Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
For the fifteenth straight year, Children’s National ranked in 10 specialty services and is the highest U.S. News ranked children’s hospital in Washington, D.C., Maryland and Virginia. Last year, U.S. News introduced pediatric & adolescent behavioral health as a service line in its rankings. While there are no ordinal rankings for behavioral health, the Children’s National program was named one of the top 50 programs in the country for the second year in a row.
“To be named among the nation’s top children’s hospitals for nine years in a row is a reflection of the extraordinary expertise, innovation and heart that our teams bring to every child and family we serve,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “Our leadership in specialties like neurology, cancer, and diabetes and endocrinology underscores the national impact of our work, and we remain focused on setting new standards in pediatric care.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“Being a top-ranked pediatric hospital means more than just excelling in a single specialty — it means being a pillar of outstanding care for your entire region,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Our rankings acknowledge these hospitals for their comprehensive excellence, helping families find the very best care conveniently located within their state and community.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/10/USNWR_CNBadges_Set2SideBySide_2025-26-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-10-07 01:00:072025-10-07 09:08:32Children’s National Hospital once again ranked among the nation’s best by U.S. News & World Report
Dr. Levitt mentoring surgeons from 14 African countries on a complex colorectal operation.
At the 14th Congress of the Pan-African Pediatric Surgery Association (PAPSA) in Abidjan, Côte d’Ivoire, Marc Levitt, MD, chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital, was invited to deliver one of the primary courses, a rare honor reserved for leaders in the field. Held only once every 2 years, the PAPSA meeting draws more than 300 pediatric surgeons from across Africa, making it the continent’s most significant gathering dedicated to pediatric surgery. Dr. Levitt’s role in the event highlights both his global expertise and the ongoing commitment of Children’s National to advancing pediatric surgical care and education in low- and middle-income countries.
Just prior to the congress, Dr. Levitt and his organization, Colorectal Team Overseas, led an international team of surgeons in partnership with the local surgical team to care for 17 children from Côte d’Ivoire and several neighboring countries with complex colorectal conditions. These conditions included anorectal malformations, cloaca and Hirschsprung’s disease, which can severely affect quality of life if untreated. Founded by Dr. Levitt, Colorectal Team Overseas advances global pediatric surgical care through education and hands-on training, extending the expertise of Children’s National to children around the world. Joining him on the mission were colorectal surgeon Andrea Badillo, MD, and surgical technician Guy Ozigre, both from Children’s National. The course also welcomed pediatric surgeons from 14 African nations, promoting collaboration and skill-building.
A busy clinic in preparation of the operating room days.
Among the many teaching highlights was the first-ever perineal body preserving posterior sagittal anorectoplasty performed in Western Africa, a technique pioneered at Children’s National. “These are life-changing procedures, and it was a privilege to perform them with such dedicated teams, who were so eager to learn,” said Dr. Levitt. “The hospital’s facilities were excellent, and the professionalism and warmth of the Ivorian teams made this an unforgettable experience.”
The workshops and surgeries, hosted at the Mother-Child Hospital Dominique Ouattara in Bingerville, reflected PAPSA’s core mission: to treat, train and transmit. With pediatric surgical needs continuing to outpace available expertise in many African countries, initiatives like this one are vital to training local specialists and developing sustainable care, according to the host and chief of pediatric surgery, Rouma Bankole, MD.
“Sharing knowledge and training the next generation of pediatric surgeons is the key to improving outcomes globally,” said Dr. Levitt.
Dr. Levitt and Colorectal Team Overseas with the local surgeons from Cote D’Ivoire
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/07/Colorectal-Team-Feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-07-10 12:37:582025-07-10 12:38:28Advancing global surgical care: Children’s National colorectal team at PAPSA 2025
Members of the Division of Colorectal & Pelvic Reconstruction at Children’s National Hospital recently traveled to Sao Paulo, Brazil, with the goal of advancing surgical care for children with complex colorectal conditions. Led by Division Chief Marc Levitt, MD, the team collaborated closely with surgeons and nurses at Hospital Municipal Infantil Menino Jesus, performing multiple intricate procedures each day and giving a course to 120+ surgeons from all over Brazil and several surrounding countries. The operations performed and the education that was provided not only gave life-changing care to children in need but also served as critical teaching opportunities, equipping local surgical teams with the skills and knowledge to deliver specialized care in their own communities. In this way, the team from Children’s National is helping countless children they will never meet, as their new partners in Brazil now have the skills to care for them
This mission was organized through Colorectal Team Overseas, an organization founded and led by Dr. Levitt to advance global pediatric surgical care through education and hands-on training. Colorectal Team Overseas gives Dr. Levitt the opportunity to extend the world-class care delivered at Children’s National to children around the world.
“Every child deserves a chance at a healthy, dignified life, no matter where they are born,” says Dr. Levitt. “On these missions, doctors, nurses and volunteers from the colorectal program at Children’s National and colleagues from around the world work hand-in-hand with medical teams in Brazil — not only to provide surgical care, but to teach, learn and build a foundation for a lasting impact. We are not just performing surgeries; we are restoring futures, together.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/05/CTO-in-Brazil-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-05-16 14:17:542025-05-16 14:22:30Colorectal care across borders: expanding access through global collaboration
Children’s National Hospital hosted its fifteenth annual Research, Education and Innovation Week from March 31–April 4, 2025, bringing together clinicians, scientists, educators and innovators from across the institution to celebrate discovery and collaboration. This year’s theme, “Empowering the Future in Pediatric Research and Innovation with Equity, Technology and a Global Reach,” served as a call to action for advancing science that improves child health both locally and around the world.
Each day of the week-long event featured thought-provoking lectures — now available to watch — dynamic panel discussions, interactive workshops and vibrant poster sessions, all highlighting the diverse and interdisciplinary work taking place across Children’s National.
Centering the patient and the planet
REI Week began on Monday with a powerful keynote lecture from Lynn R. Goldman, MD, MS, MPH, Michael and Lori Milken dean of the Milken Institute School of Public Health at the George Washington University. In her talk, “Children: Uniquely vulnerable to climate-related threats,” Dr. Goldman underscored the urgent need to protect children from the environmental hazards of a changing climate and to integrate climate science into pediatric care and advocacy.
At mid-morning, Mary-Anne “Annie” Hartley, MD, PhD, MPH, director of the LiGHT Laboratory at École Polytechnique Fédérale de Lausanne, introduced the “MOOVE” platform — Massive Open Online Validation and Evaluation of clinical LLMs. Her talk demonstrated how artificial intelligence, when rigorously validated, has the potential to transform clinical decision-making and global health equity.
Monday’s final keynote, “Zinc and childhood diarrhea,” was presented by Christopher Duggan, MD, MPH, director of the Division of Nutrition at Harvard Medical School. Dr. Duggan highlighted the global health impact of zinc supplementation in reducing childhood mortality — a reminder that simple, evidence-based interventions can save millions of lives.
In that first day, the first poster session of the week showcased projects in adolescent medicine, global health, infectious diseases, oncology and more. The session reflected the full breadth of research taking place across Children’s National.
Ambroise Wonkam, MD, PhD, professor of genetic medicine at Johns Hopkins University, then delivered Tuesday’s Global Health Keynote Lecture, “Harnessing our common African genomes to improve health and equity globally.” His work affirmed that inclusive genomics is key to building a healthier world.
Later, the Global Health Initiative event and GCAF Faculty Seminar encouraged attendees to pursue collaborative opportunities at home and abroad, reflecting the growing global footprint of Children’s National research programs.
Transforming education and care delivery
On Wednesday, Larrie Greenberg, MD, professor emeritus of pediatrics, kicked off the day with a Grand Rounds keynote on educational transformation: “Shouldn’t teachers be more collaborative with their learners?” He followed with a CAPE workshop exploring the effectiveness of case-based learning.
In the Jill Joseph Grand Rounds Lecture, Deena J. Chisolm, PhD, director of the Center for Child Health Equity at Nationwide Children’s Hospital, challenged attendees to move beyond dialogue into action in her talk, “Health equity: A scream to a whisper?,” reminding researchers and clinicians that advocacy and equity must be foundational to care.
The day continued with a poster session spotlighting medical education, neonatology, urology and neuroscience, among other fields.
Posters and pathways to progress
Throughout the week, poster sessions highlighted cutting-edge work across dozens of pediatric disciplines. These sessions gave attendees the opportunity to engage directly with investigators and reflect on the shared mission of discovery across multiple disciplines, including:
The REI Week 2025 Awards Ceremony celebrated outstanding contributions in research, mentorship, education and innovation. The winners in each category were:
POSTER SESSION AWARDS
Basic & Translational Research
Faculty: Benjamin Liu, PhD
“Genetic Conservation and Diversity of SARS-CoV-2 Envelope Gene Across Variants of Concern”
Faculty: Steve Hui, PhD
“Brain Metabolites in Neonates of Mothers with COVID-19 Infection During Pregnancy”
Faculty: Raj Shekhar, PhD
“StrepApp: Deep Learning-Based Identification of Group A Streptococcal (GAS) Pharyngitis”
Post docs/Fellows/Residents: Dae-young Kim, PhD
“mhGPT: A Lightweight Domain-Specific Language Model for Mental Health Analysis”
Post docs/Fellows/Residents: Leandros Boukas, MD, PhD
“De Novo Variant Identification From Duo Long-Read Sequencing: Improving Equitable Variant Interpretation for Diverse Family Structures”
Staff: Naseem Maghzian
“Adoptive T Lymphocyte Administration for Chronic Norovirus Treatment in Immunocompromised Hosts (ATLANTIC)”
Graduate Students: Abigail Haffey
“Synergistic Integration of TCR and CAR T Cell Platforms for Enhanced Adoptive Immunotherapy in Brain Tumors”
High School/Undergraduate Students: Medha Pappula
“An ADHD Diagnostic Interface Based on EEG Spectrograms and Deep Learning Techniques”
Clinical Research
Faculty: Folasade Ogunlesi, MD
“Poor Air Quality in Sub-Saharan Africa is Associated with Increase Health Care Utilization for Pain in Sickle Cell Disease Patients”
Faculty: Ayman Saleh, MD
“Growth Parameters and Treatment Approaches in Pediatric ADHD: Examining Differences Across Race”
Post docs/Fellows/Residents: Nicholas Dimenstein, MD, MPH
“Pre-Exposure Prophylaxis (PrEP) Eligibility in the Pediatric Emergency Department”
Staff: Tayla Smith, MPH
“The Public Health Impact of State-Level Abortion and Firearm Laws on Health Outcomes”
Graduate Students: Natalie Ewing
“Patterns of Bacteriuria and Antimicrobial Resistance in Patients Presenting for Primary Cloacal Repair: Is Assisted Bladder Emptying Associated with Bacteriuria?”
Graduate Students: Manuela Iglesias, MS
“Exploring the Relationship Between Child Opportunity Index and Bayley-III Scores in Young Children”
High School/Undergraduate Students: Nicholas Lohman
“Preliminary Findings: The Efficacy, Feasibility and Acceptability of Group Videoconference Cognitive Behavioral Therapy with Exposure and Response Prevention for Treating Obsessive-Compulsive Disorder Among Children and Young People”
Community-Based Research
Faculty: Sharon Shih, PhD “Assessing Pediatric Behavioral Health Access in DC using Secret Shopper Methodology”
Post docs/Fellows/Residents: Georgios Sanidas, MD “Arrested Neuronal Maturation and Development in the Cerebellum of Preterm Infants”
Staff: Sanam Parwani
“Intersectionality of Gender and Sexuality Diversity in Autistic and Non-Autistic Individuals”
Graduate Student: Margaret Dearey “Assessing the Burden of Period Poverty for Youth and Adolescents in Washington, DC: A Pilot Study”
Quality and Performance Improvement
Faculty: Nichole L. McCollum, MD
“A Quality Improvement Study to Increase Nurse Initiated Care from Triage and Improve Timeliness to Care”
Post docs/Fellows/Residents: Hannah Rodriguez, MD
“Reducing Unnecessary Antibiotic Use in a Level IV NICU”
Staff: Amber K. Shojaie, OTD, OTR/L
“Implementing Dynamic Axilla Splints in a Large Burn Patient”
Meleah Boyle, PhD, MPH
“Understanding and Addressing Environmental Sustainability to Protect the Health of the Children’s National and Global Communities”
Eiman Abdulrahman, MD
“Research Capacity Building to Improve Pediatric Emergency and Critical Care in Ethiopia”
Pilot Awards
Alexander Andrews, MD
“EEG as a Diagnostic and Prognostic Marker in Severe Pediatric Malaria, Blantyre Malawi”
Daniel Donoho, MD & Timothy Singer, MD
“Feasibility Study of a Novel Artificial Intelligence-Based Educational Platform to Improve Neurosurgical Operative Skills in Tanzania”
Hasan Syed, MD
“Bridging the Gap an Educational Needs Assessment for Pediatric Neurosurgery Training in Pakistan”
Sofia Perazzo, MD & Lamia Soghier, MD, MEd, MBA
“QI Mentorship to Improve Pediatric Screening and Follow-up in Rural Argentina”
Benjamin Liu, PhD
“AI-Empowered Real-Time Sequencing Assay for Rapid Detection of Schistosomiasis in Senegal”
Rae Mittal, MD
“Assessment and Enhancement of Proficiency in Emergency Child Neurology Topics for Post-Graduate Emergency Medicine Trainees in India”
Innovation Day ignites bold thinking
Thursday, REI Week shifted to the Children’s National Research & Innovation Campus for Innovation Day, a celebration of how bold ideas and collaborative culture can accelerate progress in pediatric medicine.
REI Week 2025 reaffirmed the values that define Children’s National: a commitment to excellence, collaboration and equity in pediatric research and care. As discoveries continue to emerge from our hospital and our research campuses, the connections built and ideas sparked during this week will help shape the future of pediatric health — locally and globally.
By elevating voices from the bedside to the bench, with the support of the executive sponsors Nathan Kuppermann, MD, MBChB, Catherine Bollard, MBChB, MD, Kerstin Hildebrandt, MSHS, Linda Talley, MS, RN, NE-BC and David Wessel, MD, REI Week demonstrated that we must embrace the community in all aspects of our work. Because we know that there are answers we can only get from the patients that we serve—and we need to be their voice.
Research, Education & Innovation Week will be back next year on April 13-17, 2026.
Posters at the REI Week 2025 Monday, March 31 poster session.
Panelists discuss innovation during REI Week 2025.
Global Health Initiative community engagement event during REI Week 2025.
Chris Rees presents his REI Week 2025 lecture.
Nathan Kuppermann listens to a presenter during the REI Week 2025 Tuesday, April 1, poster session.
Michelle Riley-Brown, Nathan Kuppermann, Catherine Bollard and Naomi Luban on stage during the REI Week 2025 awards ceremony.
Brandy Salmon presents on innovation programs at Virginia Tech during the REI Week 2025 Innovation Day.
Catherine Bollard listens to a presenter during the REI Week 2025 Monday, March 21 poster session.
Ambroise Wonkman poses for a picture with Children’s National staff.
Tanzeem Choudhury presenting during REI Week 2025.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/04/REI-Week-2025-Monday-Poster-Session-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-04-22 10:31:052025-09-19 12:09:57REI Week 2025 empowers the future in pediatric research and innovation
A recent study from the Division of Colorectal and Pelvic Reconstruction at Children’s National Hospital, led by Chief Marc Levitt, MD, explores the prevalence of additional abnormalities in children born with anorectal malformations (ARM). While many of these abnormalities co-occur, including vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula or esophageal atresia, renal defects and limb defects, known as the VACTERL association, the study reveals that some critical anomalies, particularly spinal cord and gynecologic malformations, are often missed, an oversight that can significantly affect patient outcomes.
What it means
This multi-institutional retrospective study aimed to assess the effectiveness of current diagnostic criteria for VACTERL screening in ARM patients and to identify anomalies that are at risk of being overlooked. The researchers utilized data from the Pediatric Health Information Systems database, which includes over 100 children’s hospitals, to analyze a wide range of associated abnormalities in ARM across the United States.
The findings highlight that the most common anomalies in ARM patients include cardiac, vertebral/spinal, renal and gynecologic (in females). While many of these anomalies are diagnosed at birth, the study suggests that some are identified only later in a patient’s care, pointing to a gap in early screening, particularly for spinal cord and gynecologic issues.
Based on the study’s results, the authors propose an expansion of the VACTERL acronym to VACTE(G)RLS to stress the importance of gynecologic (G) and spinal cord anomalies (S) in ARM patients.
Based on the study’s results, the authors propose an expansion of the VACTERL acronym to VACTE(G)RLS to stress the importance of gynecologic (G) and spinal cord anomalies (S) in ARM patients. This expanded acronym would help ensure that both surgical and non-surgical providers are aware of these often-missed malformations, improving early diagnosis and intervention.
Why it matters
Although other studies have examined the prevalence of VACTERL anomalies in ARM patients, this is the first to compare diagnosis rates at birth with diagnoses made later during subsequent hospital admissions. Timely identification of these associated malformations is crucial for early intervention in females, as untreated gynecologic anomalies can lead to reproductive issues later in life and for patients with spinal conditions that require intervention.
The proposed change to the standard usage VACTERL acronym underscores the significance and frequency of these malformations happening in combination, potentially leading to improved screening protocols and, ultimately, better patient outcomes. By emphasizing the importance of comprehensive screening at birth, the study advocates for a more thorough approach to diagnosing ARM-associated anomalies, which can significantly enhance long-term care for these patients.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/03/Young-Girl-Hematology-Patient-1.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-03-12 15:55:342025-03-20 11:34:47Study highlights need for improved screening in anorectal malformation patients
Before this study, little has been documented about how anorectal malformation type, sacral ratio, age and bowel regimen affect continence and quality of life.
A large, multi-institutional study including patient-reported outcomes for children who have anorectal malformations found that the type of malformation and whether a child is clean/continent and not soiling can have a significant impact on the assessment of a patient’s quality-of-life. The study also highlights that patients and their families seem to benefit from access to a specialized center offering multi-disciplinary care in a single location.
What it means
The study is one of the first to collect input from patients and their families at two multi-disciplinary centers for colorectal care. The authors, including Marc Levitt, MD, chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital, who collaborated with colleagues at Nationwide Children’s Hospital in Columbus and Royal Children’s Hospital in Melbourne Australia, sought to understand the impact of the anorectal malformation type and the development of the sacrum bone on continence outcomes in children. Additionally, the team aimed to compare continence outcomes by age group and determine the quality of life with different bowel regimens, including medications like laxatives or the use of enemas.
The researchers found that continence in patients taking laxatives to manage their bowels varied depending on the type of malformation, but that sacral ratio or a measure of the growth of a key pelvic bone correlating with pelvic floor development, did not seem to play a role in continence.
Additionally, patients (and patient families) had similar perceptions of their overall quality of life, as long as the child was clean/continent. Quality-of-life scores were lower, however, if a child was managed using enemas but continued to experience soiling/incontinence. This vital component was a measure of patient reported outcomes, or how the patient perceives their care is going.
Why it matters
Before this study, little has been documented about how anorectal malformation type, sacral ratio, age and bowel regimen affect continence and quality of life. For the first time, these reports are coming from the patient and family point of view. In their conclusion, the authors note that the study’s findings provide important discussion points for counseling patients on long term management strategies for children with anorectal malformations. The findings also identify new areas for research driven by what patients and their families report are most important.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/02/Rectoperineal-fistula-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-02-25 13:24:552025-02-25 13:26:50Patient-reported outcomes for children with anorectal malformation
Children’s National is ranked one of the top 10 pediatric hospitals in the nation by U.S. News & World Report. Our faculty and staff are proud of the impact made on the lives of children and families in our community. Your participation in the U.S. News & World Report annual reputational survey validates the quality of care we provide and reflects the mutual respect and trust we share as healthcare professionals.
How to determine your voting eligibility
Voting for the U.S. News & World Report Best Children’s Hospitals rankings can be done only through Doximity.
To participate, physicians must:
Be board-certified and meet the eligibility criteria for the voting categories.
For child and adolescent psychologists, your account must be up to date with your specialty and subspecialty correctly marked.
Be a credential-verified member of Doximity (you must have an active and claimed Doximity profile).
Have all certifications and board documents currently up-to-date in your Doximity profile.
You have to claim your profile on Doximity.com to participate in the online survey. If you have not yet claimed your Doximity profile, go to Doximity.com, and click “Find My Profile.”
Once your profile has been claimed, you must confirm your email address and board certifications.
Verified Doximity members will receive an email inviting them to participate in the U.S. News survey.
For more information on how to claim your profile, visit Doximity.com
How to update and verify existing Doximity account information
Your Doximity profile must have up-to-date licenses, certifications and board documents.
Once you are logged in, your profile will automatically be in “Edit Mode.” You are able to add new items or edit existing information.
Update your Doximity profile and ensure your information is current.
Once registered, users wishing to participate in the online survey should:
Watch for an email from Doximity about the annual member survey.
Even if you don’t see the email, if you are a registered Doximity user, you can still vote by logging in to Doximity.com with your username and password during the voting period.
Once logged in, look for a U.S. News graphic or button on the homepage and click on it.
The survey asks users to name the hospitals that provide the best care in your respective specialty, without consideration to location or cost. Pediatric specialists will list 10 hospitals. The order in which you list the hospitals does not matter.
Please note: Children’s National Hospital is listed as “Children’s National Hospital Washington, DC” on the survey.
Visit Doximity’s FAQs if you have issues or questions about registration or claiming your profile.
How to cast your vote
In February 2025 when voting opens, all survey-eligible physicians will receive a notification on the Doximity app for Android or iOS. If you do not use the Doximity app, you will receive an email when voting opens.
Log in to your Doximity account at doximity.com or via the mobile app.
Click the Notifications icon or tap the “Submit your Nominations” button on the homepage. You can also search for “U.S. News Best Hospitals”
Select 10 hospitals in your respective specialty that you believe provide the best care in the United States.
Submit your vote
Having technical issues?
If you have difficulty registering with Doximity or completing the survey, please visit Doximity support for assistance.
Vote
The 2025 U.S. News & World Report Best Children’s Hospitals reputation voting will open in mid-February. Look for your Doximity notification to vote.
Meet the winners (left to right): Syed M. Anwar, Ph.D., M.S., principal investigator at Children’s National; Daniel Capellan Martin, M.Sc., Polytechnic University of Madrid; Abhijeet Parida, data scientist at Children’s National; and Austin Tapp, Ph.D., postdoctoral research fellow at Children’s National.
Using an award-winning artificial intelligence (AI) algorithm developed at Children’s National Hospital, researchers ranked first in the world in the Brain Tumor Segmentation-Africa (BraTS-Africa) challenge for their approach to identifying different parts of deadly gliomas. The details of their innovative method were recently published on arXiv, a curated research-sharing platform.
“Technology can bridge the gap in healthcare between high- and low-resource countries,” said Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor in Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation (SZI). “By tailoring methods we created at our hospital to fit the needs of specific regions, such as sub-Saharan Africa, our research helps improve medical imaging and diagnosis in challenging environments.”
Dr. Linguraru was the program chair of the International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI) 2024 in Marrakesh, Morocco, the leading global meeting on AI in medical imaging.
Children’s National leads the way
Gliomas are a type of brain tumor with a high death rate and are especially difficult to diagnose in low- and middle-income countries. Given the increased need in Africa, researchers worldwide came together in Morocco to compete over the best way to accurately detect and measure tumors using MRI data and AI.
By applying advanced machine-learning techniques, the researchers adapted tools initially designed for well-resourced settings to work in countries with far fewer.
The study focused on transfer learning, a process in which an AI model is trained in advance on a large number of brain tumor images and then adjusted to work with smaller sets of new data. In this case, the models were adapted to work with local sub-Saharan African data using a strategy to combine different models’ strengths.
When tested, the approach achieved impressive accuracy scores. The Children’s National team, which included a colleague from the Polytechnic University of Madrid, ranked first in the BraTS-Africa 2024 challenge for identifying different parts of gliomas.
“To make the method widely available, the winning algorithm is shared online for others to use and improve upon,” Dr. Linguraru said. “My favorite part of these competitions is how they highlight the way innovation and collaboration can reduce global healthcare inequalities.”
The big picture
Children’s National researchers consistently lead global events using AI and advanced imaging to tackle complex healthcare challenges. In 2023, the team won a global contest to measure pediatric brain tumors at the MICCAI 2023 Conference. This year’s success in the BraTS-Africa challenge builds on this knowledge base and expands its use to adult gliomas.
At the Radiological Society of North America 2024 annual meeting, which drew 50,000 attendees, Zhifan Jiang, Ph.D., a staff scientist in the Precision Medical Imaging Lab at SZI, also won the Cum Laude Award for his scientific poster on applying AI to radiological images to predict severe outcomes for children with brain tumors caused by neurofibromatosis type 1.
“These achievements show how our science is leading the world in using AI for good,” Dr. Linguraru said. “Every day, we’re building on our knowledge of advanced imaging, brain tumors and AI to improve the diagnosis, measurement and treatment of deadly tumors — on a global scale.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/Brats2024-Team-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-10 17:12:152025-01-10 17:17:51AI for good: Children’s National wins global competitions for measuring brain tumors
Dr. Asa Yancey’s pioneering operation went unrecognized for over half a century due to discriminatory publishing practices in academic medicine.
A group of international pediatric colorectal surgery leaders called for the renaming of a surgical procedure for Hirschsprung disease after finding evidence that an African American surgeon, Asa Yancey, M.D., had pioneered the procedure 12 years before its’ current namesake, Franco Soave, M.D. Dr. Yancey was not recognized previously due to discriminatory practices in academic medical publishing.
What it means
A literature review published in the Journal of Surgical Research conducted by the American Pediatric Surgical Association Hirschsprung disease interest group, including Marc Levitt, M.D., chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital, identified that Dr. Yancey’s work describing pull-through of normal colon through a cuff of aganglionic colon as a treatment for Hirschsprung disease was published in 1952. The paper by Soave was published in 1962 and from that work, the “Soave” procedure bore his name.
The authors point out that Dr. Yancey’s pioneering operation went unrecognized for over half a century because of the discriminatory segregation in the publishing practices of academic medicine dating back to the 1950s.
Moving the field forward
Dr. Levitt and his colleagues in the interest group suggested active changes to give posthumous credit to Dr. Yancey, including renaming the procedure to the Yancey-Soave pull-through technique.
Together with Dr. Yancey’s family, including his children, three of whom are physicians, the interest group and other surgeons have started using the procedure’s new name in presentations, operative notes, articles and book chapters.
At the end of their literature review recommending the update, the authors wrote, “Posthumous acknowledgment of Yancey was long overdue but signifies improvements in the inclusion of underrepresented groups in academic medicine while simultaneously reminding physicians that there is still much work to be done.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2025/01/Asa-Yancy-feature.jpg349284Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2025-01-06 16:18:252025-01-06 16:22:14Colorectal surgeons ensure recognition for surgical innovation of Dr. Asa Yancey
The Division of Colorectal & Pelvic Reconstruction team from Children’s National Hospital at the 2024 PLPLC Conference.
Medical professionals from across the world gathered in Atlanta, Georgia, for the 2024 Pediatric Colorectal and Pelvic Reconstruction Conference. This esteemed course, hosted by the Pediatric Colorectal and Pelvic Learning Consortium (PCPLC), provided comprehensive educational experiences to those caring for children with colorectal and pelvic disorders.
Children’s National Hospital staff showcased their expertise by leading in-depth discussions, presenting accepted abstracts and designing course programming across multiple specialty areas while highlighting the program’s focus on collaborative care. Led by Chief Marc Levitt, M.D., the division of Pediatric Colorectal and Pelvic Reconstruction is the first in the mid-Atlantic region to fully integrate surgery, urology, gynecology and gastroenterology into one cohesive program for children.
Andrea Badillo, M.D., Documentation Committee member, Education Committee member
Julie Choueiki, M.S.N., R.N., Allied Health Care Professionals Conference (AHCP) co-chair
Dr. Marc Levitt leads a hands-on simulation lab using validated surgical models for treating Anorectal Malformations and Hirschsprung Disease.
Invited speakers and topics:
Marc Levitt, M.D., Cloaca Advanced; Anorectal Malformations/Hirschsprung Disease Hands-On Course; Hirschsprung disease and Constipation
Briony Varda, M.D., M.P.H., Genitourinary Complications & Creative Solutions: A Case Based Discussion of Patients with ARM; Cloaca Basics; Challenging Case Presentations in Colorectal Care
Katherine Worst, N.P., CPNP-AC, Functional Constipation, Motility, Bowel Management Basics; Bowel Management of the Colorectal Patient Including Psychosocial Care and Pelvic Floor Physical Therapy; Cloaca Review Session for Allied Health Care Professionals
Allison Mayhew, M.D., Genitourinary Complications & Creative Solutions: A Case Based Discussion of Patients with ARM; Advanced Cloaca; Cloaca Exstrophy, Gynecologic Evaluation and Follow Up
Andrea Badillo, M.D., Functional Constipation, Motility, Bowel Management Basics; Genitourinary Complications & Creative Solutions: A Case Based Discussion of Patients with ARM; Pediatric Colorectal Knowledge Competition at Course Conclusion
Christina Ho, M.D., Urological Care for the Colorectal Patient for Allied Health Care Professionals
Meghan Mesa, B.S.N., R.N., C.P.N., Performing Colorectal Clinic Skills for Allied Health Care Professionals
Justine Gagnon, B.S.N., R.N., Performing Colorectal Clinic Skills for Allied Health Care Professionals
Oral Plenary Scientific Session:
Thomas Xu, Hospital Volume and Region Associated with Variation in Vacterl Screening Among Newborns with Anorectal Malformation An Opportunity to Optimize Screening Practices
Kirsten Das, Gynecologic Anomalies in Patients with Anorectal Malformations and Associated Anomalies: A National Retrospective Cohort from 2016-2023
Eugénie Lehembre-Shiah, Cloacal Malformation And Mullerian Agenesis: Management Of The Gynecologic Reconstruction For This Rare Situation
Dr. Andrea Badillo on the panel for Functional Constipation, Motility, Bowel Management Basics.
Thomas Xu, Frequency of Vacte(G)Rls Associated Anomalies in Newborns with Anorectal Malformations Across Hospitals within the Pediatric Health Information Systems Database: Neonatal Diagnoses and Beyond; Malone Antegrade Continence Enema (Mace) – Reassessment of Complications with Advancements in Technique; Antegrade Continence Enemas for Patients with Spina Bifida to Treat Fecal Incontinence, a Comparison with Patients with Non-Neurogenic Causes
Kirsten Das, Predicting The Need For Vaginal Augmentation In Patients Undergoing Cloacal Reconstruction
As a globally recognized expert in enhancing care of children with colorectal and pelvic reconstructive needs, Dr. Levitt, , along with Alejandra Vilanova-Sanchez, M.D., edited the textbook Pediatric Colorectal and Pelvic Reconstructive Surgery. As part of his commitment to advancing education about colorectal surgery, Dr. Levitt provided a copy of the textbook to every conference attendee.
In 2024, Children’s National Hospital continued to make remarkable strides across diverse areas of pediatric medicine, from groundbreaking technological innovations to critical health advocacy. The following compilation showcases ten significant stories that demonstrate the breadth and depth of the hospital’s impact, as featured in major national news outlets including NBC Nightly News, CNN, The Washington Post, The New York Times, NPR, The Today Show, Healio, and POLITICO. Delve into our 2024 news highlights for more.
Charles Berul, M.D., and a patient family talk about the pill-sized pacemaker that saved the life of Abby, an infant born with deadly heart defects. (NBC Nightly News)
Sivabalaji Kaliamurthy, M.D., addiction psychiatrist and director of the Addictions Program, spoke to CNN about the impact of drug addiction on teen health and the lack of resources available to treat opioid use disorder. (CNN)
Susma Vaidya, M.D., M.P.H., associate medical director of the IDEAL Clinic, shared her concerns about childhood obesity treatment recommendations issued today by a leading panel of independent U.S. health experts. (The Washington Post)
Shideh Majidi, M.D., M.S.C.S., and Emily Frymark, clinical dietitian, spoke about how the food pharmacy, created in partnership with the Capital Area Food Bank, benefits patients with diabetes and other chronic conditions. (The Washington Post)
Kendric Cromer, a 12-year-old boy being treated at Children’s National Hospital, became the first person in the world with sickle cell disease to begin a commercially approved gene therapy that may cure the condition. “This is a big effort,” says David Jacobsohn, M.D., ScM, M.B.A. (The New York Times)
Mikael Petrosyan, M.D., associate chief of General and Thoracic Surgery, discusses the stress medical staff face when treating young victims of gun violence. (NPR)
Landon, an 11-year-old patient, rang the bell at Children’s National Hospital with family, friends, doctors and nurses cheering after finishing his final round of chemotherapy. (The Today Show)
Monika Goyal, M.D., M.S.C.E., pediatric emergency medicine specialist and co-director of the Center for Translational Research, emphasized the need for awareness in addressing period poverty in teenagers and young adults. (Healio)
Kolaleh Eskandanian, Ph.D., M.B.A., P.M.P., vice president and chief innovation officer, participates in a panel discussion covering AI data collection, associated risks, reliance and other topics related to artificial intelligence. (POLITICO)
Children’s National patient Kendric Cromer, 12, became one of the first children ever to be treated with a newly approved gene therapy that will free him from the sickle cell disease that has stolen his childhood. (The New York Times)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/12/2024-News-Logo-Collage-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-12-26 11:34:102024-12-26 11:49:26Children’s National in the News: 2024
2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.
A study led by researchers at Children’s National Hospital showed that babies born during the COVID-19 pandemic have differences in the size of certain structures in the brain, compared to infants born before the pandemic. The findings suggest that exposure to the coronavirus and being pregnant during the pandemic could play a role in shaping infant brain development. (3 min. read)
Children’s National Hospital was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide. (2 min. read)
In January 2023, a team of multidisciplinary doctors performed the first case in the world of using bilateral high intensity focused ultrasound (HIFU) pallidotomy on Jesus, a 22-year-old patient with dyskinetic cerebral palsy. The procedure is part of a clinical trial led by Chima Oluigbo, M.D., pediatric neurosurgeon at Children’s National Hospital. (3 min. read)
A novel ultrasound device developed by Bloom Standard received the Food and Drug Administration’s valued breakthrough device designation with the help of Children’s National Hospital. The device that enables autonomous, hands-free ultrasound scans to be performed anywhere, by any user. (2 min. read)
Understanding the effects of Lyme disease on the developing fetal brain is essential to ensure timely prenatal and postnatal treatments to protect the fetus and newborn. In response to this need, Children’s National Hospital is leading a pilot study to establish the groundwork needed for a larger study to determine the effect of in utero exposure to Lyme disease on pregnancy and early childhood neurodevelopmental outcomes. (3 min. read)
Five years ago, Cayden was born 6 weeks early weighing less than four pounds and at risk of dying from her critical congenital heart disease. Today, she’s a happy five-year-old. Early diagnosis of her hypoplastic right ventricle, double inlet left ventricle and critical coarctation of the aorta allowed for the team at Children’s National Hospital to create a careful plan for safe delivery and to offer an innovative hybrid HLHS surgical approach at the hospital within 24 hours after she was born. (1 min. read)
Children’s National Hospital appointed Wayne J. Franklin, M.D., F.A.C.C., as the new senior vice president (SVP) of the Children’s National Heart Center. In this role, Dr. Franklin oversees the full spectrum of heart care services including cardiac imaging and diagnostics, interventional cardiology, electrophysiology, cardiac anesthesia, cardiac surgery and cardiac intensive care. (2 min. read)
By pioneering artificial intelligence (AI) innovation programs at Children’s National Hospital, Marius George Linguraru, D.Phil., M.A., M.Sc., and the AI experts he leads are ensuring patients and families benefit from a coming wave of technological advances. The team is teaching AI to interpret complex data that could otherwise overwhelm clinicians. (4 min. read)
Painting a sobering picture, a research team led by Children’s National Hospital culled years of data demonstrating that maternal mental illness is an under-recognized contributor to the death of new mothers. They called for urgent action to address this public health crisis. (3 min. read)
Children’s National Hospital appointed Nathan Kuppermann, M.D., M.P.H., as its new executive vice president, chief academic officer and chair of Pediatrics. In this role, Dr. Kuppermann oversees research, education and innovation for the Children’s National Research Institute as well as academic and administrative leadership in the Department of Pediatrics at George Washington University School of Medicine & Health Services. (2 min. read)
Researchers from Children’s National Hospital presented findings from the first clinical trial of the medication vosoritide for children with hypochondroplasia – a rare genetic growth disorder. During the phase 2 trial, researchers found vosoritide increased the growth rate in children with hypochondroplasia, allowing them to grow on average an extra 1.8 cm per year. (2 min. read)
Since its establishment in July 2023, the Center for Prenatal, Neonatal & Maternal Health Research at Children’s National Hospital has gained recognition through high-impact scientific publications, featuring noteworthy studies exploring the early phases of human development. (3 min. read)
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/12/2024-with-lightbulb-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-12-19 13:29:592024-12-19 13:33:52The best of 2024 from Innovation District
Nearly 200 biomedical leaders from Washington, D.C., Maryland, and Virginia gathered at the Children’s National Research & Innovation Campus for the 2nd annual Cell & Gene Therapy Symposium. The event showcased groundbreaking developments in rare disease treatments and underscored the importance of regional collaboration.
“By targeting diseases at the cellular level, we are on the cusp of breakthroughs in cell and gene therapy that will transform medicine,” said Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research (CCIR) at Children’s National Hospital and a host of the symposium. “Progress will accelerate if we build partnerships beyond our own organizations.”
The big picture
Scientists and clinicians have worked for more than two decades to develop cell and gene therapies aimed at treating diseases on a cellular level. The past few years have been particularly promising as investment in science has led to advancements. Children’s National is at the forefront, as one of the first pediatric hospitals in the world to offer commercial gene therapies for sickle cell disease.
Many more treatments for rare diseases are in development at Children’s National and beyond. Leaders at CCIR are actively building collaborations with companies, academic institutions and enterprises across the mid-Atlantic region to accelerate these efforts.
During the symposium, Eugene Hwang, M.D., chief of Oncology at Children’s National, addressed the urgent need for more effective and less toxic treatments for pediatric brain tumors. He highlighted the potential of combining immunotherapies with innovations like low-intensity focused ultrasound, which can open the blood-brain barrier temporarily to improve drug delivery to tumors.
“With collaboration between the lab and clinic, alongside industry partners and even between hospitals, we can finally make strides I haven’t seen in my entire career,” Dr. Hwang said. “It’s an incredibly inspiring time for all of us.”
Why it matters
Experts from organizations as diverse as MaxCyte, ScaleReady, RoosterBio, PSC Biotech, Qiagen, FujiFilm and the Frederick County Office of Economic Development came together for the daylong conversation.
Michael Friedlander, Ph.D., executive director of the Fralin Biomedical Research Institute at Virginia Tech, emphasized the critical role of regional partnerships in fulfilling the potential of these emerging therapies. He pointed to the collaborative research between Children’s National and Virginia Tech on brain tumors, where bioengineers and cancer researchers are working side-by-side to create new treatments.
“We are now able to begin delivering these leading-edge therapies to patients,” Dr. Friedlander said. “For example, those who live in rural settings often have much less access to such frontline medical innovations. By collaborating with Children’s National and gaining access to urban pediatric populations, as well as patients in our more rural area, we can start to bring these therapies to a much broader audience.”
What’s next
Patrick Hanley, Ph.D., chief and director of the Cellular Therapy Program at Children’s National, observed that other regions in the U.S. are uniting to advance scientific discoveries with the backing of government, academia and industry. He hopes to see similar collaboration across the D.C., Maryland, and Virginia area, known as the DMV. Children’s National is leading an initiative called CHARM – the Capital Health and Mid-Atlantic Regenerative Medicine – to bring regional experts together for webinars, networking events and partnership opportunities.
“There’s significant interest in cell and gene therapy worldwide,” said Dr. Hanley, a symposium host. “I see an even greater interest in creating cell and gene therapy hubs. The time is right for our mid-Atlantic region, and I’m excited to see what unfolds in the next five years.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/11/CGT-Conference-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-11-26 10:13:282024-11-26 10:15:14Regional powerhouse: Cell and Gene therapy leaders from mid-Atlantic forge connections
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2024-25 Best Children’s Hospitals annual rankings. This marks the eighth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
This year, U.S. News ended ordinal rankings on its Honor Roll. Instead of assigning a numerical rank from 1 to 10, all hospitals on the Honor Roll will be recognized as having attained the highest standards of care in the nation.
In addition, Children’s National tied for #1 pediatric hospital in the Mid-Atlantic region, which includes New York, New Jersey, Delaware, Pennsylvania, the District of Columbia, West Virginia and Virginia. It’s also best in the Mid-Atlantic in Neonatology.
For the fourteenth straight year, Children’s National ranked in 10 specialty services. New this year, U.S. News included behavioral health as a service line in the rankings. Since it’s the first year, there are no ordinal rankings for behavioral health, but the Children’s National program was named one of the top 50 programs in the country.
“In my first year here, I witnessed what makes Children’s National so special — our commitment to collaboration, empowering one another, and charting a bold path forward for pediatric care,” said Michelle Riley-Brown, MHA, FACHE, president and chief executive officer of Children’s National. “I’m proud U.S. News again recognized Children’s National as one of the top in the nation and the highest-ranked pediatric hospital in D.C., Maryland and Virginia. Together, we’ll continue to push the boundaries of care, research and innovation to make a difference for those who matter most — the kids.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals and recognizes the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News.
“For nearly two decades, U.S. News has published Best Children’s Hospitals to empower the parents and caregivers of children with complex medical needs,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “Children’s hospitals appearing on the U.S. News Honor Roll have a track record of delivering unparalleled specialized care.”
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
The Children’s National specialty services that U.S. News ranked in the top 10 nationally are:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/10/US-News-Badges-2024-25-CNRI.jpg385685Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-10-08 01:00:002024-10-08 15:01:23Children’s National again ranked among the best in the nation by U.S. News & World Report
Dr. Levitt shares insights into the program’s journey, key successes and future goals.
This September, the Colorectal and Pelvic Reconstruction Program at Children’s National proudly marks five years of commitment to patient-centered care for children and their families. Under the guidance of Division Chief Marc Levitt, M.D., the program has achieved remarkable advancements in clinical care, improving patient outcomes and enhancing family experiences.
Dr. Levitt shares insights into the program’s journey, key successes and future goals, highlighting the importance of collaboration among specialists and the continuous pursuit of innovative treatments.
Q: What was your vision for the program when it first launched? Has the vision changed?
A: When the Colorectal Program first launched, we aimed to establish a comprehensive program for colorectal patient care. This included integrating specialists across multiple disciplines, such as pediatric general surgery, urology, gynecology, gastroenterology, nursing, neurosurgery, orthopedics, pathology, radiology, anesthesia, psychology and pelvic floor therapy. Our efforts have exceeded expectations; the team has developed a cohesive and collaborative dynamic where each specialist contributes effectively to patient care. This integrated approach enhances outcomes, as patients and their families are at the center of our model, surrounded by a network of dedicated caregivers and coordinators, all focused on improving the patients’ quality of life.
Q: Can you highlight some key successes or achievements of the program?
A: The creation of our integrated colorectal care program at Children’s National has been a significant success, bolstered by strong institutional support. While this model requires considerable effort, it ultimately attracts patients and leads to outstanding outcomes. We’ve received patient inquiries from 48 states (AK,AL, AR, AZ, CA, CO, CT, D.C., DE, FL, GA, HI, IA, ID, IL, IN, KS, KY, LA, MA, MD, MI, MN, MO, MS, MT, NC, ND, NE, NH, NJ, NM, NV, NY, OH, OK, OR, PA, RI, SC, TN, TX, UT, VA, VT, WA, WI, WV) and 68 countries (Australia, Bahamas, Bangladesh, Bulgaria, Canada, Chile, Croatia, Cyprus, Dominican Republic, Ecuador, Egypt, England, Ethiopia, France, Germany, Greece, Guatemala, Haiti, Hong Kong, India, Ireland, Israel, Jamaica, Jordan, Kazakhstan, Kenya, Kuwait, Lithuania, Maldives, Mauritania, Mexico, Monaco, Morocco, Myanmar, The Netherlands, New Zealand, Nepal, Nigeria, Northern Ireland, Norway, Oman, Palestine, Pakistan, Paraguay, Papua New Guinea, Peru, Philippines, Portugal, Romania, Russia, Saint Lucia, Saudi Arabia, Scotland, Serbia, Singapore, Slovakia, Slovenia, Spain, Sri Lanka, South Korea, St. Kitts & Nevis, Sudan, Sweden, Ukraine, Uzbekistan, United Arab Emirates, Venezuela, Wales).
Some key successes include the development of innovative surgical procedures for conditions such as imperforate anus and anorectal malformations, advanced repair techniques for cloacal malformations, integrated care strategies for colonic dysmotility, and novel approaches for the newborn care of patients with cloacal exstrophy. All these new approaches were developed at Children’s National over the past five years.
In addition to clinical innovations, we have significantly enhanced our academic environment. Over the last five years, our team has authored more than one hundred articles and three well-regarded books, helping health care professionals around the world improve the care they provide to their patients. We have also trained surgical fellows and nurses in colorectal care and welcomed clinicians from over 30 countries for specialized training. This outreach is especially fulfilling, as it enables us to influence the care of children around the globe whom we may never meet, by sharing valuable skills and knowledge with these practitioners.
Q: Can you share examples of particularly challenging cases or high-profile cases that have influenced the program’s clinical approach?
A: The way we care for a patient with a cloaca is unique – the entire team joins together in the operating room to assess the anatomy, and every member then gives their thoughts on how to approach the reconstruction. The very next day we perform that surgery, with the understanding of the anatomy in mind, and what plays out in that operating room is quite magical. This collaborative approach frequently leads to exceptional outcomes, as our diverse ideas come together to form a cohesive plan. Through this teamwork, we have developed creative ways to solve complex anatomical problems that no one individual surgeon would have thought of on their own.
Q: How have patient outcomes improved over time?
A: We have optimized the collaborative experience so that patients only need a single visit to see all the specialists they require. Our outcomes for complex colorectal surgeries have significantly improved, particularly for conditions like cloaca, Hirschsprung disease and anorectal malformations. Advances in surgical techniques and enhancements in nursing care have led to dramatically better results. We have reduced, and in some cases eliminated, complications from these surgeries, while also seeing improvements in bowel continence and kidney health. Our nursing teams — outpatient, operating room and inpatient — play a crucial role, offering unique insights into pre- and post-operative care that are vital for achieving successful outcomes.
Q: What have been the biggest challenges or barriers faced by the program and how have you addressed these challenges?
A: One of the biggest challenges we face is ensuring that patients can get to us. Many patients encounter obstacles with insurance companies that restrict travel outside their network, or they deal with the difficulties of traveling from far away for their surgery. We have worked diligently to address these issues by improving our insurance approval process and making families comfortable during their stay in Washington, D.C., including assistance with accommodations, necessary medical supplies, etc. If we can remove these barriers, we can care for more patients and make the experience easier for them and their families.
Q: How does the colorectal program collaborate with other departments or services? How has the program integrated from various specialties (e.g., urology, gynecology, GI) to enhance patient care?
A: We have specialists who are fully integrated in their roles on the colorectal and pelvic reconstruction team. General pediatric surgeons, urologists, gynecologists and gastroenterologists work both in the colorectal program and in their home program in a uniquely integrated fashion. For example, our urologists each spend half of their time in general urology and the other half in colorectal, handling the urologic aspects of colorectal patients’ care. In this way collaboration is enhanced and encouraged.
Q: What are the future goals or plans for the colorectal program?
A: Our future goals for the colorectal program are focused on expanding our impact and enhancing patient care. First and foremost, we aim to help as many patients as possible. We plan to collaborate with other colorectal centers worldwide to share knowledge and best practices. Training surgeons and nurses remains a priority, as we want to equip as many healthcare professionals as possible with the skills needed in this field. Additionally, we are committed to traveling to the developing world to provide care for children who cannot access services at Children’s National. Finally, we intend to enhance our research efforts, leveraging basic science to investigate and address conditions related to the colon, ultimately seeking to reduce or eliminate associated illnesses.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/09/Levitt-and-baby-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-09-23 15:51:302024-09-26 09:59:03Marc Levitt, M.D., reflects on the Colorectal & Pelvic Reconstruction Program
For the last several years, the physicians, advance practice providers, and nurses within the Division of Colorectal and Pelvic Reconstruction at Children’s National Hospital have sought to establish standardized protocols for diagnosing and treating children with severe constipation unresponsive to medical management. Their work seeks to create a collaborative approach that brings gastroenterologists with motility expertise and colorectal surgeons together from the start to streamline testing, analysis, and to avoid unnecessary surgical procedures.
To that end, the team has published several studies that make the case for such a protocol based on their experiences managing this unique population.
What it means
In a 2022 study, the team conducted a retrospective review of children referred for retractable functional constipation to the Division of Colorectal and Pelvic Reconstruction at Children’s National. A unique algorithm for assessment and treatment was created based on the data analysis.
The resulting proposed protocol for medically refractory constipation provided a collaborative framework to standardize the work-up and treatment. This protocol led to the use of antegrade flushes via appendicostomy to empty the colon and was able to in most cases avoid a colonic resection, something done much more commonly in the past
A 2023 study further reiterated the importance of these collaborative approaches, stating, “It is vitally important to recognize that constipation exists on a spectrum of severity with multiple potential etiologic factors and therefore treatment must be customized based on the individual’s symptom, anatomic and manometric findings.”
The 2023 study also introduced an enhanced standardized algorithm to evaluate and treat refractory constipation, with the central idea being a consolidation of evaluation and initiation of treatment into a single combined procedure. This means collaboration between gastroenterology and colorectal surgery in the operating room by including anorectal manometry at the start to rule out anatomic anomalies as the cause of the constipation and to test motility.
Why it matters
In the 2023 study, the authors wrote, “While algorithms for initial evaluation and treatment of functional constipation in children have been described, most articles in the pediatric literature lack details about the work-up and management of those refractory symptoms and the approaches described for such patients vary widely among clinicians.”
That means that children with functional constipation for whom medical treatment has failed face a drastically lower quality of life. Functional constipation and encopresis, or stool soiling, correlates with a higher prevalence of low self-esteem, social withdrawal, and depression. It is critical to correctly diagnose and efficiently treat these conditions and work together to do it quickly.
Children’s National leads the way
As one of the nation’s leaders in pediatric colorectal and pelvic reconstructive surgery, Children’s National, led by Division Chief Marc Levitt, M.D., receives more referrals asking for a surgical solution for severe pediatric constipation than any other center in the world.
Caring for such a large population positions the team to analyze evidence and establish protocols based on statistically relevant numbers of patients. The studies outlined above are the result of the innovative design of the Division of Colorectal and Pelvic Reconstruction, in which multiple divisions involved in the care of these patients, from Gastroenterology to Urology and beyond, experience an unprecedented ability to work together, including in the operating room. It is a fully integrated program with experts in colorectal surgery, GI motility, and colorectal nursing embedded into the same team.
While most children with functional constipation will respond to medical treatment, for those who need further help that includes surgical assessments, the evidence-based algorithms developed in these studies can truly be life-changing for these children and their families.
Read the studies in the Journal of Pediatric Surgery:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/08/colorectal-surgeons-featured.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-08-14 15:05:042024-08-15 13:38:04Multi-disciplinary collaboration key in any approach to refractory functional constipation
Clinicians can better manage care for children with total colonic Hirschsprung disease by drawing on the collective expertise from the people who have seen and treated patients with this condition, says Marc Levitt, M.D.
Clinicians can better manage care for children with total colonic Hirschsprung disease, a rare form of the condition, by drawing on the collective expertise from the people who have seen and treated patients with this condition, says Marc Levitt, M.D., chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital.
What is it?
Dr. Levitt and fellow experts within the APSA Hirschsprung Disease Interest group are working together to develop recommendations based on their collective experiences managing the condition. Their recommendations will include specifics for the diagnosis and management of total colonic Hirschsprung disease (a rare type of Hirschsprung disease that involves the entire colon) before and after reconstruction, such as diagnostic criteria, surgical approaches, bowel management, diet, antibiotic prophylaxis, colonic irrigations and post-surgical considerations.
Specifically, the group’s consensus findings and recommendations include:
Specific information about using a contrast enema for this diagnosis — namely that there is no obvious transition zone identified.
The importance of a surgical approach of colonic mapping to obtain definitive pathology and ileostomy at the time of diagnosis, which is key to getting a child with this condition feeding and growing.
Monitoring that growth with nutritional assessment and oral sodium supplementation are vital to their care.
High output stomas and loose stool after pull-through can be more readily treated now with anti-motility agents, and better care of the parastomal and perineal skin.
Why does it matter?
Children with total colonic Hirschsprung disease are unique among children with Hirschsprung disease. They present specific pre- and post-operative management challenges. Creating and sharing consensus guidelines will create a rational, expert-based approach to diagnosing and managing the condition based on direct clinical experience, that others can draw from. Because the condition is relatively rare, care decisions historically have been made based mainly on literature about it. However, that literature often shows a lack of clear consensus on how to approach the condition.
Children’s National leads the way
Dr. Levitt and his colleagues collectively have seen more cases of total colonic Hirschsprung disease than any other clinicians in the world and have helped to author better guidelines specifically to try to standardize the pre- and post-operative management of this patient group. The goal is to improve the likelihood of a better outcome for the child no matter where a family goes for care.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/07/Dr-Levitt-in-the-OR-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-07-22 12:10:302024-07-22 12:12:06Better standardized care for total colonic Hirschsprung disease
Our Global Health Initiative launched in 2016 with the goal of eliminating pediatric health disparities around the world. We aim to address the most pressing pediatric health issues through better care for medically underserved populations. This leadership helps us achieve our mission of caring for all children. A broad range of education and research projects improves health outcomes. They also offer enriching opportunities for experienced faculty and emerging leaders to advance clinical excellence.
Healing hearts in Uganda
Dr. Craig Sable and team train partners in Uganda.
Craig Sable, M.D., interim chief of Cardiology, improves care for young people with rheumatic heart disease (RHD) in Uganda. Donors, including the Karp Family Foundation, Huron Philanthropies, Zachary Blumenfeld Fund and the Wood family, make this possible. RHD affects 50 million people, mostly children, worldwide. It claims 400,000 lives each year.
Dr. Sable and Ugandan partners completed important research showing that early RHD detection, coupled with monthly penicillin treatment, can protect the heart. They are working on practical solutions, such as a new portable device with artificial intelligence (AI) that can easily screen for RHD.
In 2023, Dr. Sable led two missions in Uganda where he and his team did surgeries and special tests for 18 children with RHD. They also taught local doctors new skills to help more kids on their own.
Plastic surgery and reconstructive care in Kenya and Nepal
Each year our Craniofacial & Pediatric Plastic Surgery team, under the leadership of Johnston Family Professor of Pediatric Plastic Surgery and Chief of Pediatric Plastic Surgery Gary Rogers, M.D., J.D., LL.M., M.B.A., M.P.H., provides opportunities for fellows to participate in surgical missions.
In 2024, Perry Bradford, M.D., traveled to the Moi Teaching Hospital in Eldoret, Kenya where she provided patients with burn, pressure wound and cleft reconstruction. She built community connections with the local plastic surgeons and educated registrars and medical students. “This gave me firsthand experience working in a community with limited resources and forced me to be more creative,” Dr. Bradford says. “The experience inspired me to examine what it means to have consistent access to advanced tools and equipment.”
In 2022, a group traveled to Nepal to provide care. Some patients arrived after days of travel by yak or buffalo. One child with a burn injury recovered use of her hand. The team educated local providers to deliver life-changing treatments unavailable in Nepal.
Dr. Tesfaye Zelleke, left, and team in Ethopia.
Elevating epilepsy care in Ethiopia
Neurologist Tesfaye Zelleke, M.D., and partners in Ethiopia are seeking to improve the lives of children with epilepsy. The BAND Foundation provides support. Ethiopia has a population of about 120 million yet only a handful of pediatric neurologists.
Dr. Zelleke’s team trained nonspecialist providers to diagnose and treat children in the primary care setting. They also launched a mobile epilepsy clinic to provide community care and build the capacity of local clinicians. In collaboration with advocacy groups, the team educates the public about epilepsy with a goal of reducing stigma.
New hope in Norway
In 2023, our Division of Colorectal & Pelvic Reconstruction shared its expertise with clinicians at Oslo University Hospital, Rikshospitalet, in Norway. This effort was a key first step in Oslo becoming the first dedicated colorectal center in Scandinavia.
Marc Levitt, M.D., and team members performed complex surgeries otherwise unavailable for waiting patients. They led an academic conference. They held clinics to educate nurses, reviewed patient records and made care recommendations. Specialized care enabled a young patient with significant bowel difficulties to recover function and lead a normal life.
The team will travel to South Africa, the Czech Republic and Spain in 2024. Donors, including The Dune Road Foundation and Deanna and Howard Bayless, make this work possible.
Improving outcomes for babies in the Congo
AI can be a valuable tool for diagnosing genetic conditions. It detects unique facial patterns that clinicians without genetics training can miss. However, existing facial analysis software struggles in nonwhite populations.
A team led by Marius George Linguraru, D.Phil., M.A., M.Sc., the Connor Family Professor of Research and Innovation and principal investigator in the Sheikh Zayed Institute for Pediatric Surgical Innovation, is working to improve the newborn diagnosis rate worldwide. They are testing smartphone software in the Democratic Republic of Congo. Diverse newborn data improves AI’s ability to detect a variety of genetic conditions in more children. Early detection, diagnosis and informed care lead to better health outcomes.
Nephrology care for kids in Jamaica
Jennifer Carver and Dr. Marva Moxey-Mims, center, with staff at Bustamante Children’s Hospital.
Marva Moxey-Mims, M.D., chief of Nephrology, is bringing care to children with kidney disease in Jamaica, with a goal of improving health equity. An International Pediatric Nephrology Association grant helped make it possible.
On a recent trip, Dr. Moxey-Mims and a small team — including Jennifer Carver, RN, CNN, lead peritoneal dialysis nurse at Children’s National, and three pediatric nephrologists from Jamaica — trained nearly 30 nurses from Jamaican hospitals. Nurses received hands-on dialysis education to improve their clinical skills. The team also worked to educate the community in disease awareness and prevention.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/07/DrSable-feature.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-07-02 12:33:202025-02-28 12:30:01Around the world
“Within the field of pediatric colorectal and pelvic reconstruction, the most complex anatomic problem a pediatric surgeon can face is that of a cloacal malformation,” writes Marc A. Levitt, M.D., chief of Colorectal and Pelvic Reconstruction at Children’s National Hospital. A new, first-of-its kind textbook, Cloacal Malformations: Case Studies, seeks to shed light on the multi-disciplinary care required to care for people with this rare condition — when the urinary, gynecologic and colorectal system all exit the body via a common channel which requires reconstruction.
What is it
Dr. Levitt’s fifth textbook, Cloacal Malformations: Case Studies, is the first comprehensive account of all the care elements needed to successfully treat and manage care for someone with a cloacal malformation. It includes preoperative evaluation and surgical planning, the anorectal malformation (ARM) index, surgical reconstruction, urological evaluation and long-term care. Also covered are the gynecologic evaluation and needed interventions, neurological implications, bowel management and the long-term management of patients with cloacal malformations.
The book’s associate editors hail from some of the subspecialties that are critical to caring for these conditions, including:
Tamador Al-Shamaileh, M.D., pediatric colorectal and general
Andrea T. Badillo, M.D., pediatric colorectal and pelvic reconstruction
Allison C Mayhew, M.D., pediatric gynecology
Teresa L. Russell, MS, colorectal and pelvic reconstruction research
Briony K Varda, M.D., pediatric urology
Richard J Wood, M.D., pediatric colorectal and pelvic reconstruction
Why it matters
This textbook is a compelling resource for all clinicians caring for patients with cloacal malformations. It includes case studies that provide insights into a variety of different clinical scenarios, the first publication to categorize the different types of cloaca, as well as full brand new colored illustrations to enable the reader to understand and gain experience from detailed descriptions.
It is the first of its kind to address the full spectrum needs of someone with a cloacal malformation and will help improve and standardize care for this complex patient population no matter where that patient lives in the world.
Children’s National leads the way
Dr. Levitt is the most experienced pediatric colorectal surgeon in the world. Having performed more than 15,000 procedures during his career, he has cared for more children with cloacal malformations (1,000 cases) and other complex congenital colorectal conditions than anyone else. The information he shares in this textbook, and his previous books, is intended to enhance the care of all children with colorectal and pelvic reconstructive needs, “whether they come into our clinic or are seen by a colleague anywhere in the world,” he notes.
The range of expertise involved in the creation of this textbook reflects Dr. Levitt’s unique approach to pediatric colorectal and pelvic reconstruction, which includes a strongly integrated team of pediatric colorectal surgeons, urologists, gynecologists, gastroenterologists and nurses.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2024/03/Cloacal-Malformations-textbook-feature.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2025/09/InnovationDistrict_CN_WebHeader-1396px-1030x151.pngInnovation District2024-04-09 07:00:042025-02-13 18:54:55First textbook for cloacal malformations offers deep dive into care and treatment


 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the U.S. News & World Report 2025-26 Best Children’s Hospitals annual rankings. This marks the ninth straight year Children’s National has made the Honor Roll list. The Honor Roll is a distinction awarded to only 10 children’s hospitals nationwide.

















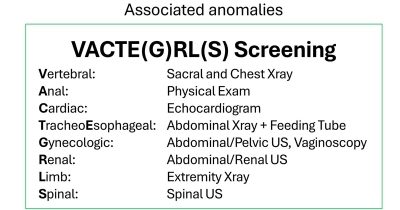
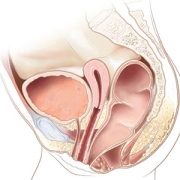
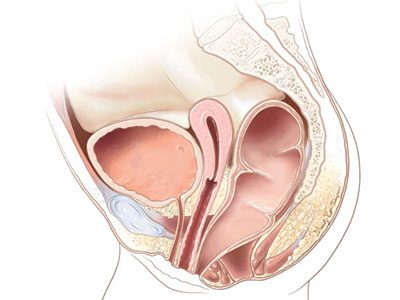








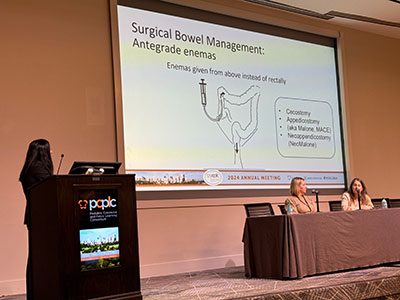

 2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.
2024 marked another groundbreaking year for Children’s National Hospital, showcasing remarkable advances across the spectrum of pediatric medicine, research and healthcare innovation. From pioneering surgical procedures to breakthrough artificial intelligence applications, the institution continued to push the boundaries of what’s possible in children’s healthcare. Read on for our list of the most popular articles we published on Innovation District in 2024.

 Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the
Children’s National Hospital in Washington, D.C., was ranked as a top hospital in the nation by the 
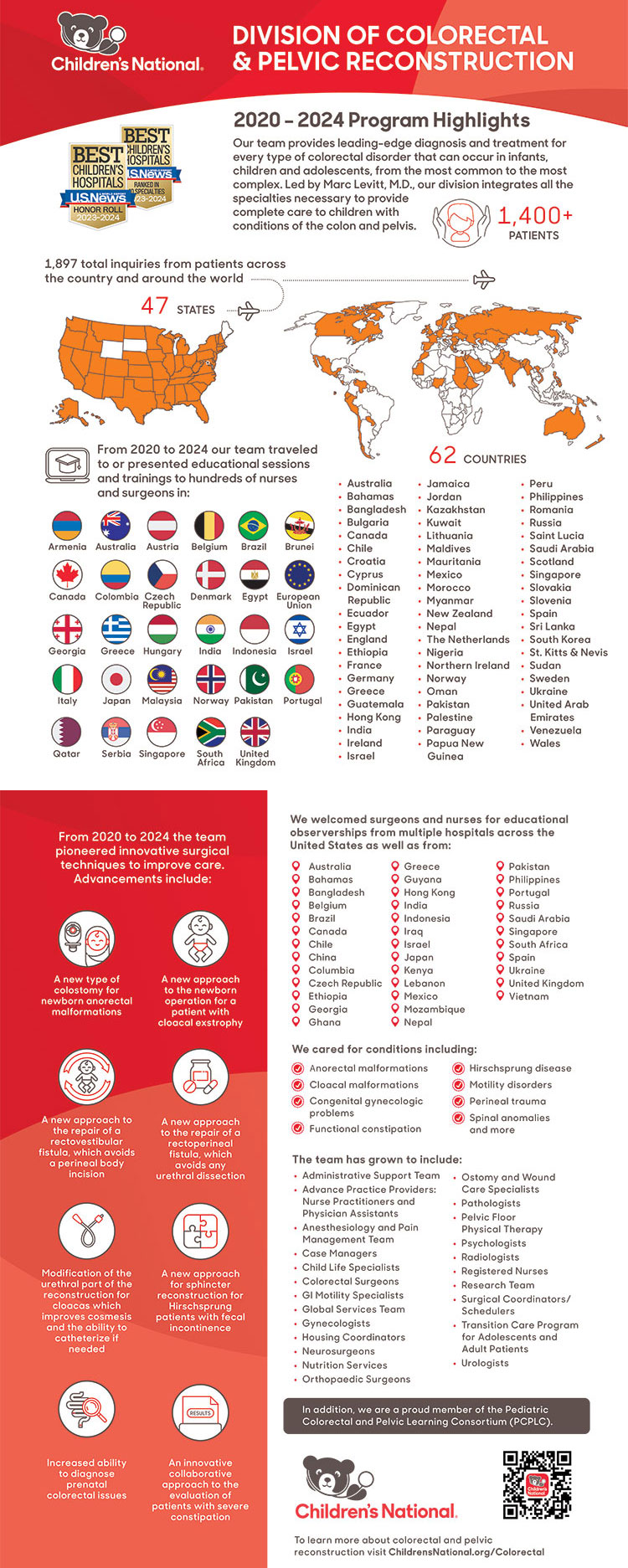



 For the last several years, the physicians, advance practice providers, and nurses within the
For the last several years, the physicians, advance practice providers, and nurses within the 





 “Within the field of pediatric colorectal and pelvic reconstruction, the most complex anatomic problem a pediatric surgeon can face is that of a cloacal malformation,” writes
“Within the field of pediatric colorectal and pelvic reconstruction, the most complex anatomic problem a pediatric surgeon can face is that of a cloacal malformation,” writes 