Stroke alert teams beneficial to timely diagnosis of pediatric stroke patients
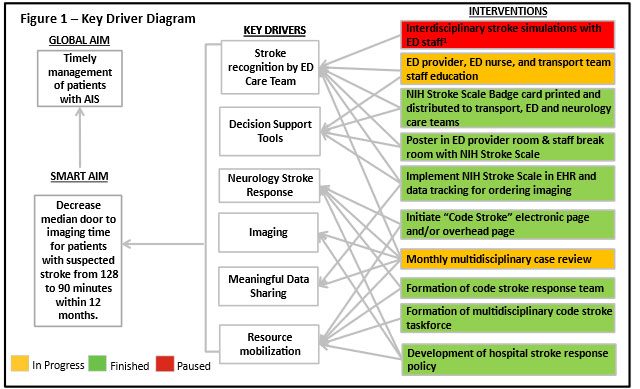
1 – Interdisciplinary stroke simulations were canceled due to short staffing and insufficient nursing support during COVID-19 pandemic.
Diagnosis times improved for pediatric arterial ischemic stroke (AIS) patients in the emergency department after the implementation of a quality improvement initiative. According to a new study, published in Pediatrics, the median door-to-imaging time for children with suspected AIS improved from 128 minutes to 68 minutes post-intervention.
What it means
Pediatric AIS is an important cause of morbidity and mortality that requires early recognition to benefit from hyperacute therapies. A quality improvement study at Children’s National Hospital aimed to improve timely diagnosis of AIS through an interdisciplinary stroke response protocol. The researchers implemented a quality improvement initiative from November 2019 to June 2023 in the emergency department that included interventions under two categories – workflow efficiency improvement and staff education. A total of 71 patients who met the criteria for the study were analyzed. Median door-to-imaging time for all patients improved from 128 minutes during the baseline period to 68 minutes.
The researchers note that establishing a well-functioning stroke response protocol is a critical step in detecting pediatric stroke in the community and expediting care for this vulnerable patient population.
“This study highlights the value of quality improvement methodologies in coordinating multiple hospital divisions for the greater goal of improving patient care,” says Theodore Trigylidas, MD, corresponding author and emergency medicine physician at Children’s National. “We hope it serves as a template for other healthcare organizations in developing their own pediatric stroke protocols.”
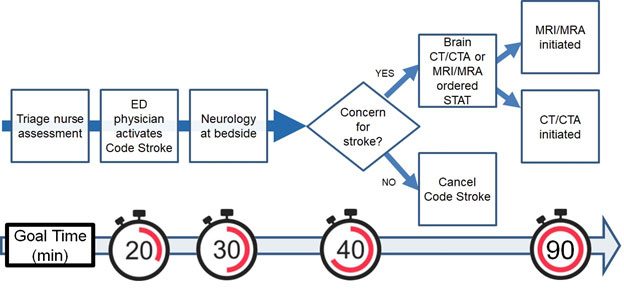
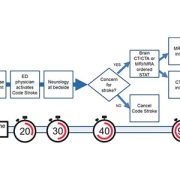
Code Stroke management algorithm. CT/CTA, computed tomography with or without angiography. MRI/MRA, magnetic resonance imaging with or without angiography.
The hold up in the field
The rarity of AIS in pediatric patients and stroke mimics, like hemiplegic migraine, may cause challenges for a timely diagnosis, and treatments for AIS – thrombolysis and thrombectomy – must be performed within specific time frames.
Moving the field forward
“By taking into consideration local staffing structures and institutional resource availability, the quality improvement approach described here can serve as a framework for how institutions might implement a pediatric acute stroke response protocol given their own unique systems of care and resource considerations,” says Dana Harrar, MD, PhD, study author and director, Pediatric Stroke Program at Children’s National.
The authors plan to expand this initiative to incorporate children at outside facilities with the goal of creating a stroke network with nearby hospitals.
Authors from Children’s National include: Theodore Trigylidas, MD, Nichole McCollum, MD, Kathleen Brown, MD, Paola Pergami, MD, Elizabeth Wells, MD, Jonathan Murnick, MD, PhD, Josh Heffren, PharmD, BCPPS and Deborah LaViolette, BSN, Dana Harrar, MD, PhD.
You can read the full study, Improving Timely Diagnosis of Arterial Ischemic Stroke at the Pediatric Emergency Department in Pediatrics.


 Thousands of medical professionals and researchers from around the world gathered in San Diego this October for
Thousands of medical professionals and researchers from around the world gathered in San Diego this October for