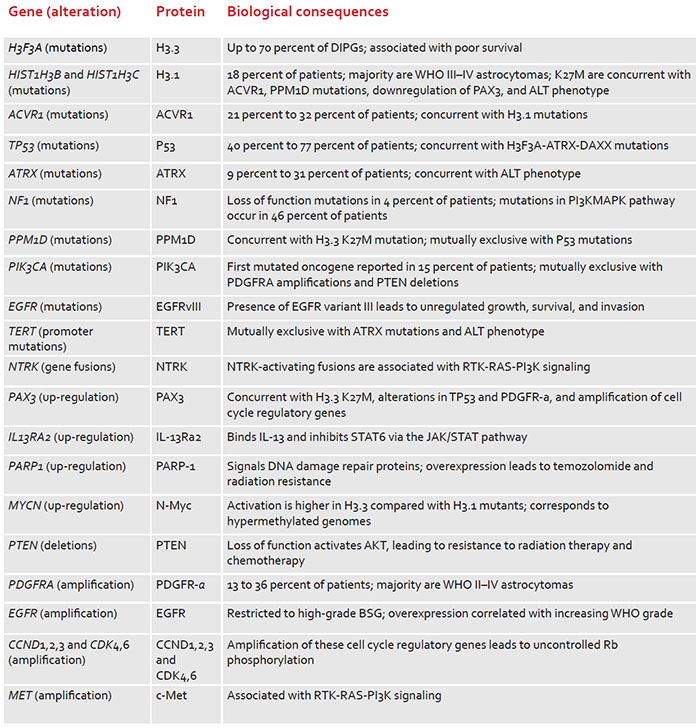
What’s Known Fewer than 150 U.S. children per year are diagnosed with diffuse intrinsic pontine glioma (DIPG), one of the most lethal pediatric central nervous system cancers. Despite an increasing number of experimental therapies tested via clinical trials, more than 95 percent of these children die within two years of diagnosis. Molecular studies have yielded additional insight about DIPG, including that mutations in histone-encoding genes are associated with 70 percent of cases. Understanding mutations that drive tumors and the genomic landscape can help to guide development of targeted therapies.
What’s New: Frequently found genetic alterations prevalent in DIPGs
https://innovationdistrict.childrensnational.org/wp-content/uploads/2016/09/R@GGenomicDIPG_Image-e1496432847469.jpg200300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2015-05-01 11:21:292018-05-02 16:57:25Clinicopathology of diffuse intrinsic pontine glioma and its redefined genomic and epigenomic landscape

 A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.
A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.