In a systematic review and meta-analysis published in JAMA Pediatrics, researchers at Children’s National Hospital found that interventions focused on health, environment and community were associated with the greatest reduction in asthma-related emergency department visits and hospitalizations among children.
In a systematic review and meta-analysis published in JAMA Pediatrics, researchers at Children’s National Hospital found that interventions focused on health, environment and community were associated with the greatest reduction in asthma-related emergency department visits and hospitalizations among children. The findings suggest that addressing social risks may be a crucial component of pediatric asthma care to improve health outcomes.
“There are persistent and striking disparities in asthma outcomes among children,” said Jordan Tyris, M.D., hospitalist fellow at Children’s National and lead author. “Understanding how to address these is of utmost importance.”
“Literature on the spectrum of social factors, including social needs, social risks and social determinants, has increased recently across many aspects of health care,” adds Dr. Tyris. “But much of this literature has focused on adults with chronic conditions, for example diabetes or high blood pressure.”
The study authors searched PubMed, Scopus, PsychINFO, SocINDEX and CINAHL from January 2008 to June 2021 for U.S.-based studies evaluating the associations of interventions addressing one or more social risks with asthma-related emergency department visits and hospitalizations among children. The systematic review included 38 of the original 641 identified articles (6%), and the meta-analysis included 19 articles (3%). Overall, participation in social risk–based interventions, particularly those that addressed health literacy, home environmental conditions and peer support were associated with significantly reduced risks for asthma-related emergency department visits and hospitalizations among children.
You can read the full study, “Social Risk Interventions and Health Care Utilization for Pediatric Asthma: A Systematic Review and Meta-analysis” in JAMA Pediatrics.
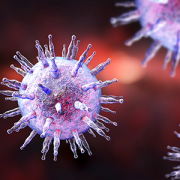
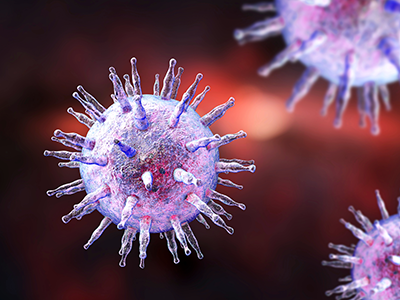
Epstein-Barr virus is a member of the herpes family and it spreads primarily through saliva.
Children’s National Hospital experts provided a contemporary description of the epidemiology, clinical presentation and management of chronic active Epstein-Barr virus (CAEBV), shedding light on this very rare disease. The paper, published in Blood Advances, assessed 57 patients outside of Asia — the biggest international retrospective cohort study published in the Western world.
Epstein-Barr virus is a member of the herpes family and it spreads primarily through saliva. Once a person is infected with Epstein-Barr virus, the immune system will control the infections, but the virus lies in a dormant state in the patient’s B Cells. However, in some patients, there is a failure of the body to control the infection, and the virus is found inside the patient’s T and/or NK cells. These rare patients are diagnosed with CAEBV. The hallmark of the disease is proliferation of Epstein-Barr virus-infected T or NK cells that infiltrate tissues, leading to end-organ damage. Patients most often experience fevers, hepatosplenomegaly, liver inflammation, cytopenias and lymphoproliferation that may progress to lymphoma.
Given it is most prevalent in Asia, little is known about the disease in the Western world. There has only been one published paper regarding the outcomes of patients in the U.S., which included 19 patients amassed over 28 years, and was published a decade ago.
Multiple treatments have been attempted to control the disease, but none have resulted in consistent remission. Historically, the consensus is to use steroids and/or antiviral drug in combination with proteasome inhibitor agents. In some cases, clinicians also use cytotoxic chemotherapy to reduce disease burden and improve the patient’s condition before HSCT. Still, this approach is limited because most patients die due to the progression of their disease despite these interventions.
Ultimately, most of these patients are referred for allogeneic hematopoietic stem cell transplantation (HSCT), which is the only known curative therapy for CAEBV. However, the best approach to control disease prior to HSCT, as well as the optimal conditioning regimen, are unknown.
“For the first time in many years, we provide insight on contemporary treatment options to consider for patients with CAEBV, as well as identifying risk factors for worse outcomes,” said Blachy Dávila Saldaña, M.D., blood and marrow transplant specialist at Children’s National and lead author of the study. “HSCT is curative, but patients need to be considered prior to the evolution of more advanced disease, particularly lymphoma. We also provide a new platform that will inform research on new interventions and therapies for this population.”
“CAEBV remains a challenging disorder to treat, especially once severe complications develop,” said Catherine Bollard, M.D., M.B.Ch.B., director of the Center for Cancer and Immunology Research at Children’s National. “However, our data suggests that T cell modulating therapies may enhance disease control, and future studies should address this question in a controlled setting.”
Future steps also include performing genetic studies to identify those at risk of developing the disease, and developing new platforms for treatment, including checkpoint inhibitors and cytotoxic lymphocyte therapies (CTL’s), which is a form of adoptive immunotherapy that employs virus-specific T cells.
The cohort includes patients treated in CNH and multiple institutions around the world, including Texas Children’s and the National Institutes of Health. “This work was only possible through our collaborative research in anti-EBV cellular therapies,” said Dr. Dávila.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/11/Epstein-Barr-virus-illustration.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-11-23 13:40:242024-11-27 09:40:12Study with largest cohort in the Western world sheds light on Epstein-Barr virus
When asked a simple “yes” or “no” question about food allergy-related bullying, 17% of kids said they’d been bullied, teased or harassed about their food allergy. But when asked to reply to a multi-item list of victimization behaviors, that number jumped to 31%.
Living with a food allergy can greatly impact a child’s everyday life – from limiting participation in social activities to being treated differently by peers. While previous research indicates many kids experience food allergy-related bullying, a new study in the Journal of Pediatric Psychology found that offering kids with food allergies a multi-question assessment gives a more accurate picture of the size and scope of the problem.
When asked a simple “yes” or “no” question about food allergy-related bullying, 17% of kids said they’d been bullied, teased or harassed about their food allergy. But when asked to reply to a multi-item list of victimization behaviors, that number jumped to 31%. Furthermore, Children’s National Hospital researchers found that only 12% of parents reported being aware of it.
The reported bullying ranged from verbal teasing or criticism to more overt acts such as an allergen being waved in their face or intentionally put in their food. Researchers say identifying accurate assessment methods for this problem are critical so children can get the help they need.
“Food allergy-related bullying can have a negative impact on a child’s quality of life. By using a more comprehensive assessment, we found that children with food allergies were bullied more than originally reported and parents may be in the dark about it,” says Linda Herbert, Ph.D., director of the Psychosocial Clinical and Research Program in the Division of Allergy and Immunology at Children’s National and one of the study’s researcher.
“The results of this study demonstrate a need for greater food allergy education and awareness of food allergy-related bullying among communities and schools where food allergy-related bullying is most likely to occur,” Herbert adds.
The study looked at food allergy-related bullying among a diverse patient population and evaluated parent-child disagreement and bullying assessment methods. It included 121 children and 121 primary caregivers who completed questionnaires. The children ranged in age from 9 to 15-years-old and were diagnosed by an allergist with at least one of the top eight IgE-mediated food allergies – peanut, tree nut, cow’s milk, egg, wheat, soy, shellfish and fish.
Of the 41 youth who reported food allergy-related bullying:
51% reported experiencing overt physical acts such as an allergen being waved in their face, thrown at them or intentionally put in their food.
66% reported bullying experiences that are categorized as non-physical overt victimization acts including verbal teasing, remarks or criticisms about their allergy and verbal threats or intimidation.
Eight reported relational bullying, such as rumors being spread, people speaking behind their back and being intentionally ignored or excluded due to their food allergy.
The researchers also note that food allergy bullying perpetrators included, but were not limited to, classmates and other students, and bullying most commonly occurred at school.
The authors found that only 12% of parents reported that their child had been bullied because of their food allergy and of those, 93% said their child had reported the bullying to them. Some parents reported they had been made fun of or teased themselves because of concerns about their child’s food allergy.
“It’s important to find ways for children to open up about food allergy-related bullying,” Herbert says. “Asking additional specific questions about peer experiences during clinic appointments will hopefully get children and caregivers the help and support they need.”
Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, under Award Number K23AI130184 and National Institute on Minority Health and Health Disparities, part of the National Institutes of Health, under Award Number P20MD000198. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
In a new observational study, researchers provide insight into key features distinguishing MIS-C patients to provide a more realistic picture of the burden of disease in the pediatric population and aid with the early detection of disease and treatment for optimal outcomes.
Multisystem Inflammatory Syndrome in Children (MIS-C) significantly affected more Black and Latino children than white children, with Black children at the highest risk, according to a new observational study of 124 pediatric patients treated at Children’s National Hospital in Washington, D.C. Researchers also found cardiac complications, including systolic myocardial dysfunction and valvular regurgitation, were more common in MIS-C patients who were critically ill. Of the 124 patients, 63 were ultimately diagnosed with MIS-C and were compared with 61 patients deemed controls who presented with similar symptoms but ultimately had an alternative diagnosis.
In the study, published in The Journal of Pediatrics, researchers provide insight into key features distinguishing MIS-C patients to provide a more realistic picture of the burden of disease in the pediatric population and aid with the early detection of disease and treatment for optimal outcomes. The COVID-linked syndrome has affected nearly 4,000 children in the United States in the past year. Early reports showed severe illness, substantial variation in treatment and mortality associated with MIS-C. However, this study demonstrated that with early recognition and standardized treatment, short-term mortality can be nearly eliminated.
“Data like this will be critical for the development of clinical trials around the long-term implications of MIS-C,” says Dr. Roberta DeBiasi, M.D., lead author and chief of the Division of Pediatric Infectious Diseases at Children’s National. “Our study sheds light on the demographic, clinical and biomarker features of this disease, as well as viral load and viral sequencing.”
Of the 63 children with MIS-C, 52% were critically ill, and additional subtypes of MIS-C were identified including those with and without still detectable virus, those with and without features meeting criteria for Kawasaki Disease, and those with and without detectable cardiac abnormalities. While median age (7.25 years) and sex were similar between the MIS-C cohort and control group, Black (46%) and Latino (35%) children were overrepresented in the MIS-C group, especially those who required critical care. Heart complications were also more frequent in children who became critically ill with MIS-C (55% vs. 28%). Findings also showed MIS-C patients demonstrated a distinct cytokine signature, with significantly higher levels of certain cytokines than those of controls. This may help in the understanding of what drives the disease and which potential treatments may be most effective.
In reviewing viral load and antibody biomarkers, researchers found MIS-C cases with detectable virus had a lower viral load than in primary SARS-CoV-2 infection cases, but similar to MIS-C controls who had alternative diagnoses, but who also had detectable virus. A larger proportion of patients with MIS-C had detectable SARS-CoV-2 antibodies than controls. This is consistent with current thinking that MIS-C occurs a few weeks after a primary COVID-19 infection as part of an overzealous immune response.
Viral sequencing was also performed in the MIS-C cohort and compared to cases of primary COVID-19 infection in the Children’s National geographic population. 88% of the samples analyzed fell into the GH clade consistent with the high frequency of the GH clade circulating earlier in the pandemic in the U.S. and Canada, and first observed in France.
“The fact that there were no notable sequencing differences between our MIS-C and primary COVID cohorts suggests that variations in host genetics and/or immune response are more likely primary determinants of how MIS-C presents itself, rather than virus-specific factors,” says Dr. DeBiasi. “As we’ve seen new variants continue to emerge, it will be important to study their effect on the frequency and severity of MIS-C.”
Researchers are still looking for consensus on the most efficacious treatments for MIS-C. In a recent editorial in the New England Journal of Medicine, Dr. DeBiasi calls for well-characterized large prospective cohort studies at single centers, and systematic and long-term follow-up for cardiac and non-cardiac outcomes in children with MIS-C. Data from these studies will be a crucial determinant of the best set of treatment guidelines for immunotherapies to treat MIS-C.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/06/little-boy-at-doctors.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-06-25 11:34:002021-07-28 11:56:16Demographic, clinical and biomarker features of MIS-C
Children’s National Hospital in Washington, D.C., was ranked in the top 10 nationally in the U.S. News & World Report 2021-22 Best Children’s Hospitals annual rankings. This marks the fifth straight year Children’s National has made the Honor Roll list, which ranks the top 10 children’s hospitals nationwide. In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fifth year in a row.
For the eleventh straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“It is always spectacular to be named one of the nation’s best children’s hospitals, but this year more than ever,” says Kurt Newman, M.D., president and CEO of Children’s National. “Every member of our organization helped us achieve this level of excellence, and they did it while sacrificing so much in order to help our country respond to and recover from the COVID-19 pandemic.”
“When choosing a hospital for a sick child, many parents want specialized expertise, convenience and caring medical professionals,” said Ben Harder, chief of health analysis and managing editor at U.S. News. “The Best Children’s Hospitals rankings have always highlighted hospitals that excel in specialized care. As the pandemic continues to affect travel, finding high-quality care close to home has never been more important.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/06/US-NewsTriple-Badge-2021-400x300-1.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-06-15 01:00:392024-12-30 12:48:18For fifth year in a row, Children’s National Hospital nationally ranked a top 10 children’s hospital
Adolescents reported that epinephrine auto-injectors were frequently available, but least likely to be present outside of the home or school.
Severe food allergic reactions can be life-threatening or fatal and are experienced by up to 40% of children with food allergies, with adolescents at greatest risk. To assess early adolescents’ food allergy self-management, Linda Herbert, Ph.D., and her colleagues at Children’s National Hospital, had 101 adolescents ages 10-14 years complete the Food Allergy Management 24-Hour Recall as an interview.
Adolescents reported that epinephrine auto-injectors were frequently available, but least likely to be present outside of the home or school. Adolescents also relied on past experience with food to determine safety, which is not a recommended strategy. Appropriate assessment of food safety and problem-solving involving how to keep epinephrine auto-injectors with adolescents outside the home should be primary intervention targets.
Parents of young children with newly diagnosed food allergy are at risk for poor psychosocial outcomes due to food allergy’s life-threatening nature and demanding management routines. Presently, there are no interventions to support food allergy parents during this adjustment phase.
Ashley Ramos, Ph.D., and colleagues at Children’s National Hospital conducted a pilot study to explore the feasibility, acceptability and preliminary efficacy of a novel intervention using peer mentorship to improve psychosocial functioning in parents of young children with newly diagnosed food allergy. Parent mentors were trained in mentorship and matched with a mentee, a parent of a child under the age of 5 years with newly diagnosed food allergy, for a 6-month intervention period.
Their findings indicate the use of a peer mentorship program to support parents of children with newly diagnosed food allergy is feasible and helpful. It may be appropriate to develop and implement such programs in allergy clinics.
Study authors from Children’s National include: Ashley Ramos, Ph.D., Frances Cooke, Emily Miller and Linda Herbert, Ph.D.
Seven clinical sites in six different cities will join forces to perform mechanistic and translational studies examining the basic immunology of pediatric asthma among urban, under-resourced and largely minority children and adolescents.
The National Institute of Allergy and Infectious Diseases (NIAID) allocated $10 million in funding to establish the Childhood Asthma in the Urban Setting (CAUSE) network. The NIAID plans to increase this number by $70 million over seven years to support the network. Children’s National Hospital will be part of the new research network, which is a 7-year consortium comprising of seven clinical sites in six different cities that will join forces to perform mechanistic and translational studies examining the basic immunology of pediatric asthma among urban, under-resourced and largely minority children and adolescents.
Children’s National is the home of Improving Pediatric Asthma Care in the District of Columbia (IMPACT DC). The program focuses on research, care and advocacy to decrease asthma morbidity experienced by at-risk youth in the region while serving as a model program for the nation. NIAID gave an initial $3 million to IMPACT DC to conduct its own pilot study of anti-IgE therapy to prevent asthma exacerbations. Additional support for this and other studies will come from subcontracts from the CAUSE Coordinating Center at the University of Wisconsin in Madison.
“This new award allows IMPACT DC to remain part of one of the nation’s most prestigious pediatric asthma research consortia,” said Stephen Teach, M.D, M.P.H., chair for the Department of Pediatrics at George Washington University School of Medicine and Health Sciences. “It will allow us to both pursue an independent research agenda while collaborating with similar academic centers nationwide.”
Pediatric asthma is the most common chronic disease in children, and it is estimated that about 6.1 million children under 18 years suffer from this condition. It disproportionately affects urban, minority and under-resourced children and adolescents.
“It is essential to develop an understanding of the basic immunology of the disease and therapeutic options to ameliorating these disparities,” said Dr. Teach.
CAUSE researchers will explore the mechanisms of immune tolerance to allergens, the role of early environmental exposures in the pathogenesis of asthma, the pathogenesis and mechanisms of non-atopic asthma, the role of the respiratory epithelium in asthma and more.
The CAUSE network comprises of seven clinical research centers, including Children’s National led by principal investigator, Dr. Teach, and the following research centers:
Boston Children’s Hospital. Principal investigators: Wanda Phipatanakul, M.D., and Talal Chatila, M.D.
Cincinnati Children’s Hospital Medical Center. Principal investigator: Gurjit Khurana Hershey, M.D., Ph.D.
Columbia University Health Sciences, New York. Principal investigator: Meyer Kattan, M.D.
Icahn School of Medicine at Mount Sinai, New York. Principal investigators: Paula Busse, M.D., Supinda Bunyavanich, M.D., and Juan Wisnivesky, M.D.
Lurie Children’s Hospital of Chicago. Principal investigators: Rajesh Kumar, M.D., and Jacqueline Pongracic, M.D.
University of Colorado Denver. Principal investigator: Andrew Liu, M.D.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/04/girl-with-asthma-inhaler.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-04-26 10:40:312024-09-06 15:08:14Children’s National becomes part of CAUSE Network
Ongoing efforts by researchers at Children’s National Hospital to improve T-cell therapies have led to a spin-out company MANA Therapeutics which has announced a $35 million Series A financing. MANA is a clinical stage company creating nonengineered, allogeneic and off-the-shelf cell therapies that target multiple cancer antigens. Its EDIFY™ platform aims to educate T-cells that target multiple target multiple cell surface and intracellular tumor-associated antigens across a broad range of liquid and solid tumors, with an initial focus on relapsed acute myeloid leukemia (AML).
MANA was founded in 2017, and was based on the research and human proof-of-concept clinical trials conducted by Catherine Bollard, M.D., M.B.Ch.B., Conrad Russell Y. Cruz, M.D., Ph.D., Patrick Hanley, Ph.D. and other investigators at Children’s National along with their colleagues at Johns Hopkins Medical Center. The trials demonstrated safety and anti-tumor activity of MANA’s approach, and Children’s National provided an exclusive license to MANA to further develop this promising technology into commercial products in the field of immuno-oncology.
MANA Therapeutics recruited an experienced leadership team from industry including Martin B. Silverstein, M.D., president and CEO, who is a former senior executive at Gilead Sciences when they acquired Kite Pharma, one of the leading cell therapy companies, as well as Madhusudan V. Peshwa, Ph.D., chief technology officer, who joined from GE Health Care where he had been Chief Technology Officer and Global Head of R&D for Cell and Gene Therapies.
“MANA is building upon the strong foundational science established at Children’s National with a unique approach that promises to produce off-the-shelf allogeneic therapies that do not compromise on safety or efficacy,” said Marc Cohen, co-founder and executive chairman of MANA Therapeutics. “I look forward to continuing to support the MANA team as they advance their internal pipeline for the treatment of AML and select solid tumors, and expand the potential of EDIFY through strategic partnerships focused on new target antigens and cancer types.”
An international leader in the immunotherapy field, Dr. Bollard was an early believer in the potential of immune cell therapies to dramatically improve the treatment of patients with cancer and patients with life-threatening viral infections. Recently, she and her team at the Children’s National Center for Cancer and Immunology Researchpublished findings in Blood showing T-cells taken from the blood of people who recovered from a COVID-19 infection can be successfully multiplied in the lab and maintain the ability to effectively target proteins that are key to the virus’s function.
“Over the past decade we have seen tremendous progress in cancer research and treatment and are beginning to unlock the potential of cell therapy for a variety of tumor types,” said Dr. Bollard. “The human proof-of-concept trials conducted by my team and colleagues showed potential for a nonengineered approach to educating T-cells to attack multiple tumor antigens, which MANA is expanding even further through refinement of the manufacturing process for an allogeneic product and application to a broader set of antigens in a variety of clinical indications and settings.”
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/02/t-cells-attacking-cancer-cell.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-02-11 16:11:442024-10-29 15:39:54Children’s National spin-out cell therapy company receives funding
Pediatric food allergy is a growing public health concern, with 8 percent of children in the United States affected. Although new treatments for food allergies are being developed, the vast majority of cases are currently managed by daily evaluation of food safety and vigilance for accidental allergen exposure and allergic reactions. This often impacts patients’ and caregivers’ quality of life and overall psychosocial functioning.
In a recent article published in the Journal of Allergy and Clinical Immunology: In Practice, Linda Herbert, Ph.D., and Audrey DunnGalvin, Ph.D., provide a review of mental health concerns related to food allergy. The authors present two cases in which patients received psychological services for food allergy-related anxiety. For both cases, treatment resulted in decreased anxiety and improved food allergy management/oral immunotherapy treatment engagement.
The authors also discuss unmet food allergy-related psychosocial needs, including the lack of food allergy-specific anxiety measures, psychosocial domains that warrant investigation, development of supportive interventions for patients engaging in allergen immunotherapy and the lack of adequate mental health providers with food allergy expertise.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2021/01/common-food-allergens.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-01-27 14:19:422021-01-27 14:21:56Psychotherapeutic treatment for psychosocial concerns related to food allergy
Food allergy is a major public health concern in many countries around the world. In the United States, studies suggest that it affects up to 8% of children and 10% of adults and is responsible for an emergency room admission every three minutes. Historically, the only treatment for food allergy has been complete allergen avoidance combined with rescue medications when accidental exposures occur. Fortunately, advances in food allergy research over the past decade have yielded new treatments, but with these new treatments come new stressors.
In a recent study published in the journal Current Treatment Options in Allergy, Linda Herbert, Ph.D., and colleagues provide an overview of the current state of the literature regarding patients’ and caregivers’ food allergy experiences and needs within the United States. The authors also put forth a set of recommendations regarding how best to proceed with patient-centered development and evaluation of new food allergy treatments.
“The past year has been a stark reminder about the importance of partnership and working together toward common goals,” says Dr. Beers. “I am humbled and honored to be taking on this role at such a pivotal moment for the future health and safety of not only children, but the community at large.”
Lee Savio Beers, M.D., F.A.A.P., medical director of Community Health and Advocacy at the Child Health Advocacy Institute (CHAI) at Children’s National Hospital, has begun her term as president of the American Academy of Pediatrics (AAP). The AAP is an organization of 67,000 pediatricians committed to the optimal physical, mental and social health and well-being for all children – from infancy to adulthood.
“The past year has been a stark reminder about the importance of partnership and working together toward common goals,” says Dr. Beers. “I am humbled and honored to be taking on this role at such a pivotal moment for the future health and safety of not only children, but the community at large.”
Dr. Beers has pledged to continue AAP’s advocacy and public policy efforts and to further enhance membership diversity and inclusion. Among her signature issues:
Partnering with patients, families, communities, mental health providers and pediatricians to co-design systems to bolster children’s resiliency and to alleviate growing pediatric mental health concerns.
Continuing to support pediatricians during the COVID-19 pandemic with a focus on education, pediatric practice support, vaccine delivery systems and physician wellness.
Dr. Beers is looking forward to continuing her work bringing together the diverse voices of pediatricians, children and families as well as other organizations to support improving the health of all children.
“Dr. Beers has devoted her career to helping children,” says Kurt Newman, M.D., president and chief executive officer of Children’s National. “She has developed a national advocacy platform for children and will be of tremendous service to children within AAP national leadership.”
Read more about Dr. Beer’s career and appointment as president of the AAP.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/09/Lee-Beers.jpg400300Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2021-01-04 11:10:372023-07-03 10:51:37Lee Beers, M.D., F.A.A.P, begins term as AAP president
Children’s National Hospital announced a $5 million gift from The Boeing Company that will help drive lifesaving pediatric discoveries at the new Children’s National Research & Innovation Campus.
Children’s National Hospital announced a $5 million gift from The Boeing Company that will help drive lifesaving pediatric discoveries at the new Children’s National Research & Innovation Campus. The campus, now under construction, is being developed on nearly 12 acres of the former Walter Reed Army Medical Center. Children’s National will name the main auditorium in recognition of Boeing’s generosity.
“We are deeply grateful to Boeing for their support and commitment to improving the health and well-being of children in our community and around the globe,” said Kurt Newman, M.D., president and CEO of Children’s National “The Boeing Auditorium will help the Children’s National Research & Innovation campus become the destination for discussion about how to best address the next big healthcare challenges facing children and families.”
The one-of-a-kind pediatric hub will bring together public and private partners for unprecedented collaborations. It will accelerate the translation of breakthroughs into new treatments and technologies to benefit kids everywhere.
“Children’s National Hospital’s enduring mission of positively impacting the lives of our youngest community members is especially important today,” said Boeing President and CEO David Calhoun. “We’re honored to join other national and community partners to advance this work through the establishment of their Research & Innovation Campus.”
Children’s National Research & Innovation Campus partners currently include Johnson & Johnson Innovation – JLABS, Virginia Tech, the National Institutes of Health (NIH), Food & Drug Administration (FDA), U.S. Biomedical Advanced Research and Development Authority (BARDA), Cerner, Amazon Web Services, Microsoft, National Organization of Rare Diseases (NORD) and local government.
The 3,200 square-foot Boeing Auditorium will be the focal point of the state-of-the-art conference center on campus. Nationally renowned experts will convene with scientists, medical leaders and diplomats from around the world to foster collaborations that spur progress and disseminate findings.
Boeing’s $5 million commitment deepens its longstanding partnership with Children’s National. The company has donated nearly $2 million to support pediatric care and research at Children’s National through Chance for Life and the hospital’s annual Children’s Ball. During the coronavirus pandemic, Boeing fabricated and donated 2,000 face shields to help keep patients and frontline care providers at Children’s National safe.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/02/Research-Innovation-Campus.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-11-05 11:16:312023-07-03 10:40:51Boeing gives $5 million to support Research & Innovation Campus
Children’s National Hospital in Washington, D.C., was ranked No. 7 nationally in the U.S. News & World Report 2020-21 Best Children’s Hospitals annual rankings. This marks the fourth straight year Children’s National has made the list, which ranks the top 10 children’s hospitals nationwide.
In addition, its neonatology program, which provides newborn intensive care, ranked No.1 among all children’s hospitals for the fourth year in a row.
For the tenth straight year, Children’s National also ranked in all 10 specialty services, with seven specialties ranked in the top 10.
“Our number one goal is to provide the best care possible to children. Being recognized by U.S. News as one of the best hospitals reflects the strength that comes from putting children and their families first, and we are truly honored,” says Kurt Newman, M.D., president and CEO of Children’s National Hospital.
“This year, the news is especially meaningful, because our teams — like those at hospitals across the country — faced enormous challenges and worked heroically through a global pandemic to deliver excellent care.”
“Even in the midst of a pandemic, children have healthcare needs ranging from routine vaccinations to life-saving surgery and chemotherapy,” said Ben Harder, managing editor and chief of Health Analysis at U.S. News. “The Best Children’s Hospitals rankings are designed to help parents find quality medical care for a sick child and inform families’ conversations with pediatricians.”
The annual rankings are the most comprehensive source of quality-related information on U.S. pediatric hospitals. The rankings recognize the nation’s top 50 pediatric hospitals based on a scoring system developed by U.S. News. The top 10 scorers are awarded a distinction called the Honor Roll.
The bulk of the score for each specialty service is based on quality and outcomes data. The process includes a survey of relevant specialists across the country, who are asked to list hospitals they believe provide the best care for patients with the most complex conditions.
Below are links to the seven Children’s National specialty services that U.S. News ranked in the top 10 nationally:
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/06/US-News-2020-ID.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-06-16 01:00:292024-12-30 12:50:15Children’s National ranked a top 10 children’s hospital and No. 1 in newborn care nationally by U.S. News
Children’s National Research Institute directors Vittorio Gallo, Ph.D., and Mark Batshaw, M.D.
The Children’s National Research Institute recently released its 2019-2020 academic annual report, titled 150 Years Stronger Through Discovery and Care to mark the hospital’s 150th birthday. Not only does the annual report give an overview of the institute’s research and education efforts, but it also gives a peek in to how the institute has mobilized to address the coronavirus pandemic.
“Our inaugural research program in 1947 began with a budget of less than $10,000 for the study of polio — a pressing health problem for Washington’s children at the time and a pandemic that many of us remember from our own childhoods,” says Vittorio Gallo, Ph.D., chief research officer at Children’s National Hospital and scientific director at Children’s National Research Institute. “Today, our research portfolio has grown to more than $75 million, and our 314 research faculty and their staff are dedicated to finding answers to many of the health challenges in childhood.”
Highlights from the Children’s National Research Institute annual report
In 2018, Children’s National began construction of its new Research & Innovation Campus (CNRIC) on 12 acres of land transferred by the U.S. Army as part of the decommissioning of the former Walter Reed Army Medical Center campus. In 2020, construction on the CNRIC will be complete, and in 2012, the Children’s National Research Institute will begin to transition to the campus.
In late 2019, a team of scientists led by Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, traveled to the Democratic Republic of Congo to collect samples from 60 individuals that will form the basis of a new reference genome data set. The researchers hope their project will generate better reference genome data for diverse populations, starting with those of Central African descent.
A gift of $5.7 million received by the Center for Translational Research’s director, Lisa Guay-Woodford, M.D., will reinforce close collaboration between research and clinical care to improve the care and treatment of children with polycystic kidney disease and other inherited renal disorders.
The Center for Neuroscience Research’s integration into the infrastructure of Children’s National Hospital has created a unique set of opportunities for scientists and clinicians to work together on pressing problems in children’s health.
Children’s National and the National Institute of Allergy and Infectious Diseases are tackling pediatric research across three main areas of mutual interest: primary immune deficiencies, food allergies and post-Lyme disease syndrome. Their shared goal is to conduct clinical and translational research that improves what we know about those conditions and how we care for children who have them.
An immunotherapy trial has allowed a little boy to be a kid again. In the two years since he received cellular immunotherapy, Matthew has shown no signs of a returning tumor — the longest span of time he’s been tumor-free since age 3.
In the past 6 years, the 104 device projects that came through the National Capital Consortium for Pediatric Device Innovation accelerator program raised $148,680,256 in follow-on funding.
Even though he’s watched more than 500 aspiring physicians pass through the Children’s National pediatric residency program, program director Dewesh Agrawal, M.D., still gets teary at every graduation.
Understanding and treating the novel coronavirus (COVID-19)
In a short period of time, Children’s National Research Institute has mobilized its scientists to address COVID-19, focusing on understanding the virus and advancing solutions to ameliorate the impact today and for future generations. Children’s National Research Institute Director Mark Batshaw, M.D., highlighted some of these efforts in the annual report:
Eric Vilain, M.D., Ph.D., director of the Center for Genetic Medicine Research, is looking at whether or not the microbiome of bacteria in the human nasal tract acts as a defensive shield against COVID-19.
Catherine Bollard, M.D., MBChB, director of the Center for Cancer and Immunology Research, and her team are seeing if they can “train” T cells to attack the invading coronavirus.
Sarah Mulkey, M.D., Ph.D., an investigator in the Center for Neuroscience Research and the Fetal Medicine Institute, is studying the effects of, and possible interventions for, coronavirus on the developing brain.
You can view the entire Children’s National Research Institute academic annual report online.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/05/Vittorio-Gallo-and-Marc-Batshaw.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-05-19 14:08:392024-06-28 13:19:46Children’s National Research Institute releases annual report
Children’s National Hospital collects patients’ blood, extracts T-cells and replicates them in the presence of specific proteins found on cancer cells which, in essence, teaches the T-cells to target specific tumor markers. Training the T-cells, growing them to sufficient quantities and ensuring they are safe for administration takes weeks. But when patients return to the outpatient clinic, their T-cell infusion lasts just a few minutes.
For the third consecutive year, Children’s National was selected to compete in STAT Madness, an annual bracket-style competition that chooses the year’s most impactful biomedical innovation by popular vote. Children’s entry, “Immunotherapy of relapsed and refractory solid tumors with ex vivo expanded multi-tumor associated antigen specific cytotoxic T lymphocytes,” uses the body’s own immune system to attack and eliminate cancer cells in pediatric and adult patients with solid tumor malignancies.
In 2018, Children’s first-ever STAT Madness entry advanced through five brackets in the national competition and, in the championship round, finished second. That innovation, which enables more timely diagnoses of rare diseases and common genetic disorders, helping to improve kids’ health outcomes around the world, also was among four “Editor’s Pick” finalists, entries that spanned a diverse range of scientific disciplines.
An estimated 11,000 new cases of pediatric cancer were diagnosed in children 14 and younger in the U.S. in 2019. And, when it comes to disease, cancer remains the leading cause of death among children, according to the National Institutes of Health. An enterprising research team led by Children’s National faculty leveraged T-cells – essential players in the body’s immune system – to treat pediatric and adult patients with relapsed or refractory solid tumors who had exhausted all other therapeutic options.
“We’re using the patient’s own immune system to fight their cancer, rather than more traditional chemotherapy drugs,” says Catherine M. Bollard, M.D., director of the Center for Cancer & Immunology Research at Children’s National and co-senior author of the study. “It’s more targeted and less toxic to the patient. These T-cells home in on any cancer cells that might be in the body, allowing healthy cells to continue to grow,” Dr. Bollard adds.
That means patients treated in the Phase I, first-in-human trial didn’t lose their hair and weren’t hospitalized for the treatment. After a quick clinical visit for their treatment, they returned to normal activities, like school, with good energy levels.
“With our specially trained T-cell therapy, many patients who previously had rapidly progressing disease experienced prolonged disease stabilization,” says Holly J. Meany, M.D., a Children’s National oncologist and the study’s co-senior author. “Patients treated at the highest dose level showed the best clinical outcomes, with a six-month, progression-free survival of 73% after tumor-associated antigen cytotoxic T-cell (TAA-T) infusion, compared with 38% with their immediate prior therapy.”
The multi-institutional team published their findings from the study online July 29, 2019, in the Journal of Clinical Oncology.
“Our research team and our parents are delighted that some patients treated in our study continue to do well following T-cell therapy without additional treatment. In some cases, two years after treatment, patients do not appear to have active disease and are maintaining an excellent quality of life,” says Amy B. Hont, M.D., the study’s lead author. “One of these was a patient whose parents were told his only other option was palliative care. Our innovation gives these families new hope,” Dr. Hont adds.
The 2020 STAT Madness #Core64 bracket opened March 2, and the champion will be announced April 6.
In addition to Drs. Hont, Meany and Bollard, Children’s National co-authors include C. Russell Cruz, M.D., Ph.D., Robert Ulrey, MS, Barbara O’Brien, BS, Maja Stanojevic, M.D., Anushree Datar, MS, Shuroug Albihani, MS, Devin Saunders, BA, Ryo Hanajiri, M.D., Ph.D., Karuna Panchapakesan, MS, Payal Banerjee, MS, Maria Fernanda Fortiz, BS, Fahmida Hoq, MBBS, MS, Haili Lang, M.D., Yunfei Wang, DrPH, Patrick J. Hanley, Ph.D., and Jeffrey S. Dome, M.D., Ph.D.; and Sam Darko, MS, National Institute of Allergy and Infectious Diseases.
Financial support for the research described in this post was provided by the Children’s National Hospital Heroes Gala, Alex’s Army Foundation, the Children’s National Board of Visitors and Hyundai Hope on Wheels Young Investigator Grant to Support Pediatric Cancer Research, the Children’s National Research Institute Bioinformatics Unit, the Clinical and Translational Science Institute and the National Institutes of Health under award No. UL1-TR001876.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2020/03/STAT-Madness-vote-small.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2020-03-04 09:57:002024-06-12 17:03:24It’s a three-peat! Children’s National again competes in STAT Madness
After a teen was transferred to Children’s National Hospital suffering from severe difficulty breathing and swallowing, a multidisciplinary team continued the detective work and surmises that vaping was to blame for her unusual symptoms.
A teenage girl with no hint of prior asthma or respiratory illness began to feel hoarseness in her throat and a feeling that she needed to clear her throat frequently. Within a few weeks, her hoarseness and throat-clearing worsened with early morning voice loss and feeling as if food were lodged in her throat. She started having trouble swallowing and began to avoid food all together.
Her pediatrician prescribed loratadine for suspected allergies to no avail. Days later, an urgent care center prescribed a three-day course of prednisone. For a few days, she felt a little better, but went back to feeling like she was breathing “through a straw.” After going to an emergency room with acute respiratory distress and severe difficulty swallowing, staff tried intravenous dexamethasone, ampicillin/sulbactam, and inhaled racemic epinephrine and arranged for transfer.
When she arrived at Children’s National Hospital, a multidisciplinary team continued the detective work with additional testing, imaging and bloodwork.
Examining her throat confirmed moderate swelling and a partially obstructed airway draped with thick chartreuse-colored mucus. The teen had no history of an autoimmune disorder, no international travel and no exposure to animals. She had no fever and had received all her scheduled immunizations.
“With epiglottitis – an inflammation of the flap found at the base of the tongue that prevents food from entering the trachea – our first concern is that an underlying infection is to blame,” says Michael Jason Bozzella, D.O., MS, a third-year infectious diseases fellow and lead author of the case report published Feb. 5, 2020, in Pediatrics. “We tested her specimens in a number of ways for a host of respiratory pathogens, including human rhino/enterovirus, respiratory syncytial virus, influenza, Epstein-Barr virus, Streptococcus and more. All negative. We also looked for more atypical infections with bacteria, like Arcanobacterium, Mycoplasma and Gonorrhea. Those were all negative as well,” Dr. Bozzella adds.
She slowly improved during a seven-day initial hospital stay, though soon returned for another six-day hospital stay after it again became excruciatingly painful for her to swallow.
Every throat culture and biopsy result showed no evidence of fungal, bacterial or viral infection, acid-fast bacilli or other malignancy. But in speaking with doctors, the teen had admitted to using candy-and fruit-flavored e-cigarettes three to five times with her friends over the two months preceding her symptoms. The last time she vaped was two weeks before her unusual symptoms began.
According to the Centers for Disease Control and Prevention, 2,668 people in the U.S. have been hospitalized for e-cigarette or vaping product use-associated lung injury, as of Jan. 14, 2020. The Children’s National case report’s authors say the increasing use of vaping products by teenagers highlights the potential for unknown health risks to continue to grow.
“This teenager’s use of e-cigarettes is the most plausible reason for this subacute epiglottitis diagnosis, a condition that can become life-threatening,” says Kathleen Ferrer, M.D., a hospitalist at Children’s National and the case report’s senior author. “This unusual case adds to a growing list of toxic effects attributable to vaping. While we normally investigate infectious triggers, like Streptococci, Staphylococci and Haemophilus, we and other health care providers should also consider e-cigarettes as we evaluate oro-respiratory complaints.”
Children allergic to cow’s milk are smaller and weigh less, according to the first published study to characterize growth trajectories from early childhood to adolescence in children with persistent food allergies.
Children who are allergic to cow’s milk are smaller and weigh less than peers who have allergies to peanuts or tree nuts, and these findings persist into early adolescence. The results from the longitudinal study – believed to be the first to characterize growth patterns from early childhood to adolescence in children with persistent food allergies – was published online in The Journal of Allergy and Clinical Immunology.
“Published data about growth trajectories for kids with ongoing food allergies is scarce,” says Karen A. Robbins, M.D.,* lead study author and an allergist in the Division of Allergy and Immunology at Children’s National Hospital when the study was conducted. “It remains unclear how these growth trends ultimately influence how tall these children will become and how much they’ll weigh as adults. However, our findings align with recent research that suggests young adults with persistent cow’s milk allergy may not reach their full growth potential,” Dr. Robbins says.
According to the Centers for Disease Control and Prevention, 1 in 13 U.S. children has a food allergy with milk, eggs, fish, shellfish, wheat, soy, peanuts and tree nuts accounting for the most serious allergic reactions. Because there is no cure and such allergies can be life-threatening, most people eliminate one or more major allergen from their diets.
The multi-institutional research team reviewed the charts of pediatric patients diagnosed with persistent immunoglobulin E-mediated allergy to cow’s milk, peanuts or tree nuts based on their clinical symptoms, food-specific immunoglobulin levels, skin prick tests and food challenges. To be included in the study, the children had to have at least one clinical visit during three defined time frames from the time they were age 2 to age 12. During those visits, their height and weight had to be measured with complete data from their visit available to the research team. The children allergic to cow’s milk had to eliminate it completely from their diets, even extensively heated milk.
From November 1994 to March 2015, 191 children were enrolled in the study, 111 with cow’s milk allergies and 80 with nut allergies. All told, they had 1,186 clinical visits between the ages of 2 to 12. Sixty-one percent of children with cow’s milk allergies were boys, while 51.3% of children with peanut/tree nut allergies were boys.
In addition to children allergic to cow’s milk being shorter, the height discrepancy was more pronounced by ages 5 to 8 and ages 9 to 12. And, for the 53 teens who had clinical data gathered after age 13, differences in their weight and height were even more notable.
“As these children often have multiple food allergies and other conditions, such as asthma, there are likely factors besides simply avoiding cow’s milk that may contribute to these findings. These children also tend to restrict foods beyond cow’s milk,” she adds.
The way such food allergies are handled continues to evolve with more previously allergic children now introducing cow’s milk via baked goods, a wider selection of allergen-free foods being available, and an improving understanding of the nutritional concerns related to food allergy.
Dr. Robbins cautions that while most children outgrow cow’s milk allergies in early childhood, children who do not may be at risk for growth discrepancies. Future research should focus on improving understanding of this phenomenon.
In addition to Dr. Robbins, the research team includes co-author Robert A. Wood, M.D., and senior author Corinne A. Keet, M.D., Ph.D., both of Johns Hopkins University School of Medicine.
*Dec. 18, 2019 update: After leaving full-time employment at Children’s National Hospital, Dr. Robbins became an AstraZeneca employee, working on immuno-oncology safety.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/12/little-girl-drinking-milk.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-12-16 18:40:242025-02-28 12:24:07Children allergic to cow’s milk smaller and lighter
Recently, Kurt Newman, M.D., president and CEO of Children’s National Hospital, authored an opinion piece for the popular political website, The Hill. In the article, he called upon stakeholders from across the landscape to address the significant innovation gap in children’s healthcare versus adults.
As Chair of the Board of Trustees of the Children’s Hospital Association, Dr. Newman knows the importance of raising awareness among policy makers at the federal and state level about the healthcare needs of children. Dr. Newman believes that children’s health should be a national priority that is addressed comprehensively. With years of experience as a pediatric surgeon, he is concerned by the major inequities in the advancements of children’s medical devices and technologies versus those for adults. That’s why Children’s National is working to create collaborations, influence policies and facilitate changes that will accelerate the pace of pediatric healthcare innovation for the benefit of children everywhere. One way that the hospital is tackling this challenge is by developing the Children’s National Research & Innovation Campus, which will be the nation’s first innovation campus focused on pediatric research.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2018/02/Kurt-Newman-capitol-building.jpg300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-12-11 15:41:002023-07-10 10:07:22Making healthcare innovation for children a priority
Children’s National Hospital and Virginia Tech create formal partnership that includes the launch of a Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus.
Children’s National Hospital and Virginia Tech recently announced a formal partnership that will include the launch of a 12,000-square-foot Virginia Tech biomedical research facility within the new Children’s National Research & Innovation Campus. The campus is an expansion of Children’s National that is located on a nearly 12-acre portion of the former Walter Reed Army Medical Center in Washington, D.C. and is set to open its first phase in December 2020. This new collaboration brings together Virginia Tech, a top tier academic research institution, with Children’s National, a U.S. News and World Report top 10 children’s hospital, on what will be the nation’s first innovation campus focused on pediatric research.
“Virginia Tech is an ideal partner to help us deliver on what we promised for the Children’s National Research & Innovation Campus – an ecosystem that enables us to accelerate the translation of potential breakthrough discoveries into new treatments and technologies,” says Kurt Newman, M.D., president and CEO, Children’s National. “Our clinical expertise combined with Virginia Tech’s leadership in engineering and technology, and its growing emphasis on biomedical research, will be a significant advance in developing much needed treatment and cures to save children’s lives.”
Earlier this year, Children’s National announced a collaboration with Johnson & Johnson Innovation LLC to launch JLABS @ Washington, DC at the Research & Innovation Campus. The JLABS @ Washington, DC site will be open to pharmaceutical, medical device, consumer and health technology companies that are aiming to advance the development of new drugs, medical devices, precision diagnostics and health technologies, including applications in pediatrics.
“We are proud to welcome Virginia Tech to our historic Walter Reed campus – a campus that is shaping up to host some of the top minds, talent and innovation incubators in the world,” says Washington, D.C. Mayor Muriel Bowser. “The new Children’s National Research & Innovation Campus will exemplify why D.C. is the capital of inclusive innovation – because we are a city committed to building the public and private partnerships necessary to drive discoveries, create jobs, promote economic growth and keep D.C. at the forefront of innovation and change.”
Faculty from the Children’s National Research Institute and the Fralin Biomedical Research Institute at Virginia Tech Carilion (VTC) have worked together for more than a decade, already resulting in shared research grants, collaborative publications and shared intellectual property. Together, the two institutions will now expand their collaborations to develop new drugs, medical devices, software applications and other novel treatments for cancer, rare diseases and other disorders.
“Joining with Children’s National in the nation’s capital positions Virginia Tech to improve the health and well-being of infants and children around the world,” says Virginia Tech President Tim Sands, Ph.D. “This partnership resonates with our land-grant mission to solve big problems and create new opportunities in Virginia and D.C. through education, technology and research.”
The partnership with Children’s National adds to Virginia Tech’s growing footprint in the Washington D.C. region, which includes plans for a new graduate campus in Alexandria, Va. with a human-centered approach to technological innovation. Sands said the proximity of the two locations – just across the Potomac – will enable researchers to leverage resources, and will also create opportunities with the Virginia Tech campus in Blacksburg, Va. and the Virginia Tech Carilion Health Science and Technology campus in Roanoke, Va.
Carilion Clinic and Children’s National have an existing collaboration for provision of certain specialized pediatric clinical services. The more formalized partnership between Virginia Tech and Children’s National will drive the already strong Virginia Tech-Carilion Clinic partnership, particularly for children’s health initiatives and facilitate collaborations between all three institutions in the pediatric research and clinical service domains.
Children’s National and Virginia Tech will engage in joint faculty recruiting, joint intellectual property, joint training of students and fellows, and collaborative research projects and programs according to Michael Friedlander, Ph.D., Virginia Tech’s vice president for health sciences and technology, and executive director of the Fralin Biomedical Research Institute at VTC.
“The expansion and formalization of our partnership with Children’s National is extremely timely and vital for pediatric research innovation and for translating these innovations into practice to prevent, treat and ultimately cure nervous system cancer in children,” says Friedlander, who has collaborated with Children’s National leaders and researchers for more than 20 years. “Both Virginia Tech and Children’s National have similar values and cultures with a firm commitment to discovery and innovation in the service of society.”
“Brain and other nervous system cancers are among the most common cancers in children (alongside leukemia),” says Friedlander. “With our strength in neurobiology including adult brain cancer research in both humans and companion animals at Virginia Tech and the strength of Children’s National research in pediatric cancer, developmental neuroscience and intellectual disabilities, this is a perfect match.”
The design of the Children’s National Research & Innovation Campus not only makes it conducive for the hospital to strengthen its prestigious partnerships with Virginia Tech and Johnson & Johnson, it also fosters synergies with federal agencies like the Biomedical Advanced Research and Development Authority, which will collaborate with JLABS @ Washington, DC to establish a specialized innovation zone to develop responses to health security threats. As more partners sign on, this convergence of key public and private institutions will accelerate discoveries and bring them to market faster for the benefit of children and adults.
“The Children’s National Research & Innovation Campus pairs an inspirational mission to find new treatments for childhood illness and disease with the ideal environment for early stage companies. I am confident the campus will be a magnet for big ideas and will be an economic boost for Washington DC and the region,” says Jeff Zients, who was appointed chair of the Children’s National Board of Directors effective October 1, 2019. As a CEO and the former director of President Obama’s National Economic Council, Zients says that “When you bring together business, academia, health care and government in the right setting, you create a hotbed for innovation.”
Ranked 7th in National Institutes of Health research funding among pediatric hospitals, Children’s National continues to foster collaborations as it prepares to open its first 158,000-square-foot phase of its Research & Innovation Campus. These key partnerships will enable the hospital to fulfill its mission of keeping children top of mind for healthcare innovation and research while also contributing to Washington D.C.’s thriving innovation economy.
https://innovationdistrict.childrensnational.org/wp-content/uploads/2019/12/VT_CNRICampus_Rendering-sm.png300400Innovation Districthttps://innovationdistrict.childrensnational.org/wp-content/uploads/2023/12/innovationdistrict_logo-1-1030x165.pngInnovation District2019-12-11 10:18:202023-07-03 10:40:18Children’s National welcomes Virginia Tech to its new campus