
COVID-19 Pandemic: 3rd Annual CN – NIAID Virtual Symposium
The CN-NIAID Virtual Symposium highlighted work being done to fight the COVID-19 pandemic globally.
Public Health
The CN-NIAID Virtual Symposium highlighted work being done to fight the COVID-19 pandemic globally.


In a cohort retrospective study comparing clinical features of COVID-19 and seasonal flu, researchers found surprisingly little difference in the rates of hospitalization, admission to the intensive care unit and mechanical ventilator use between the two groups.
As the fall approaches, pediatric hospitals will start seeing children with seasonal influenza A and B. At the same time, COVID-19 will be co-circulating in communities with the flu and other respiratory viruses, making it more difficult to identify and prevent the novel coronavirus.
With little published data directly comparing the clinical features of children with COVID-19 to those with seasonal flu, researchers at Children’s National Hospital decided to conduct a retrospective cohort study of patients in the two groups. Their findings — published September 8 in JAMA Network Open — surprised them.
The study — detailed in the article “Comparison of Clinical Features of US Children With COVID-19 vs Seasonal Influenza A and B” — showed no statistically significant differences in the rates of hospitalization, admission to the intensive care unit and mechanical ventilator use between the two groups.
The other unexpected finding was that more patients with COVID-19 than those with seasonal influenza reported fever, cough, diarrhea or vomiting, headache, body ache or chest pain at the time of diagnosis, says Xiaoyan Song, Ph.D., M.Sc., M.B., the study’s principal investigator.
“I didn’t see this coming when I was thinking about doing the study,” says Dr. Song, director of Infection Control and Epidemiology at Children’s National since 2007 and a professor of pediatrics at the George Washington University School of Medicine and Health Sciences. “It took several rounds of thinking and combing through the data to convince myself that this was the conclusion.”
Given that much remains unknown about COVID-19, the researchers’ discovery that children with the disease present with more symptoms at the time of diagnosis is a valuable one.
“It’s a good cue from a prevention and planning perspective,” says Dr. Song. “We always emphasize early recognition and early isolation with COVID. Having a clinical picture in mind will assist clinicians as they diagnose patients with symptoms of the coronavirus.”
The study included 315 children who were diagnosed with a laboratory-confirmed COVID-19 between March 25, 2020, and May 15, 2020, and 1,402 children who were diagnosed with a laboratory-confirmed seasonal influenza between Oct. 1, 2019, and June 6, 2020, at Children’s National. Asymptomatic patients who tested positive for COVID-19 during pre-admission or pre-procedural screening were excluded from the study.
Of the 315 patients who tested positive for COVID-19, 52% were male, with a median age of 8.4 years. Of these patients, 54 (17.1 %) were hospitalized, including 18 (5.7%) who were admitted to the intensive care unit (ICU) and 10 (3.2%) who received mechanical ventilator treatment.
Among the 1,402 patients who tested positive for influenza A or B, 52% were male, with a median age of 3.9 years, and 291 (21.2%) were hospitalized, including 143 for influenza A and 148 for influenza B. Ninety-eight patients (7.0%) were admitted to the ICU, and 27 (1.9%) received mechanical ventilator support.
The study showed a slight difference in the age of children hospitalized with COVID-19 compared to those hospitalized with seasonal influenza. Patients hospitalized with COVID-19 had a median age of 9.7 years vs. those hospitalized with seasonal influenza who had a median age of 4.2 years.
In both groups, fever was the most often reported symptom at the time of diagnosis followed by cough. A greater proportion of patients hospitalized with COVID-19 than those hospitalized with seasonal influenza reported fever (76% vs. 55%), cough (48% vs. 31%), diarrhea or vomiting (26% vs. 12%), headache (11% vs. 3%), body ache/myalgia (22% vs. 7%), and chest pain (11% vs. 3%).
More patients hospitalized with COVID-19 than those with seasonal influenza reported sore throat or congestion (22% vs. 20%) and shortness of breath (30% vs. 20%), but the differences were not statistically significant.
During the study period, the researchers noticed an abrupt decline of influenza cases at Children’s National after local schools closed in mid-March and stay-at-home orders were implemented about two weeks later to combat the community spread of COVID-19. Dr. Song says the impact of school closures on the spread of COVID-19 among children is the next area of study for her research team.
“We want to assess the quantitative impact of school closures so we can determine at what point the cost of closing schools and staying at home outweighs the benefit of reducing transmission of COVID-19 and burdens on the health care system,” she says.
Dr. Song urges members of the community “first and foremost to stay calm and be strong. We’re learning new and valuable things about this virus each day, which in turn improves care. The collision of the flu and COVID-19 this fall could mean an increase in pediatric hospitalizations. That’s why it’s important to get your flu shot, because it can help take at least one respiratory virus out of circulation.”
Other researchers who contributed to this study include Meghan Delaney, D.O.; Rahul K. Shah, M.D.; Joseph M. Campos, Ph.D.; David L. Wessel, M.D.; and Roberta L. DeBiasi, M.D.


New research suggests that children can shed SARS-CoV-2, the virus that causes COVID-19, even if they never develop symptoms or for long after symptoms have cleared. But many questions remain about the significance of the pediatric population as vectors for this sometimes deadly disease.
New research suggests that children can shed SARS-CoV-2, the virus that causes COVID-19, even if they never develop symptoms or for long after symptoms have cleared. But many questions remain about the significance of the pediatric population as vectors for this sometimes deadly disease, according to an invited commentary by Children’s National Hospital doctors that accompanies this new study published online Aug. 28, 2020 in JAMA Pediatrics. The commissioned editorial, written by Roberta L. DeBiasi, M.D., M.S., chief of the Division of Infectious Diseases, and Meghan Delaney, D.O., M.P.H., chief of the Division of Pathology and Lab Medicine, provides important insight on the role children might play in the spread of COVID-19 as communities continue to develop public health strategies to reign in this disease.
The study that sparked this commentary focused on 91 pediatric patients followed at 22 hospitals throughout South Korea. “Unlike in the American health system, those who test positive for COVID-19 in South Korea stay at the hospital until they clear their infections even if they aren’t symptomatic,” explains Dr. DeBiasi.
The patients here were identified for testing through contact tracing or developing symptoms. About 22% never developed symptoms, 20% were initially asymptomatic but developed symptoms later, and 58% were symptomatic at their initial test. Over the course of the study, the hospitals where these children stayed continued to test them every three days on average, providing a picture of how long viral shedding continues over time.
The study’s findings show that the duration of symptoms varied widely, from three days to nearly three weeks. There was also a significant spread in how long children continued to shed virus and could be potentially infectious. While the virus was detectable for an average of about two-and-a-half weeks in the entire group, a significant portion of the children — about a fifth of the asymptomatic patients and about half of the symptomatic ones — were still shedding virus at the three week mark.
Drs. DeBiasi and Delaney write in their commentary that the study makes several important points that add to the knowledge base about COVID-19 in children. One of these is the large number of asymptomatic patients — about a fifth of the group followed in this study. Another is that children, a group widely thought to develop mostly mild disease that quickly passes, can retain symptoms for weeks. A third and important point, they say, is the duration of viral shedding. Even asymptomatic children continued to shed virus for a long time after initial testing, making them potential key vectors.
However, the commentary authors say, despite these important findings, the study raises several questions. One concerns the link between testing and transmission. A qualitative “positive” or “negative” on testing platforms may not necessarily reflect infectivity, with some positives reflecting bits of genetic material that may not be able to make someone sick or negatives reflecting low levels of virus that may still be infectious.
Testing reliability may be further limited by the testers themselves, with sampling along different portions of the respiratory tract or even by different staff members leading to different laboratory results. It’s also unknown whether asymptomatic individuals are shedding different quantities of virus than those with symptoms, a drawback of the qualitative testing performed by most labs. Further, testing only for active virus instead of antibodies ignores the vast number of individuals who may have had and cleared an asymptomatic or mild infection, an important factor for understanding herd immunity.
Lastly, Drs. DeBiasi and Delaney point out, the study only tested for viral shedding from the respiratory tract even though multiple studies have detected the virus in other bodily fluids, including stool. It’s unknown what role these other sources might play in the spread of this disease.
Drs. DeBiasi and Delaney note that each of these findings and additional questions could affect public health efforts continually being developed and refined to bring COVID-19 under control in the U.S. and around the world. Children’s National has added their own research to these efforts, with ongoing studies to assess how SARS-CoV-2 infections proceed in children, including how antibodies develop both at the individual and population level.
“Each of these pieces of information that we, our collaborators and other scientists around the world are working to gather,” says Dr. DeBiasi, “is critical for developing policies that will slow the rate of viral transmission in our community.”

Minority and socioeconomically disadvantaged children have significantly higher rates of COVID-19 infection, a new study led by Children’s National Hospital researchers shows.
Minority and socioeconomically disadvantaged children have significantly higher rates of COVID-19 infection, a new study led by Children’s National Hospital researchers shows. These findings, reported online August 5 in Pediatrics, parallel similar health disparities for the novel coronavirus that have been found in adults, the authors state.
COVID-19, an infection caused by the novel coronavirus SARS-CoV-2 that emerged in late 2019, has infected more than 4.5 million Americans, including tens of thousands of children. Early in the pandemic, studies highlighted significant disparities in the rates of infection in the U.S., with minorities and socioeconomically disadvantaged adults bearing much higher burdens of infection. However, says Monika Goyal, M.D., M.S.C.E, a pediatric emergency medicine specialist and associate division chief in the Division of Emergency Medicine at Children’s National whose research focuses on health disparities, it’s been unclear whether these disproportionate rates of infection also extend to youth.
To investigate this question, she and her colleagues looked to data collected between March 21, 2020, and April 28, 2020, from a drive-through/walk-up COVID-19 testing site affiliated with Children’s National — one of the first exclusively pediatric testing sites for the virus in the U.S. To access this free testing site, funded by philanthropic support, patients between the ages of 0 and 22 years needed to meet specific criteria: mild symptoms and either known exposure, high-risk status, family member with high-risk status or required testing for work. Physicians referred patients through an online portal that collected basic demographic information, reported symptoms and the reason for referral.
When Dr. Goyal and her colleagues analyzed the data from the first 1,000 patients tested at this site, they found that infection rates differed dramatically among different racial and ethnic groups. While about 7% of non-Hispanic white children were positive for COVID-19, about 30% of non-Hispanic Black and 46% of Hispanic children were positive.
“You’re going from about one in 10 non-Hispanic white children to one in three non-Hispanic Black children and one in two Hispanic children. It’s striking,” says Dr. Goyal.
Using data from the American Families Survey, which uses five-year census estimates derived from home address to estimate median family income, the researchers separated the group of 1,000 patients into estimated family income quartiles. They found marked disparities in COVID-19 positivity rates by income levels: while those in the highest quartile had infection rates of about 9%, about 38% of those in the lowest quartile were infected.
There were additional disparities in exposure status, Dr. Goyal adds. Of the 10% of patients who reported known exposure to COVID-19, about 11% of these were non-Hispanic white. However, non-Hispanic Black children were triple this number.
Although these numbers show clear disparities in COVID-19 infection rates, the authors are now trying to understand why these disparities occur and how they can be mitigated.
“Some possible reasons may be socioeconomic factors that increase exposure, differences in access to health care and resources, as well as structural racism,” says Dr. Goyal.
She adds that Children’s National is working to address those factors that might increase risk for COVID-19 infection and poor outcomes by helping to identify unmet needs — such as food and/or housing insecurity — and steer patients toward resources when patients receive their test results.
“As clinicians and researchers at Children’s National, we pride ourselves on not only being a top-tier research institution that provides cutting-edge care to children, but by being a hospital that cares about the community we serve,” says Denice Cora-Bramble, M.D., M.B.A., chief medical officer of Ambulatory and Community Health Services at Children’s National and the research study’s senior author. “There’s still so much work to be done to achieve health equity for children.”
Other Children’s National researchers who contributed to this study include Joelle N. Simpson, M.D.; Meleah D. Boyle, M.P.H, Gia M. Badolato, M.P.H; Meghan Delaney, D.O,. M.P.H.; and Robert McCarter Jr., Sc.D.
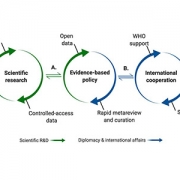
Since COVID-19 emerged late last year, there’s been an enormous amount of research produced on this novel coronavirus disease. But the content publicly available for this data and the format in which it’s presented lack consistency across different countries’ national public health institutes, greatly limiting its usefulness, Children’s National Hospital scientists report in a new study. Their findings and suggestions, published online August 19 in Science & Diplomacy, could eventually help countries optimize their COVID-19-related data — and data for future outbreaks of other diseases — to help further new research, clinical decisions and policy-making around the world.
Recently, explains study senior author Emmanuèle Délot, Ph.D., research faculty at Children’s National Research Institute, she and her colleagues sought data on sex differences between COVID-19 patients around the world for a new study. However, she says, when they checked the information available about different countries, they found a startling lack of consistency, not only for sex-disaggregated data, but also for any type of clinical or demographic information.
“The prospects of finding the same types of formats that would allow us to aggregate information, or even the same types of information across different sites, was pretty dismal,” says Dr. Délot.
To determine how deep this problem ran, she and colleagues at Children’s National, including Eric Vilain, M.D., Ph.D., the James A. Clark Distinguished Professor of Molecular Genetics and the director of the Center for Genetic Medicine Research at Children’s National, and Jonathan LoTempio, a doctoral candidate in a joint program with Children’s National and George Washington University, surveyed and analyzed the data on COVID-19.
The research spanned data reported by public health agencies from highly COVID-19 burdened countries, viral genome sequence data sharing efforts, and data presented in publications and preprints.
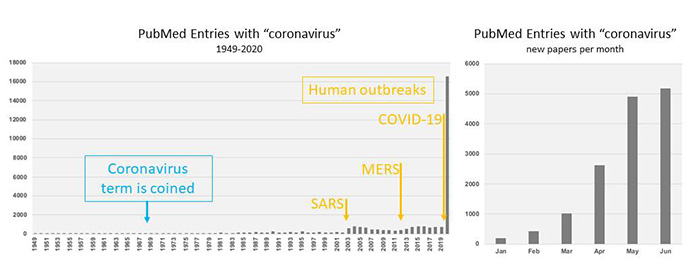
Publications with the term “coronavirus” archived in PubMed over time.
At the time of study, the 15 countries with the highest COVID-19 burden at the time included the US, Spain, Italy, France, Germany, the United Kingdom, Turkey, Iran, China, Russia, Brazil, Belgium, Canada, the Netherlands and Switzerland. Together, these countries represented more than 75% of the reported global cases. The research team combed through COVID-19 data presented on each country’s public health institute website, looking first at the dashboards many provided for a quick glimpse into key data, then did a deeper dive into other data on this disease presented in other ways.
The data content they found, says LoTempio, was extremely heterogeneous. For example, while most countries kept running totals on confirmed cases and deaths, the availability of other types of data — such as the number of tests run, clinical aspects of the disease such as comorbidities, symptoms, or admission to intensive care, or demographic information on patients, such as age or sex — differed widely among countries.
Similarly, the format in which data was presented lacked any consistency among these institutes. Among the 15 countries, data was presented in plain text, HTML or PDF. Eleven offered an interactive web-based data dashboard, and seven had comma-separated data available for download. These formats aren’t compatible with each other, LoTempio explains, and there was little to no documentation about where the data that supplies some formats — such as continually updated web-based dashboards — was archived.
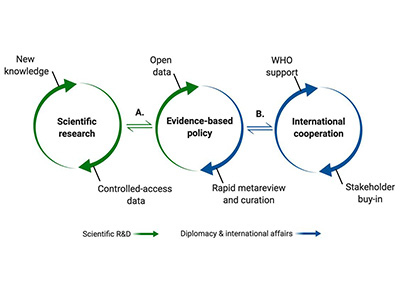
Graphic representation of the science-policy interface.
Dr. Vilain says that a robust system is already in place to allow uniform sharing of data on flu genomes — the World Health Organization’s (WHO) Global Initiative on Sharing All Influenza Data (GISAID) — which has been readily adapted for the virus that causes COVID-19 and has already helped advance some types of research. However, he says, countries need to work together to develop a similar system for harmonized sharing other types of data for COVID-19. The study authors recommend that COVID-19 data should be shared among countries using a standardized format and standardized content, informed by the success of GISAID and under the backing of the WHO.
In addition, the authors say, the explosion of research on COVID-19 should be curated by experts who can wade through the thousands of papers published on this disease since the pandemic began to identify research of merit and help merge clinical and basic science.
“Identifying the most useful science and sharing it in a way that’s usable to most researchers, clinicians and policymakers, will not only help us emerge from COVID-19 but could help us prepare for the next pandemic,” Dr. Vilain says.
Other researchers who contributed to this study include D’Andre Spencer, MPH, Rebecca Yarvitz, BA, and Arthur Delot-Vilain.

Sixteen finalists have been selected in the “Make Your Medical Device Pitch for Kids!” special COVID-19 edition competition presented by the National Capital Consortium for Pediatric Device Innovation (NCC-PDI). Representing innovations in COVID-19-related pediatric medical devices, the finalists will compete in a virtual pitch event held on July 20,2020 where up to $250,000 in awards will be given. Winners will receive grant funding of up to $50,000.
The competition is led by NCC-PDI co-founders the Sheikh Zayed Institute for Pediatric Surgical Innovation at Children’s National Hospital and the A. James Clark School of Engineering at the University of Maryland and powered by nonprofit accelerator and NCC-PDI member, MedTech Innovator.
This competition focuses on pediatric medical devices that support home health monitoring and telehealth, and improve sustainability, resiliency and readiness in diagnosing and treating children during a pandemic.
“As COVID -19 continues to threaten the health of families and children across the nation, we must continue to seek new and better ways to deliver quality care during a pandemic and offer technology solutions to reopen more safely,” says Kolaleh Eskandanian, Ph.D., MBA, PMP, vice president and chief innovation officer at Children’s National Hospital and principal investigator of NCC-PDI. “Competitions like this are vital to get ahead of the healthcare challenge that COVID-19 presents in the world of pediatrics. By supporting innovation, we provide critical breakthroughs that can positively impact the lives of the children and families we serve.”
Along with grant funding, one company from the competition will be selected by Johnson & Johnson Innovation – JLABS to receive a one-year residency at JLABS @ Washington, DC, which will be located on the new Children’s National Research & Innovation Campus currently under construction. In addition to the 2021 JLABS residency, the awardee will have access to the JLABS community and expert mentoring by the Johnson & Johnson family of companies.
The 16 pediatric device innovations that judges selected for the final competition include:
Funding for the competition is made possible by a grant from the Food and Drug Administration (FDA) and a philanthropic gift from Mei Xu, founder of e-commerce platform Yes She May, a site dedicated to women-owned brands.
In addition to this COVID-19 special edition event, NCC-PDI recently revealed the ten finalists in its prestigious 8th annual “Make Your Medical Device Pitch for Kids!” competition. Cardiovascular, NICU, and orthopaedic and spine device innovations are the focus of the fall competition, taking place October 7, 2020 as part of the 8th Annual Symposium on Pediatric Device Innovation, presented by Children’s National and co-located with The MedTech Conference powered by AdvaMed.



Invited commentary by Sarah Mulkey, M.D., Ph.D., prenatal-neonatal neurologist in the Division of Prenatal Pediatrics at Children’s National Hospital, emphasizes importance of studying the Zika population long term.
A simple measuring tape could be the key to identifying which children could develop neurological and developmental abnormalities from Zika virus exposure during gestation. This is according to an invited commentary published July 7, 2020 in JAMA Network Open and written by Sarah Mulkey, M.D., Ph.D., prenatal-neonatal neurologist in the Division of Prenatal Pediatrics at Children’s National Hospital.
Zika virus (ZIKV), first isolated in 1947 in the Zika Forest in Uganda, made headlines in 2015-2016 for causing a widespread epidemic that spread through parts of North and South America, several islands in the Pacific and parts of Southeast Asia. Although previously linked with no or mild symptoms, researchers discovered during this epidemic that Zika can cross from a pregnant woman to her gestating fetus, leading to a syndrome marked by microcephaly (decreased brain growth), abnormal neurologic tone, vision and hearing abnormalities and joint contractures.
“For the 90% to 95% of ZIKV-exposed infants who fortunately were not born with severe abnormalities at birth and were normocephalic, our hope was that these children would have normal neurodevelopmental outcomes,” Dr. Mulkey writes in the commentary. “Unfortunately, this has not been the case.”
Her commentary expands on a study in the same issue entitled “Association between exposure to antenatal Zika virus and anatomic and neurodevelopmental abnormalities in children” by Cranston et al. In this study, the researchers find that head circumference — a simple measure taken regularly at postnatal appointments in the U.S. — can provide insight into which children were most likely to develop neurologic abnormalities. Their findings show that 68% of those whose head circumference was in the “normal” range at birth developed neurologic problems. Those whose head circumference was at the upper end of this range were significantly less likely to have abnormalities than those at the lower end.
Just this single measurement offers considerable insight into the risk of developing neurologic problems after Zika exposure. However, notes Dr. Mulkey, head circumference growth trajectory is also key. Of the 162 infants whose heads were initially in the normocephalic range at birth, about 10.5% went on to develop microcephaly in the months after birth.
“Because early head growth trajectory is associated with cognitive outcomes in early childhood,” Dr. Mulkey writes, “following the head circumference percentile over time can enable recognition of a child with increased risk for poor outcome who could benefit from early intervention therapies.”
This simple assessment could be significantly augmented with neuroimaging, she adds. The study by Cranston et al., as well as others in the field, have shown that brain imaging often reveals problems in ZIKV-exposed children, such as calcifications and cerebral atrophy, even in those with normal head circumferences. This imaging doesn’t necessarily need to take place at birth, Dr. Mulkey says. Postnatal development of microcephaly, failure to thrive or developmental delay can all be triggers for imaging later on.
Together, Dr. Mulkey says, the study by Cranston et al. and others that focus on ZIKV-exposed children support the need for following these patients long term. Children exposed to ZIKV in the epidemic nearly five years ago are now approaching school age, a time fraught with more complicated cognitive and social demands. Through her own research at Children’s National’s Congenital Zika Virus Program and collaboration with colleagues in Colombia, Dr. Mulkey is following multiple cohorts of ZIKV exposed children as they grow. She recently published a study on neurological abnormalities in one of these cohorts in JAMA Pediatrics in January 2020.
“It’s really important to follow these children as long as possible so we’ll really know the outcomes of this virus,” Dr. Mulkey says.


Children’s National Hospital in Washington, D.C., was ranked No. 7 nationally in the U.S. News & World Report 2020-21 Best Children’s Hospitals annual rankings. This marks the fourth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide.
In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fourth year in a row.
For the tenth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“Our number one goal is to provide the best care possible to children. Being recognized by U.S. News as one of the best hospitals reflects the strength that comes from putting children and their families first, and we are truly honored,” says Kurt Newman, M.D., president and CEO of Children’s National Hospital.
“This year, the news is especially meaningful, because our teams — like those at hospitals across the country — faced enormous challenges and worked heroically through a global pandemic to deliver excellent care.”
“Even in the midst of a pandemic, children have healthcare needs ranging from routine vaccinations to life-saving surgery and chemotherapy,” said Ben Harder, managing editor and chief of Health Analysis at U.S. News. “The Best Children’s Hospitals rankings are designed to help parents find quality medical care for a sick child and inform families’ conversations with pediatricians.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
The other three specialties ranked among the top 50 were cardiology and heart surgery, gastroenterology and gastro-intestinal surgery, and urology.


New research, published in AIDS and Behavior, shows the effectiveness of an Advance Care Planning model developed through participatory research with adolescents in improving palliative care among adult people living with HIV (PLWH).
Since the beginning of the COVID-19 pandemic, there has been a dramatic increase in advance care planning (ACP) and the creation of advance directives, also known as living wills, in the United States. New research, published in AIDS and Behavior, shows the effectiveness of an ACP model developed through participatory research with adolescents in improving palliative care among adult people living with HIV (PLWH).
These findings demonstrate that ACP positively contributes to the palliative care of adult PLWH by relieving suffering and maximizing quality of life. The intervention was based on the FAmily CEntered (FACE) Advance Care Model, which was developed and tested by principal investigator Maureen E. Lyon, Ph.D., and her colleagues.
Dr. Lyon’s team used this model successfully with adolescents living with HIV as part of five-year, five-site trial that included Children’s National Hospital. The trial was co-funded by the National Institutes of Health and National Institute of Nursing Research. The success of that study was parlayed into a new five-year study testing a slightly modified ACP intervention in adults, with Children’s National serving as the coordinating center. “The adolescents showed us the way,” says Dr. Lyon.
The paper details the findings of a longitudinal, two arm, randomized controlled clinical trial examining whether an ACP intervention aimed at adult PLWH and their families correlated with higher congruence in treatment preferences, as well as higher congruence over time. Patient-surrogate dyads were randomized to an ACP intervention arm or an active control arm at a 2:1 ratio (86 intervention dyads and 43 control dyads at 18-month follow up), due to prior demonstrated benefit of ACP.
The ACP intervention consisted of two 60-minute, patient-focused sessions. During session 1, Respecting Choices Next Steps® ACP Conversation, both patients and their surrogate decision-makers focused on the patients’ understanding of HIV, experience of symptoms, fears, hopes and worries. Next, a patient’s treatment preferences were explored via the Statement of Treatment Preferences (SoTP), which became a part of the patient’s electronic health record (EHR). Surrogates were questioned on their comprehension and willingness to comply with the patient’s wishes. Session 1 was acknowledged as the beginning of a conversation, and continued conversation between the dyad was encouraged.
Session 2, Five Wishes©, involved a facilitator guiding the dyad through a Five Wishes© advance directive. Session 2 resulted in legal documentation of a patient’s preferences in five specific areas: The patient’s preferred health care decision-maker, the kind of medical treatment the patient wants, how comfortable the patient wants to be, how the patient wants people to treat him/her and what the patient wants loved ones to know. The patient, surrogate and treating physicians all received a copy, and a copy was also submitted to the patient’s EHR.
Dyads in the control arm participated in two 60-minute sessions entitled Developmental or Relationship History (excluding any medical questions) and Nutrition & Exercise.
The researchers then assessed treatment preference congruence for each patient-surrogate dyad by presenting them with five different hypothetical scenarios. After the first session, congruence across all scenarios was significantly higher among ACP intervention dyads compared to control dyads. ACP patients were also significantly more likely to give their surrogates leeway in treatment decision making compared to control patients.
Compared to control dyads, ACP dyads were significantly more likely to maintain High → High congruence transition and significantly less likely to experience Low → Low congruence transition as measured from immediately post-intervention to 12-months post-intervention. The only two cases of Low → High congruence transition occurred in the intervention arm. Of note, ACP surrogates accurately reported on changes in patient preferences over one year, showing the positive impact of early conversation on longitudinal congruence.
Dr. Lyon hopes these results will encourage people to talk to their loved ones as soon as possible about ACP, not only during the current pandemic but into the future. “People can use what’s happening in the news as a trigger to begin these conversations,” she says. “The 1990 Patient Self-Determination Act (PSDA) encourages persons of all ages– including children and their parents– to decide the type and extent of medical care they want to accept or refuse if they become unable to make those decisions due to illness. Our research shows conversations matter.”
The original research paper, “Effect of FAmily CEntered (FACE®)Advance Care Planning on Longitudinal Congruence in End-of-Life Treatment Preferences: A Randomized Clinical Trial,” was recently published in AIDS and Behavior. Dr. Maureen E. Lyon, Ph.D., FABPP, of the Center for Translational Research/Children’s Research Institute, was the principal investigator of the trial and a co-senior of the paper.


Matthew Oetgen, M.D., MBA, chief of orthopaedics and sports medicine at Children’s National Hospital, presented findings from a study aimed at improving quality and safety for pediatric spinal fusion procedures by reducing surgical site infection rates.
Pediatric orthopaedic surgery as a field is focused on improving quality and value in pediatric spine surgery, especially when it comes to eliminating surgical site infections (SSI). Many studies have documented how and why surgical site infections occur in pediatric spinal fusion patients, however, there is very little data about what approaches are most effective at reducing SSIs for these patients in a sustainable way.
At the Pediatric Orthopaedic Society of North America’s 2020 Annual Meeting, Matthew Oetgen, M.D., MBA, chief of orthopaedic surgery and sports medicine at Children’s National Hospital, presented findings from a long-term single institution study of acute SSI prevention measures.
“These findings give us specific insight into the tactics that are truly preventing, and in our case sometimes even eliminating, SSIs for pediatric scoliosis surgery,” says Dr. Oetgen, who also served on the annual meeting program committee. “By analyzing patient records across more than a decade, we were able to see that some strategies are quite effective, and others, that we thought would move the needle, just don’t.”
The team reviewed medical records and radiographs dating back to 2008 for 1,195 patients who had spinal fusion for scoliosis, including idiopathic scoliosis as well as other forms such as neuromuscular or syndromic scoliosis. Over that period of time, the division of orthopaedics and sports medicine at Children’s National was collaborating with the hospital’s infection control team to achieve several programmatic implementation milestones, including:
Over the study time period, the team found that SSIs did decrease, but interestingly, the rate did not progressively decrease with each subsequent intervention.
“Instead, we found that the rate went down and was even eliminated for some subgroups when the perioperative infection control protocols were implemented in 2013 and sustained through the study period end,” says Dr. Oetgen. “The other programmatic efforts that started in 2012 and 2015 had no impact on infection rates.”
He also notes that the study’s findings have identified a crucial component in the process for infection control in pediatric spinal surgery—perioperative protocols. “A relatively uncomplicated perioperative infection control protocol did the best job decreasing SSI in spinal fusion. Future efforts to optimize this particular protocol may help improve the rates even further.”


Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
You can view the entire Children’s National Research Institute academic annual report online.
Despite early reports suggesting COVID-19 does not seriously impact children, a new study shows that children who contract COVID-19 can become very ill.
In contrast to the prevailing view that the novel coronavirus known as COVID-19 does not seriously impact children, a new study finds that children who contract the virus can become very ill—many of them critically so, according to physician researchers at Children’s National Hospital. Their results, published in the Journal of Pediatrics and among the first reports from a U.S. institution caring for children and young adults, shows differences in the characteristics of children who recovered at home, were hospitalized, or who required life support measures. These findings highlight the spectrum of illness in children, and could help doctors and parents better predict which pediatric patients are more likely to become severely ill as a consequence of the virus.
In late 2019, researchers identified a new coronavirus, known as SARS-CoV-2, which causes COVID-19. As the disease spread around the world, the vast majority of reports suggested that elderly patients bear the vast majority of the disease burden and that children are at less risk for either infection or severe disease. However, study leader Roberta DeBiasi, M.D., M.S., chief of the Division of Infectious Diseases at Children’s National, states that she and her colleagues began noticing an influx of children coming to the hospital for evaluation of a range of symptoms starting in mid-March 2020, who were tested and determined to be infected with COVID-19. One quarter of these children required hospitalization or life support.
“It was very apparent to us within the first several weeks of the epidemic that this was a very different situation than our colleagues on the West Coast of the US had described as their experience just weeks before,” DeBiasi says. “Right away, we knew that it was important for us to not only care for these sick children, but to examine the factors causing severe disease, and warn others who provide medical care to children.”
To better understand this phenomenon, she and her colleagues examined the medical records of symptomatic children and young adults who sought treatment at Children’s National for COVID-19 between March 15 and April 30, 2020. Each of these 177 children tested positive using a rapid assay to detect SARS-CoV-2 performed at the hospital. The researchers gathered data on each patient, including demographic details such as age and sex; their symptoms; whether they had any underlying medical conditions; and whether these patients were non-hospitalized, hospitalized, or required critical care.
The results of their analysis show that there was about an even split of male and female patients who tested positive for COVID-19 at Children’s National during this time period. About 25% of these patients required hospitalization. Of those hospitalized, about 75% weren’t considered critically ill and about 25% required life support measures. These included supplemental oxygen delivered by intubation and mechanical ventilation, BiPAP, or high-flow nasal cannula – all treatments that support breathing – as well as other support measures such as dialysis, blood pressure support and medications to treat infection as well as inflammation.
Although patients who were hospitalized spanned the entire age range, more than half of them were either under a year old or more than 15 years old. The children and young adults over 15 years of age, Dr. DeBiasi explains, were more likely to require critical care.
About 39% of all COVID-19 patients had underlying medical conditions, including asthma, which has been highlighted as a risk factor for worse outcomes with this infection. However, DeBiasi says, although underlying conditions were more common as a whole in hospitalized patients – present in about two thirds of hospitalized and 80% of critically ill – asthma didn’t increase the risk of hospitalization or critical illness. On the other hand, children with underlying neurological conditions, such as cerebral palsy, microcephaly, or global developmental delay, as well as those with underlying cardiac, hematologic, or oncologic conditions were significantly more likely to require hospitalization.
In addition, although early reports of COVID-19 suggested that fever and respiratory symptoms are hallmarks of this infection, Dr. DeBiasi and her colleagues found that fewer than half of patients had both concurrently. Those with mild, upper respiratory symptoms, such as runny nose, congestion, and cough were less likely to end up hospitalized than those with more severe respiratory symptoms, such as shortness of breath. The frequency of other symptoms including diarrhea, chest pain and loss of sense of smell or taste was similar among hospitalized and non-hospitalized patients.
Dr. DeBiasi notes that although other East Coast hospitals are anecdotally reporting similar upticks in pediatric COVID-19 patients who become seriously ill, it’s currently unclear what factors might account for differences from the less frequent and milder pediatric illness on the West Coast. Some factors might include a higher East Coast population density, differences between the genetic, racial and ethnic makeup of the two populations, or differences between the viral strains circulating in both regions (an Asian strain on the West Coast, and a European strain on the East Coast).
Regardless, she says, the good news is that the more researchers learn about this viral illness, the better prepared parents, medical personnel and hospitals will be to deal with this ongoing threat.
Other researchers from Children’s National who participated in this study include Xiaoyan Song, Ph.D., M.Sc., Meghan Delaney, D.O., M.P.H., Michael Bell, M.D. , Karen Smith, M.D., Jay Pershad, M.D., Emily Ansusinha, Andrea Hahn, M.D., M.S., Rana Hamdy, M.D., M.P.H., MSCE, Nada Harik, M.D., Benjamin Hanisch, M.D., Barbara Jantausch, M.D., Adeline Koay, MBBS, MS.c., Robin Steinhorn, Kurt Newman, M.D. and David Wessel, M.D.


Telehealth is more than a doctor-to-patient tool during COVID-19. Experts in congenital heart disease meet weekly to share details about how it affects their vulnerable patients.
During the COVID-19 pandemic, telehealth has been crucial in allowing doctors to maintain safe contact with patients who require ongoing medical care without an office visit. Just as important is the role that telehealth is playing to connect care providers with each other to ensure that everyone around the world has the information they need to provide the best care possible for this swift-moving disease.
One good example of this specialist-to-specialist thought leadership connection is the ongoing weekly meeting hosted by the Children’s National Hospital cardiac critical care specialists. Since early in the spread of COVID-19, the Cardiac-ICU team, led by cardiovascular specialists including Ricardo Munoz, M.D., chief of cardiac critical care medicine and executive director of telehealth at Children’s National, have connected pediatric clinicians around the world to discuss how best to care for particularly vulnerable patients with pre-existing heart diseases, and to discuss breaking news in epidemiology of the disease and the effectiveness of various treatment approaches.
The video conference attracts hundreds of physicians and nurses who specialize in pediatric cardiac care from countries all over the world. In the last week of April, the meeting featured a late-breaking session to discuss new pediatric intensive care observations of inflammatory symptoms similar to Kawasaki disease, which were being detected in the United Kingdom, Paris and the United States. While more information is needed about this discovery, the ability of these experts to gather and compare disease phenotypes from country to country facilitates both the additional classification of pediatric-related symptoms and improves how all centers, no matter their location, can prepare to treat children who present locally with these symptoms.
In recent weeks, cardiac physicians and nurses from some of the world’s hardest hit regions, including Italy and Spain, have shared detailed information about their on-the-ground experiences to help colleagues in the U.S. and elsewhere better prepare for new developments.
“This new disease is a moving target, especially when it comes to understanding how it might impact children and adults with existing cardiac disease, particularly those with congenital heart disease,” says Dr. Munoz. “It is extremely important that we learn from each other, especially when we are able to connect with our colleagues in the epicenters of the most serious outbreaks of COVID-19. We are happy to host this important weekly meeting with the goal of helping every specialist keep as many patients with cardiac diseases as safe as possible throughout the global health emergency.”
If you would like to join these weekly telehealth meetings, please send your request to COVIDMultiCICUResponse@childrensnational.org.
The International Consortium for Health Outcomes Measurement (ICHOM) announced the release of a Congenital Heart Disease Standard Set (CHDSS) in late April 2020.
Gerard Martin, M.D., FAAP, FACC, FAHA, cardiologist at Children’s National Hospital, chaired the working group and contributed to the standards’ writing. In ICHOM‘s press release, he noted that, “Having a global set of outcomes that matters most to adult patients and parents of children with congenital heart disease will provide a road map for healthcare professionals and organizations engaged in setting care strategies for this population around the world. I would like to acknowledge the efforts of the Working Group and ICHOM staff for their incredible effort on this project.”
The CHDSS is a minimum core set of standards, comprised of Patient, Parent, and Clinician – Reported Outcome Measures already being collected by most practices in routine clinical care. The CHDSS measures 14 outcomes under the ICHOM framework for comprehensive outcomes measurement. These overarching domains are Overall Health, Social Health, Mental Health, and Physical Health.
Learn more about the CDHSS, the contributors and read the ICHOM press release.

The CHDSS measures 14 outcomes under the ICHOM overarching domains of Overall Health, Social Health, Mental Health, and Physical Health.


Young people with the co-occurrence of autism and gender diversity and their families partner with clinical researchers to understand care needs and how care providers can meet those needs.
The first ever set of specific recommendations to support transgender autistic young people was co-created by these youth and their families working hand-in-hand with clinical experts. The resulting model offers clinicians a set of concrete ways to provide this unique population the support they need.
The recommendations, A Clinical Program for Transgender and Gender-Diverse Neurodiverse/Autistic Adolescents Developed through Community-Based Participatory Design, were published by the Journal of Clinical Child and Adolescent Psychology on May 4, 2020.
“The idea of patients helping to co-design their own care isn’t new, but including the perspectives of autistic youth in their own care is quite new,” says John Strang, Psy.D., who directs the Gender and Autism Program within the Center for Autism Spectrum Disorders at Children’s National Hospital.
He continues, “And for the many youth who are both transgender and autistic, including their voices and perspectives in their clinical care is critical. Without their input, there is a great risk for misunderstanding their needs – and for marginalization.”
“This was an important process in which to participate, and will hopefully help those — autistic people, trans people, and autistic trans people alike — who often only see themselves represented by cisgender, neurotypical researchers and providers. It is a relief to be a part of creating something like this,” adds Marisa Alexa McCool, a co-researcher who is an autistic transgender woman.
The new publication builds on previously published broad clinical guidelines for providers, now integrating the perspectives of autistic transgender individuals themselves. The program includes specific approaches for supporting young people in their diverse needs, and identifies three key components central to this care:
The perspectives included in the new clinical program were from a range of ages and backgrounds, as well as across multiple points in time to make sure that as youths’ own views evolved, their evolving needs were captured as well.
The authors created a specific clinical guide to complement the publication, which is available on the Children’s National website.
“We’re so happy to have been able to partner with self-advocates from the autistic transgender and gender diverse communities, youth who are living this experience, and their families, to co-create a community-driven model that can be used for kids seeking guidance and support,” says Dr. Strang.
“We hear over and over again that what parents and care providers really need are concrete tools to support young people with co-occurring autism and gender diversity, so that’s what we sought to do here,” he concludes. “It’s exciting because, for the first time, we have some simple tools to support these kids. And this is critical, because although the co-occurrence of autism and gender diversity has been of great interest to researchers, nearly all studies to date have focused on how many transgender youth are autistic, instead of how to help and support this poorly understood group.”


Patients and staff at the Uganda Heart Institute for RHD-related heart surgeries in Uganda, March 2020. These patients were originally scheduled as part of the cancelled medical mission, but UHI cardiovascular surgeon successfully managed these cases without the support of the mission doctors from the U.S.
In early March as countries around the globe began to wrestle with how best to tackle the spread of COVID-19, a group of doctors, nurses, researchers and other medical staff from Children’s National Hospital were wrestling with a distinct set of challenges: What to do about the 10 Ugandan children and adults who were currently scheduled for lifesaving heart surgery (and the countless others who would benefit from the continued training of the local heart surgery team) to correct complications of rheumatic heart disease (RHD) during an impending medical mission in the country.
Rheumatic heart disease impacts over 39 million people globally and causes nearly 300,000 deaths per year. RHD is the result of frequent, untreated streptococcal throat infections in childhood that ultimately cause the body’s immune system to repeatedly damage heart valves. It is completely preventable, yet the majority of the world’s children still live in impoverished and overcrowded conditions that predispose them to RHD. Most patients present with advanced valvular heart disease. For example, in Uganda, an RHD registry includes over 600 children with clinical RHD, of which nearly 40% die within four years and the median survival time from enrollment in the registry is only nine months. For these patients, heart surgery is the only viable solution for long-term survival and normal quality of life.

Patricia: 9-year-old from Gulu (northern Uganda), had mitral valve replacement and was doing well on a recent follow-up visit at her home.
The scheduled trip from Washington was part of a nearly 20-year partnership** between doctors, nurses, researchers and other medical staff in the United States, including Craig Sable, M.D., associate chief of cardiology, and and Pranava Sinha, M.D.,pediatric cardiovascular surgeon, at Children’s National Hospital in Washington, D.C., and the Uganda Heart Institute in Kampala, Uganda. The partnership aims to tackle RHD head-on. It provides surgical skill transfer, allows for treatment of more complex patients, and increases sustainable surgical capacity for Uganda’s RHD patients over time. As a result, over the last 15 years more than 1,000 children have received lifesaving heart surgery in Uganda, with the Uganda Heart Institute (UHI) performing one to two heart valve surgeries every two weeks over the last few years.

Jackline: 12-year-old from Gulu, had mitral valve repair and aortic valve replacement. Jackline and Patricia were diagnosed through one of our research programs and benefit from our novel telehealth program, which helps connect patients from remote parts of Uganda to specialists at UHI.
COVID-19 was changing the current plan, however. Travel between countries was limited, and the team from the U.S. wouldn’t have been permitted to leave the U.S. and return according to schedule. The trip, and the support teams who were scheduled to arrive to help with the surgeries, were cancelled. The U.S. team members who had already arrived in Uganda were sent home after helping their UHI colleagues set up and prepare for the surgeries as much as possible. Knowing that patients and families were counting on the surgery mission to go forward after waiting for months or years to have surgery for heart valve disease, UHI decided not to cancel the majority of the surgeries. Instead, for the first time, they planned and successfully completed five valve-related cases in a single week – several of them quite complex. The cardiologists and cardiac surgeons from Children’s National who were supposed to be in-country for these procedures were forced to limit their in person assistance to the set-up activities the week prior to surgery and telehealth consult during the procedures.
“It was hard not to be able to stay and work with the UHI team to help these families,” says Dr. Sable. “But we are so proud of the UHI team for meeting this challenge on their own. We knew they had the skills to perform at this volume and complexity. It’s a proud moment to see the team accomplish this major milestone, and to see the patients they cared for thrive.”
The patients are the most important outcome: The five who had successful open-heart surgery are all doing well, either on their way to recovery or already discharged to their communities, where they will, for the first time in memory, be able to play, exercise and go to school or work.
Longer term, this success demonstrates the UHI medical team’s ability to manage greater surgical capacity even when surgical missions from the U.S. resume. The partnership’s goal is to complete at least 1,000 annual operations (both pediatric and adult), with the majority being performed by the local team. Having this capacity available will mean the difference between life and death for many children and adults who have RHD in Uganda and the surrounding countries.
**This work is supported by the Edwards Life Sciences/Thoracic Surgery Foundation, the Emirates Airline Foundation, Samaritan’s Purse Children’s Heart Project and Gift of Life International.


Run at the state-level, mandatory newborn screening (NBS) programs detect a host of hereditary disorders so that infants can be treated before further damage, or even death, occurs.
Newborn screening (NBS) programs are critical to public health. Run at the state-level, mandatory NBS programs detect a host of hereditary disorders so that infants can be treated before further damage, or even death, occurs.
While much attention is paid to testing technology, programs must still meet basic minimum requirements to reliably identify and treat all affected individuals including minimum reporting requirements, case surveillance and a dedicated short-term follow-up program. In newborn screening, success is systematic.
A new report “How a baby with classic galactosemia was nearly missed: When the test succeeds but system fails,” published in the American Journal of Medical Genetics, takes a look at an individual case that almost slipped through the cracks of a local NBS program.
One disorder detected by NBS is classic galactosemia (CG), which arises from a deficiency in the galactose-1-phosphate uridyltransferase (GALT) enzyme, leaving infants unable to metabolize galactose-1-phosophate, a monosaccharide abundantly present in milk. CG can result in fatal liver failure, sepsis and coagulopathy if the affected infant is not switched to soy-based formula within the first week of life.
CG can be detected through a combination of enzyme assay, DNA analysis and galactose quantification. However, NBS programs differ in testing protocols for CG by state, and not all NBS programs conduct all of these tests. This is of particular relevance to the Washington, D.C., metropolitan area, a regional nexus where crossing state and district lines for medical care is common.
The report describes how a D.C.-born infant was screened for CG through all three tests. While his galactose levels were normal, his GALT was low and DNA testing revealed homozygosity for a CG mutation known as K285N. In tandem, the latter two indicators constitute a true positive result for CG, and necessitate the proper issuance of referrals, precautions and follow-up, which failed to occur in this case.
The infant breastfed and displayed notable lethargy, and parents were directed to a local emergency department in a neighboring state which does not screen for CG with DNA testing.
The providers there were unfamiliar with the DNA results, and after new labs came back normal, the NBS results were deemed as “likely falsely positive” for CG. Fortunately, a provider at the community hospital forwarded the NBS results to the Children’s National Rare Disease Institute (CNRDI). Upon review, CNRDI metabolic specialists immediately sought to rectify the situation by reaching out to the family with proper instructions and arranging a clinical evaluation, which occurred 10 days after birth.
While this case had a fortunate ending, the report highlights the potential deficiencies in NBS programs, which have historically been among America’s most successful public health initiatives. The proper and timely functioning of NBS systems is contingent upon the functioning of its constituent parts, including testing, diagnosis, follow-up, management and stakeholder education.
While test results were accurate in this case, systemic shortcomings left a patient in danger. As the authors state, “Programs must keep in mind that the true success of newborn screening extends beyond just the test itself…to improve safety and care outcomes we must focus on the system.”
A clinical report by a team of authors, mainly comprised of Children’s National clinicians, was published earlier this month in the American Journal of Medical Genetics. Authors include Sarah Viall, PPCNP, MSN, a pediatric nurse practitioner in the Rare Disease Institute; Nicholas Ah Mew, M.D., director of the Inherited Metabolic Disorders Program; and Beth A. Tarini, M.D., M.S., associate director of the Center for Translational Research.
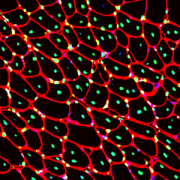
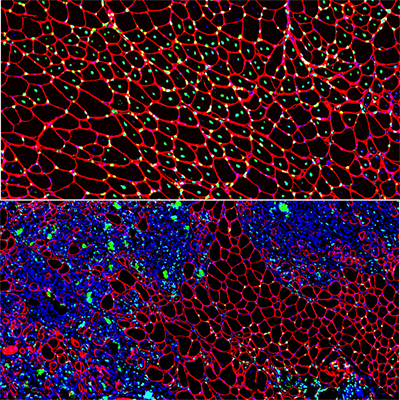
Muscle regeneration marked by incorporation of muscle stem cell nuclei (green) in the myofibers (red) in dystrophic muscles with low TGFβ level (upper image), but not with high TGFβ level (lower image). Inflammatory and other nuclei are labeled blue.
Boys with Duchenne muscular dystrophy (DMD) experience poor muscle regeneration, but the precise reasons for this remain under investigation. An experimental model of severe DMD that experiences a large spike in transforming growth factor-beta (TGFβ) activity after muscle injury shows that high TGFβ activity suppresses muscle regeneration and promotes fibroadipogenic progenitors (FAPs). This leads to replacement of the damaged muscle fibers by calcified and connective tissue, compromising muscle structure and function. While blocking FAP buildup provides a partial solution, a Children’s National Hospital study team identifies correcting the muscle micro-environment caused by high TGFβ as a ripe therapeutic target.
The team’s study was published online March 26, 2020, in JCI Insight.
DMD is a chronic muscle disease that affects 1 in 6,200 young men in the prime of their lives. The disorder, caused by genetic mutations leading to the inability to produce dystrophin protein, leads to ongoing muscle damage, chronic inflammation and poor regeneration of lost muscle tissue. The patients experience progressive muscle wasting, lose the ability to walk by the time they’re teenagers and die prematurely due to cardiorespiratory failure.
The Children’s National team finds for the first time that as early as preadolescence (3 to 4 weeks of age), their experimental model of severe DMD disease showed clear signs of the type of spontaneous muscle damage, regenerative failure and muscle fiber loss seen in preadolescent boys who have DMD.
“In boys, the challenge due to muscle loss exists from early in their lives, but had not been mimicked previously in experimental models,” says Jyoti K. Jaiswal, MSc, Ph.D., principal investigator in the Center for Genetic Medicine Research at Children’s National, and the study’s co-senior author. “TGFβ is widely associated with muscle fibrosis in DMD, when, in fact, our work shows its role in this disease process is far more significant.”
Research teams have searched for experimental models that replicate the sudden onset of symptoms in boys who have DMD as well as its complex progression.
“Our work not only offers insight into the delicate balance needed for regeneration of skeletal muscle, but it also provides quantitative information about muscle stem cell activity when this balanced is disturbed,” says Terence A. Partridge, Ph.D., principal investigator in the Center for Genetic Medicine Research at Children’s National, and the study’s co-senior author.
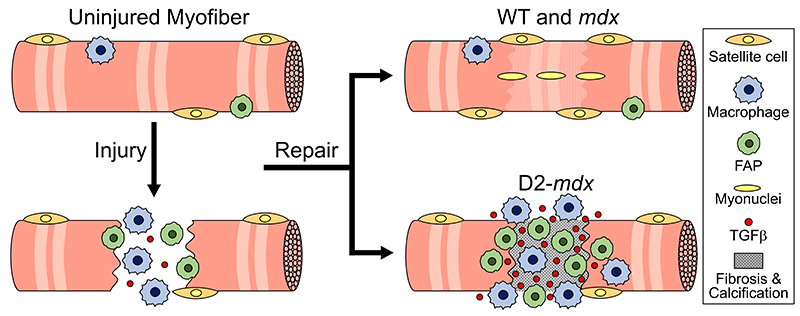
This schematic depicts the fate of injured myofibers in healthy or dystrophic muscle (WT or mdx experimental models) that maintain low TGFβ level, compared with D2-mdx experimental models that experience a large increase in TGFβ level. As the legend shows, various cells are involved in this regenerative response.
“The D2-mdx experimental model is a relevant one to use to investigate the interplay between inflammation and muscle degeneration that is seen in humans with DMD,” adds Davi A.G. Mázala, co-lead study author. “This model faithfully recapitulates many features of the complex disease process seen in humans.”
Between 3 to 4 weeks of age in the experimental models of severe DMD disease, the level of active TGFβ spiked up to 10-fold compared with models with milder disease. Intramuscular injections of an off-the-shelf drug that inhibits TGFβ signaling tamped down the number of FAPs, improving the muscle environment by lowering TGFβ activity.
“This work lays the foundation for studies that could lead to future therapeutic strategies to improve patients’ outcomes and lessen disease severity,” says James S. Novak, Ph.D., principal investigator in Children’s Center for Genetic Medicine Research, and co-lead study author. “Ultimately, our goal is to improve the ability of patients to continue to maintain muscle mass and regenerate muscle.”
In addition to Mázala, Novak, Jaiswal and Partridge, Children’s National study co-authors include Marshall W. Hogarth; Marie Nearing; Prabhat Adusumalli; Christopher B. Tully; Nayab F. Habib; Heather Gordish-Dressman, M.D.; and Yi-Wen Chen, Ph.D.
Financial support for the research described in this post was provided by the National Institutes of Health under award Nos. T32AR056993, R01AR055686 and U54HD090257; Foundation to Eradicate Duchenne; Muscular Dystrophy Association under award Nos. MDA295203, MDA480160 and MDA 477331; Parent Project Muscular Dystrophy; and Duchenne Parent Project – Netherlands.


Investigators from around the world penned manuscripts that were assembled in a special issue of “Neurochemical Research” that honors Vittorio Gallo, Ph.D., for his leadership in the field of neural development and regeneration.
At a pivotal moment early in his career, Vittorio Gallo, Ph.D., was accepted to work with Professor Giulio Levi at the Institute for Cell Biology in Rome, a position that leveraged courses Gallo had taken in neurobiology and neurochemistry, and allowed him to work in the top research institute in Italy directed by the Nobel laureate, Professor Rita Levi-Montalcini.
For four years as a student and later as Levi’s collaborator, Gallo focused on amino acid neurotransmitters in the brain and mechanisms of glutamate and GABA release from nerve terminals. Those early years cemented a research focus on glutamate neurotransmission that would lead to a number of pivotal publications and research collaborations that have spanned decades.
Now, investigators from around the world who have worked most closely with Gallo penned tributes in the form of manuscripts that were assembled in a special issue of “Neurochemical Research” that honors Gallo “for his contributions to our understanding of glutamatergic and GABAergic transmission during brain development and to his leadership in the field of neural development and regeneration,” writes guest editor Arne Schousboe, of the University of Copenhagen in Denmark.

Vittorio Gallo, Ph.D. as a 21-year-old mustachioed graduate student.
“In spite of news headlines about competition in research and many of the negative things we hear about the research world, this shows that research is also able to create a community around us,” says Gallo, chief research officer at Children’s National Hospital and scientific director for the Children’s National Research Institute.
As just one example, he first met Schousboe 44 years ago when Gallo was a 21-year-old mustachioed graduate student.
“Research can really create a sense of community that we carry on from the time we are in training, nurture as we meet our colleagues at periodic conferences, and continue up to the present. Creating community is bi-directional: influencing people and being influenced by people. People were willing to contribute these 17 articles because they value me,” Gallo says. “This is a lot of work for the editor and the people who prepared papers for this special issue.”
In addition to Gallo publishing more than 140 peer-reviewed papers, 30 review articles and book chapters, Schousboe notes a number of Gallo’s accomplishments, including:
Purkinje cells are large neurons located in the cerebellum that are elaborately branched like interlocking tree limbs and represent the only source of output for the entire cerebellar cortex.
Even the image selected to grace the special issue’s cover continues the theme of continuity and leaving behind a legacy. That image of Purkinje cells was created by a young scientist who works in Gallo’s lab, Aaron Sathyanesan, Ph.D. Gallo began his career working on the cerebellum – a region of the brain important for motor control – and now studies with a team of scientists and clinician-scientists Purkinje cells’ role in locomotor adaptive behavior and how that is disrupted after neonatal brain injury.
“These cells are the main players in cerebellar circuitry,” Gallo says. “It’s a meaningful image because goes back to my roots as a graduate student and is also an image that someone produced in my lab early in his career. It’s very meaningful to me that Aaron agreed to provide this image for the cover of the special issue.”
