Neurocognitive and emotional factors predict hospital visits in children with SCD
Neurocognitive and emotional factors are predictors of visits children with SCD make to the hospital.
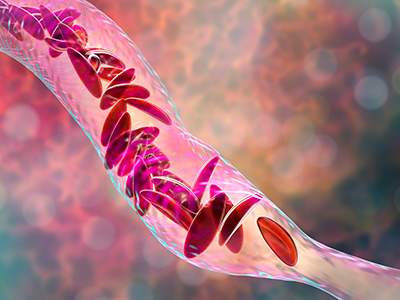
Many children with sickle cell disease (SCD) experience significant pain that often results in trips to the emergency department (ED) or hospitalization. Disease characteristics explain some – but not all – of the variability in pain-related healthcare utilization. In a new study published in Pediatric Blood & Cancer, experts examined the role of neurocognitive functioning and emotional factors in predicting future healthcare visits for pain up to three years later.
The big picture
In the 3-year study of 112 youth with SCD between ages 7-16, researchers found that poorer attentional control and greater emotional distress predicted more ED visits and hospitalizations for pain years later.
Past studies that have pointed to the importance of neurocognitive and emotional factors in the experience of pain have only looked at relationships at a single point in time.
“Those types of studies limit our ability to evaluate the directionality of relationships and consider the implications of neurocognitive functioning and emotional well-being for children’s health as they get older,” said lead author Steven Hardy, Ph.D., director of Psychology and Patient Care Services and psychologist in the Center for Cancer and Blood Disorders (CCBD) at Children’s National Hospital.
Why it matters
This study advances the understanding of the effects of neurocognitive functioning and emotions on the course of pain and disease morbidity in pediatric SCD.
Additionally, the findings will benefit patients by shedding light on potential intervention targets to support effective pain management.
“It also helps to reframe the conversation around pain and healthcare utilization in SCD by broadening our understanding of the factors that precipitate pain to include neurocognitive functioning and mental health,” Dr. Hardy added.
What’s unique
This work demonstrates that factors beyond disease characteristics are important to consider in a comprehensive approach to managing pain and improving quality of life for children with SCD.
“It shows that we also need to be thinking about how neurocognitive functioning and mental health affect one’s ability to manage their disease in terms of taking medications, avoiding pain triggers, coping with pain, communicating about symptoms and advocating for needs,” Dr. Hardy said. “Future work will look to see if we can preserve neurocognitive functioning and support mental health as a way to reduce pain impairment and improve quality of life.”
Children’s National is conducting several studies focused on better understanding the course of neurocognitive functioning and pain in pediatric SCD. Psychologists in the CCBD are also exploring novel interventions to preserve neurocognitive functioning and promote the development of effective strategies for coping with pain in SCD.






 A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.
A clinical trial testing a new drug to increase growth in children with short stature. The first ever high-intensity focused ultrasound procedure on a pediatric patient with neurofibromatosis. A low dose gene therapy vector that restores the ability of injured muscle fibers to repair. These were among the most popular articles we published on Innovation District in 2022. Read on for our full top 10 list.